
Abstract
This article aims to review the clinical management strategies available for the rare iridocorneal endothelial syndrome. The different clinical variations as well as the imaging techniques available to aid diagnosis are discussed. We then present the evidence available to help the reader to understand how the condition can be managed medically and also the important surgical aspects of treatment. This involves raised intraocular pressure management in addition to the visual management options of partial or full thickness keratoplasty. We hope that this review provides an exhaustive but also succinct review of the literature available on what is a rare and difficult condition to treat.
Introduction
Iridocorneal endothelial (ICE) syndrome is a rare and fascinating condition that can be challenging for ophthalmic surgeons to manage. It comprises a spectrum of three clinical entities: progressive essential iris atrophy, Cogan-Reese syndrome, and Chandler syndrome.Citation1 It is characterized by proliferative and structural abnormalities of the corneal endothelium, progressive obliteration of the iridocorneal angle, and iris anomalies such as atrophy and polycoria.Citation2 ICE syndrome is sporadic in presentation; it is usually unilateral and typically affects adult patients, females more often than males.
The purpose of this review is to highlight the difficulties associated with managing the condition, to discuss the evidence available for the clinical diagnosis and management of the condition.
Method of literature search
A PubMed search was performed using the search terms “ICE”, “Iridocorneal endothelial syndrome”, “Endothelial syndromes”, “Chandler syndrome”, “progressive iris atrophy” and “Cogan-Reese syndrome”. A full systematic review of the literature using the PubMed database was conducted up until 1/11/17. The articles used were written in English, with all articles accessed in full. Both review articles and original articles were used for this review.
Clinical diagnosis
ICE syndrome is characterized by proliferative and structural abnormalities of the corneal endothelium, progressive obstruction of the iridocorneal angle, and iris anomalies such as atrophy, correctopia, and polycoria. The consequences of these changes are corneal decompensation and secondary glaucoma, which represent the most frequent causes of visual loss in these patients.
Given the progressive nature of ICE syndrome and the wide spectrum of clinical presentations it is important to establish the diagnosis from similar conditions. Posterior polymorphous dystrophy (PPD) may show similar clinical features such as iridocorneal adhesions, membranes, and ectropion uveae which are typically associated with ICE syndrome. This can at times complicate diagnosis. PPD, in contrast to ICE syndrome, has a genetic component and is rarely progressive unlike ICE syndrome.Citation3
Specular microscopy can be used to differentiate between these two conditions. ICE cells are dark areas with a light central spot and a light peripheral zone. These are generally larger than normal endothelial cells, and occur in areas where the cornea appears to have a hammered silver appearance.Citation3 These cells are regarded as pathognomonic of ICE syndrome and are termed “ICE cells” along with the tissue they form termed “ICE tissue”Citation4 (). Four basic patterns of ICE cells have been described by previous authors.Citation4 More recent findings using in-vivo confocal microscopy have highlighted two main patterns of abnormal “epithelioid-like” endothelium, both characterized by marked hyperreflective nuclei and loss of regularity in cellular size and shape.Citation5–Citation10 Stromal nerve fibers in affected eyes were unusually thicker and distorted. It is suggested these signs can be examined to aid diagnosis, especially in edematous corneas.Citation6,Citation7
Figure 1 (A) Specular microscopy from a normal cornea. (B) Specular microscopy from a patient with iridocorneal endothelial syndrome.
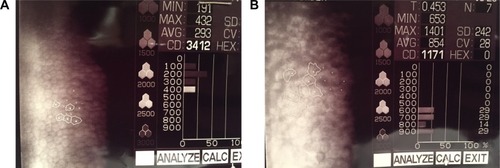
Anterior segment imaging in the form of ultrasound biomicroscopy or anterior segment optical coherence tomography (OCT) can be a useful tool for detecting peripheral anterior synechiae and iris atrophy more reliably than slit lamp microscopy and gonioscopy when corneal edema is present.Citation11 Central anterior chamber depth is shown to be significantly less in patients with ICE syndrome (mean 2.25 (± SD 0.32) mm) than in normal subjects (2.76 (±0.32) mm).Citation11 In contrast, PPD vesicles appear as dark rings with distinct, scalloped edges surrounding a lighter center.Citation3 With repeated specular microscopy examination over several years, the PPD cells showed no changes in configuration or migration. No accelerated endothelial cell loss occurred. In the ICE patients, normal endothelial cell density was lost, although the amount of ICE cells remained constant.Citation3 Both conditions show multilayered endothelial cells and thickened Descemet’s membrane.Citation12
Corneas affected by ICE syndrome are said to exhibit extensive endothelial changes early in the course of the disease, before other manifestations are clinically apparent.Citation2 Lymphocytes are often found in the endothelium, which may only be found early in the disease process.Citation2 Epithelialization of the endothelial cell layer has been demonstrated using immunohistochemical studies,Citation13 which results in cellular proliferation across the iridocorneal angle similar to that seen in epithelial downgrowth and posterior polymorphous endothelial dystrophy.Citation13 Abnormal iris profiles have been reported using anterior segment OCT scanning.Citation14
The ICE cells that border normal endothelial cells are said to be in a static, immobile state. These cells are often damaged or necrotic at boundary zones, suggesting that ICE cells may have a toxic effect on normal neighboring endothelial cells.Citation15,Citation16 This may explain why corneal failure in this syndrome is often slowly progressive.Citation17 Some evidence suggests that a subclinical form may exist in the contralateral eye,Citation18 predisposing to shallow or closed anterior chamber angles, which should be examined for gonioscopically.Citation11 Contralateral endothelial cells are not reduced, although normal hexagonal-shaped cells are reduced.Citation19
Three subtypes of the ICE syndrome exist, producing a spectrum of disease. These are progressive essential iris atrophy, Cogan-Reese syndrome, and Chandler syndrome.Citation1 Differentiating between these conditions is difficult clinically, and most distinctions are made based on different levels of iris abnormalities, with Chandler syndrome said to be the most common subtype.Citation20
Progressive iris atrophy involves significant iris atrophy often with hole formation. This is not diagnostic, however, as this can occur in the Cogan-Reese variant.Citation21 Gonioscopy may show the presence of peripheral anterior synechiae as a result of angle endothelialization. This causes variable degrees of angle closure and consequent intraocular pressure (IOP) increase. Iris heterochromia and ectropion uveae can occur rarely.Citation21
Cogan-Reese syndrome is characterized by proliferation of the corneal endothelium involving most of the iris and anterior chamber angle. This does not usually cause marked pupillary displacement. This subset involves the presence of multiple iris nodules, surrounded by iris stromal loss of crypts and a matted appearance. These nodules often develop late in the disease process and can appear as fine, yellowish nodules on the iris surface. Later in the disease course they become darker and larger.Citation1,Citation22
Chandler’s syndrome is said to have less iris involvement. Corneal edema, epithelial bullae, and a hammered silver appearance of the corneal endothelium. Mild iris atrophy can also occur but full thickness iris holes are rare.Citation23
Medical management
Due to the unknown etiology of ICE syndrome, medical management of this condition can be difficult, and is often a temporizing measure. No therapy is available which targets the pathogenesis of ICE syndrome, meaning medical treatment is aimed at controlling IOP and corneal clarity. Due to the progressive nature of the disease and the younger presenting age of ICE patients, often with preexisting glaucoma, medical management is usually insufficient.Citation24–Citation26 Older reports suggest surgical intervention is required in up to 88% of cases,Citation25 although these results were published prior to the advent of topical medications that are now ubiquitous. Newer data from an Indian cohort of 203 patients suggest 50% of patients require surgical intervention for IOP lowering and 14% require keratoplasy.Citation24 These rates are certainly subject to geographical factors and availability of both medical and surgical treatment modalities, but adequately illustrate the difficulty associated with managing this condition medically.
Topical medication can be used in order to control IOP, with the reduction of IOP helping to reduce the amount of corneal edema. Hypertonic saline and hairdryer use can be applied in conjunction, as would be advised for other conditions affected by corneal edema.Citation27 Aqueous suppressants are recommended as first-line agents, with prostaglandins suggested to be used cautiously due to the reported links between herpes viruses and ICE syndrome.Citation1,Citation28 Miotics are said to add little value, likely as a result of an abnormal iris.Citation1,Citation29
There is a suggestion within the literature that ICE syndrome has a viral etiology, after initial early reports of patients with concurrent anterior segment inflammation.Citation21,Citation30 One study reports polymerase chain reaction evidence of HSV DNA presence in 16 out of 25 (64%) ICE syndrome corneal specimens, potentially pointing toward a viral trigger or cause.Citation31 Epstein–Barr virus (EBV) and varicella zoster virus were not detected,Citation31 although other authors have suggested EBV may play a role after high titers of IgG antibodies to the EBV capsid antigen were found in ICE patients when compared with controls.Citation32 Despite these findings, there is no available evidence to suggest that antiviral therapy alters the progression of ICE syndrome.
Glaucoma surgical management
Surgical intervention for IOP control is often required, given the high failure rate of medical treatment.
Data are scarce within the literature in regard to trabeculectomy. Only retrospective studies and case reports exist, although these report moderate success with augmented trabeculectomy.Citation33–Citation36 The largest involves 16 eyes all undergoing primary trabeculectomy with mitomycin-C, between the dates of 1991 and 2013,Citation35 with no history of previous intraocular surgery. Median postoperative IOP was reduced significantly from 36 to 14 mmHg (P<0.001), with the median number of postoperative anti-glaucoma medications reduced from 3 to 0 (P<0.001). Complete success was defined as IOP ≤5 and ≥21 using no medications with the following outcomes reported: 75% at 6 months, 64% at 12 months, 57% at 36 months, and 33% at 60 months. These results are similar to those found in other cohorts,Citation34,Citation36 including one from Germany which showed a mean IOP of 12.1 mmHg, although the mean follow-up time was shorter (14.9 months).Citation36
Common complications include hypotony, although this appears to resolve with conservative management in both studies.Citation35,Citation36 Encouragingly, the majority of eyes appear to maintain good visual acuity, with 10%–31% of patients losing more than two Snellen lines,Citation35,Citation36 with the commonest reason for reduced vision being corneal edema as opposed to inadequate IOP control.Citation35 From the aforementioned study looking at 16 eyes, two required penetrating keratoplasty (PK) at 20 months and 59 months postoperatively.Citation35
It is important to note that a significant proportion of eyes undergoing trabeculectomy for ICE syndrome (12.5%–53.8%) require a secondary glaucoma drainage implant (GDI) at some stage, suggesting augmented trabeculectomy does not always offer definitive treatment.
GDI surgery seems to offer an adequate alternative means to lower IOP. Again, only retrospective studies exist which show 70% of eyes maintaining an IOP of <21 mmHg using additional topical medications after Baerveldt tube, Molteno valve, or Ahmed valve implantation.Citation34 Doe et alCitation34 report a better success rate of 66% without topical medication required for additional control. It is important to note that the vast majority of the eyes reported from these studies have previously undergone glaucoma surgery, usually in the form of enhanced trabeculectomy. In some cases, the surgery was performed 30 years ago using older techniques. The findings of these studies are therefore difficult to compare directly with the trabeculectomy outcomes above, as these are not primary procedures and may have higher levels of preoperative conjunctival fibrosis increasing the risk of failure. This may inadvertently select for more difficult or refractory cases, and more research is required for this to be determined. In both studies, significant proportions (50%Citation37 and 26.3%Citation34 respectively) of patients required tube revisions or further GDI implantation in an attempt to achieve adequate pressure control.Citation34,Citation37 About 20% of eyes were reported to have a recurrence of an ICE membrane after GDI, causing blockage of the tube.Citation37 50% of the eyes suffered corneal decompensation at mean follow-up of 55 months, despite some having undergone PK.Citation37
Filtering surgery is said to fail due to the continued growth of the endothelial membrane over the osteum site,Citation34,Citation38 which is often only apparent when examined histologically. Contraction and synechial closure of the ostium are also suspected.Citation34 Marked subconjunctival fibrosis has also been noted in trabeculectomy cases postoperatively, leading to speculation that these eyes may be predisposed to a more aggressive inflammatory response partly due to the fact that this disease tends to involve a younger patient cohort.Citation26,Citation34 One suggestion from the literature for GDI insertion in this cohort of patients is to route the tube along the sclera and to lengthen the tube in order to allow for repositioning.Citation34 These authors also suggest keeping the tube away from potential endothelial proliferation sites such as the iris and endothelium. Peripheral iridectomy could allow the tube to sit in the sulcal plane. Entry through the pars plana can be used in pseudophakic, aphakic, or vitrectomized eyes. Despite these suggestions, however, only one patient in this study was stated to have a tube placed into the vitreous cavity and unfortunately still suffered corneal decompensation.
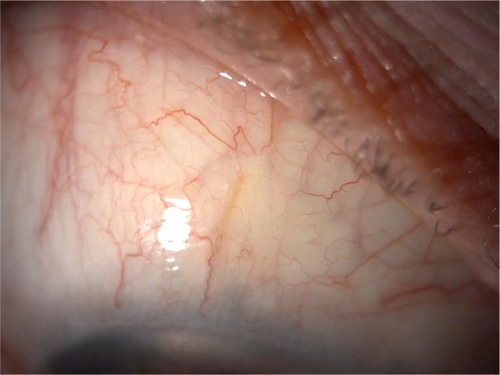
New minimally invasive glaucoma surgical devices offer an exciting option for future management of complex glaucoma such as ICE syndrome. Studies have shown the efficacy of Xen45 gel stents (allergan affiliate; AqueSys Inc., Aliso Viejo, CA, USA) in primary open angle glaucoma patients both in clinical trials and clinical practice.Citation39–Citation41 One case report exists reporting the successful implantation of a Xen45 stent in a patient with ICE syndrome who had also undergone prior Descemet’s membrane endothelial keratoplasty surgery (). Additional intraoperative and postoperative anti-VEGF injections were given to optimize postoperative scarring.Citation42 It would be reasonable to hypothesize that other angle-based surgery such as using the iStent (Glaukos Corp., San Clemente, CA, USA) and Hydrus stent (Ivantis, Irvine, CA, USA) may not be the intervention of choice, given the likely proliferation of endothelial cells over the stent opening, although no evidence currently exists to support this.
Figure 2 Xen45 stent (AqueSys Inc., Aliso Viejo, CA, USA) visible in the conjunctival space in a patient with iridocorneal endothelial syndrome.
Corneal surgical management
Although controlling IOP is crucial for maintaining long-term visual potential, ICE syndrome is associated with significant corneal symptoms as a result of the abnormal proliferation of an ectopic membrane over the anterior chamber angle. Lowering IOP was often the main intervention to reduce the rate of corneal decompensation.
There is a paucity of literature in regard to keratoplasty techniques in this syndrome, although replacement of the full corneal thickness with PK has been shown to be an effective treatment for corneal symptoms in early case series.Citation43–Citation45 The largest case series provides 5-year follow-up data on 14 ICE eyes undergoing PK. Repeat grafts in six eyes were required, although 12 of the 14 had clear corneas at the end of follow-up. This fits with findings from other data sets, as ICE syndrome has been reported alongside stromal dystrophies as being the commonest indication for undergoing three or more corneal transplants.Citation46 From the data provided in the above cohort, it is reassuring to see that all of the eyes either improved or maintained their preoperative visual acuity. About 50% of eyes had a visual acuity of better than 20/100, with three having better than 20/40.Citation43 Allograft rejection rates were high, however, with 11 eyes having primary graft rejection episodes.Citation43 This agrees with the findings of other authors, who report similar visual outcomes with PK.Citation45,Citation47 An interesting suggestion was that simultaneous extracapsular cataract extraction did not result in a poorer visual prognosis of the graft.Citation47 Older series also show PK to be effective at reducing morbidity from pain caused by bullous epithelial disease.
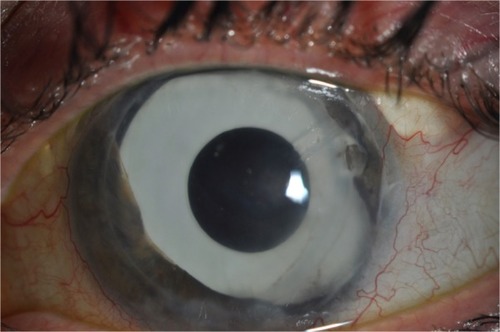
With the advances in lamellar corneal surgery, endothelial keratoplasty has been shown to be a viable option for ICE patients. Descemet stripping automated endothelial keratoplasty (DSAEK) may be theoretically advantageous for many reasons, but has the potential to be more technically challenging in this group of patients due to peripheral anterior synechiae formation, shallow anterior chambers, and iris abnormalities meaning graft positioning can be difficult ().Citation48,Citation49 Different techniques have been suggested as a means to overcoming this, including suture dragging techniques,Citation50 donor fixation,Citation49 and pupilloplasties.Citation51 However, most of the procedures reported in the literature use standard techniquesCitation48,Citation49,Citation52 and, despite this, graft dislocation rates requiring rebubbling in 22%Citation49 of eyes are comparable with non-ICE procedures.Citation53 Again, only small retrospective patient cohort reviews exist, but it is reassuring to see that good initial visual outcomes are reported from multiple centers around the world.Citation49,Citation52,Citation54–Citation57 Many studies fail to report follow-up periods beyond 24 months and lack data on endothelial cell counts.Citation52,Citation54,Citation56,Citation57 Authors from India report good visual outcomes and corneal clarity at a mean follow-up period of 1 year using automated endothelial graft techniques.Citation54 It is important to note that more than half of these patients had a postoperative IOP rise that required oral medication to control, which can be problematic in a group of patients with preexisting glaucomatous damage. Only one patient was noted to have optic nerve changes due to glaucoma, although the follow-up period was short.Citation54 No comment is made on the rejection profile of these transplants.
Figure 3 Broad peripheral anterial synechiae seen in iridocorneal endothelial syndrome.

A smaller cohort with longer follow-up shows the rejection profile of DSAEK grafts to be high, with 50% of the eyes having a rejection episode,Citation49 which is higher than the reported rejection rate of non-ICE patients from larger series.Citation58 Corneal clarity and visual acuity were not well maintained beyond the 12-month mark, where only 12% of the grafts had a best corrected visual acuity of 6/12. 77.7% of the grafts failed at a mean age of 18 months in conjunction with a reduction in endothelial cell count and increased central corneal thickness.Citation49 The endothelial cell loss appears to be rapid in ICE patients when compared with a DSEK cohort performed for mainly for pseudophakic or aphakic bullous keratopathy (79% vs 38% cell loss at 6 months respectively).Citation49,Citation59 Both groups of patients had undergone previous glaucoma surgery, which is known to be an independent factor for cell loss after corneal transplantation,Citation59,Citation60 suggesting there is a component of the ICE pathophysiology that causes grafts to fail more rapidly than in other conditions.
Due to the rarity of ICE syndrome and the availability of data within the literature, it is difficult to say with certainty whether partial thickness or full lamellar transplantation is favorable in this condition. Direct comparison of individual studies is difficult due to differences in available data and small patient numbers, meaning statistical significance is hard to ascertain. Only one study using data from Singapore exists comparing PK with DSAEK. Kaplan–Meier survival analysis showed no significant difference between either group with a mean follow-up period of nearly 6 years. This study echoes the findings of other authorsCitation49 which suggest the PK survival rate is longer than that of DSAEK (9 vs 4.6 years respectively).Citation48 Two PKs (11.7%) had rejection episodes leading to graft failure, while none were reported in the DSAEK group. Overall, around 40% of eyes required treatment for raised IOP, with no statistical difference found between the two groups. The double-edged sword of glaucoma surgery is nicely represented by the results from this study.Citation48 On the one hand, those eyes that had undergone previous glaucoma surgery were significantly less likely to require escalation of IOP-lowering therapy post keratoplasty (9.1% vs 50%, P=0.034). However, these grafts were more likely to fail (50% vs 32.6%, P=0.432), although the difference did not reach statistical significance. No significant difference between a glaucoma drainage device and trabeculectomy groups was found in terms of survival.
Nonetheless, DSAEK appears to offer rapid and better visual rehabilitation with reduced astigmatic effect,Citation49,Citation52 albeit with survival times of generally less than 24 months. Although there is potential for regrafting post DSAEK, the concept of repeating surgery every 2 years is far from ideal. Rejection rates appear to be lower in ICE patients undergoing DSAEK vs PK (33% vs 79% respectively),Citation43,Citation49 which despite being more frequent in this subgroup of patients is consistent with findings from other studiesCitation49,Citation58 ().
Figure 4 A patient who has undergone multiple procedures for iridocorneal endothelial syndrome. A clear Descemet stripping automated endothelial keratoplasty graft is visible, with a supertemporal Baerveldt tube in situ. A prosthetic iris implant can also be seen.
Older, pre-DSAEK techniques such as deep lamellar endothelial keratoplasty have reported similar visual outcomes to those mentioned above.Citation61 No cases of graft failure were reported, although the maximum follow-up period was only 20 months.Citation61 Deep lamellar endothelial keratoplasty requires the excision of host stroma as opposed to just a descemetorhexis. This can be time consuming and prolongs visual recovery but can be advantageous in phakic eyes with shallower anterior chambers, allowing the donor button to be inserted more easily.
Although lamellar surgery is evolving rapidly, few cases are reported using Descemet’s membrane endothelial keratoplasty for ICE syndrome.Citation42,Citation62 This technique has many potential advantages and may provide benefits in the future. One paper describes the technique being used successfully in three cases, all of which had an improved best corrected visual acuity and reduction in corneal thickness.Citation62 Two of the three cases required rebubbling of the graft, although advances in intraoperative OCT may help to improve postoperative graft adherence in the future.Citation63
Boston type 1 keratoprosthesis is an option in patients who have had failed allogenic transplants.Citation64 Four cases have been reported, three of which had an improved visual acuity of 6/30 Snellen equivalent 4 years postoperatively, with all grafts being retained in situ. As expected, glaucomatous progression is a known complication along with retroprosthetic membrane formation,Citation64 both of which may require surgical intervention.Citation61
Cosmetic and diplopic interventions
Patients with ICE syndrome may develop a myriad of iris changes, which can vary as the syndrome persists over time. These may manifest as stromal atrophy, corectopia, pseudopolycoria, and the induced nodular irregularity of iris nevus syndrome. If the pupil is displaced, or the stroma is insufficient to absorb light, glare and other unwanted optical phenomena such as monocular diplopia may occur. One report shows how combined cataract extraction and iris reconstruction using a multipiece endocapsular iris prosthesis can help to alleviate symptoms and improve cosmesis.Citation65 Suturing techniques may not be possible due to the friable nature of the iris.Citation66 Visual acuity postoperatively was 6/9 Snellen equivalent with a reduction in glare. It is worth noting that this patient had undergone previous trabeculectomy and glaucoma drainage device insertion, and IOP remained stable postoperatively.
Femtosecond-assisted corneal keratopigmentation (tattooing) is a new technique that has been proposed for cosmetic improvement of opaque corneasCitation67 for cosmetic purposes. This technique has been used to aid functional eye disability related to a severe iris and pupil defect from ICE syndrome. Femtosecond laser technology allows tattoos to be created using intralamellar dissections. It is necessary to enter into the anterior chamber in order to remove atrophic parts of iris that are obscuring the visual axis. Excellent visual acuity is reported postoperatively.Citation68
Conclusion
This review highlights the complexities associated with managing patients with ICE syndrome. There is clearly no one single intervention that can treat the condition for an entire lifetime. Due to the rarity of the syndrome and the associated lack of high level evidence it is difficult to ascertain the best strategy for managing these patients. What is clear is that many patients will require multiple interventions in order to control IOP and corneal clarity. It may be wise to control IOP before tackling visual enhancement in order to promote long-term visual outcomes. However, as discussed above, previous glaucoma procedures result in poorer corneal transplantation outcomes. The minimally invasive glaucoma surgical devices may offer less invasive approaches to control IOP, with the potential to be less problematic for the cornea. Ultimately, frank discussion with the patient is required early on into the disease process so that appropriate expectations are set. This helps to guide the patient and clinician as to which future interventions are chosen.
Disclosure
The authors report no conflicts of interest in this work.
References
- SacchettiMMantelliFMarencoMMacchiIAmbrosioORamaPDiagnosis and management of iridocorneal endothelial syndromeBiomed Res Int2015201576309326451377
- LevySGKirknessCMMossJFickerLMcCartneyACOn the pathology of the iridocorneal-endothelial syndrome: the ultrastructural appearances of “subtotal-ice”Eye (Lond)19959Pt 33183237556740
- LaganowskiHCSherrardESMuirMGBuckleyRJDistinguishing features of the iridocorneal endothelial syndrome and posterior polymorphous dystrophy: value of endothelial specular microscopyBr J Ophthalmol19917542122162021586
- SherrardESFrangoulisMAMuirMGBuckleyRJThe posterior surface of the cornea in the irido-corneal endothelial syndrome: a specular microscopical studyTrans Ophthalmol Soc U K1985104Pt 77667743868217
- GaribaldiDCScheinODJunAFeatures of the iridocorneal endothelial syndrome on confocal microscopyCornea200524334935115778613
- LeQHSunXHXuJJIn-vivo confocal microscopy of iridocorneal endothelial syndromeInt Ophthalmol2009291111818297250
- ChiouAGKaufmanSCBeuermanRWOhtaTYaylaliVKaufmanHEConfocal microscopy in the iridocorneal endothelial syndromeBr J Ophthalmol199983669770210340979
- SheppardJDJrLattanzioFAJrWilliamsPBMitrevPVAllenRCConfocal microscopy used as the definitive, early diagnostic method in Chandler syndromeCornea200524222722915725894
- LevySGMcCartneyACSawadaHDopping-HepenstalPJAlexanderRAMossJDescemet’s membrane in the iridocorneal-endothelial syndrome: morphology and compositionExp Eye Res19956133233337556496
- HowellDNDammsTBurchetteJLJrGreenWREndothelial meta-plasia in the iridocorneal endothelial syndromeInvest Ophthalmol Vis Sci1997389189619019286281
- ZhangMChenJLiangLLatiesAMLiuZUltrasound biomicros-copy of Chinese eyes with iridocorneal endothelial syndromeBr J Ophthalmol2006901646916361670
- BromleyJGRandlemanJBStoneDStultingRDGrossniklausHEClinicopathologic findings in iridocorneal endothelial syndrome and posterior polymorphous membranous dystrophy after Descemet stripping automated endothelial keratoplastyCornea20123191060106422333668
- HirstLWBancroftJYamauchiKGreenWRImmunohistochemical pathology of the corneal endothelium in iridocorneal endothelial syndromeInvest Ophthalmol Vis Sci19953658208277706030
- HollóGNaghizadehFOptical coherence tomography characteristics of the iris in Cogan-Reese syndromeEur J Ophthalmol201424579779924729138
- HaemmerliGFelixHShape and motility, two interdependent featuresScan Electron Microsc1982Pt 27317396962996
- PolliackAGordonSScanning electron microscopy of murine macrophages. Surface characteristics during maturation, activation, and phagocytosisLab Invest19753354694771186128
- BourneWMBrubakerRFProgression and regression of partial corneal involvement in the iridocorneal endothelial syndromeAm J Ophthalmol199211421711811642292
- MalhotraCPandavSSGuptaAJainAKPhenotypic heterogeneity of corneal endothelium in iridocorneal endothelial syndrome by in vivo confocal microscopyCornea201433663463724727634
- Lucas-GlassTCBaratzKHNelsonLRHodgeDOBourneWMThe contralateral corneal endothelium in the iridocorneal endothelial syndromeArch Ophthalmol1997115140449006423
- WilsonMCShieldsMBA comparison of the clinical variations of the iridocorneal endothelial syndromeArch Ophthalmol198910710146514682803093
- ScheieHGYanoffMIris nevus (Cogan-Reese) syndrome. A cause of unilateral glaucomaArch Ophthalmol197593109639701180755
- EagleRCJrFontRLYanoffMFineBSProliferative endotheliopathy with iris abnormalities. The iridocorneal endothelial syndromeArch Ophthalmol1979971121042111508177
- ChandlerPAAtrophy of the stroma of the iris, endothelial dystrophy, corneal edema, and glaucomaTrans Am Ophthalmol Soc1955537589 discussion, 89–9313360867
- ChandranPRaoHLMandalAKChoudhariNSGarudadriCSSenthilSGlaucoma associated with iridocorneal endothelial syndrome in 203 Indian subjectsPLoS One2017123e017188428282413
- KiddMHetheringtonJMageeSSurgical results in iridocorneal endothelial syndromeArch Ophthalmol198810621992013341974
- LaganowskiHCKerr MuirMGHitchingsRAGlaucoma and the iridocorneal endothelial syndromeArch Ophthalmol199211033463501543451
- SiuGDYoungALJhanjiVAlternatives to corneal transplantation for the management of bullous keratopathyCurr Opin Ophthalmol201425434735224807064
- SaleemAAAliMAkhtarFIridocorneal endothelial syndromeJ Coll Physicians Surg Pak201424Suppl 2S112S11424906259
- WandMGilbertCMLiesegangTJLatanoprost and herpes simplex keratitisAm J Ophthalmol1999127560260410334356
- ShieldsMBProgressive essential iris atrophy, Chandler’s syndrome, and the iris nevus (Cogan-Reese) syndrome: a spectrum of diseaseSurv Ophthalmol1979241320483159
- AlvaradoJAUnderwoodJLGreenWRDetection of herpes simplex viral DNA in the iridocorneal endothelial syndromeArch Ophthalmol199411212160116097993217
- TsaiCSRitchRStrausSEPerryHDHsiehFYAntibodies to Epstein-Barr virus in iridocorneal endothelial syndromeArch Ophthalmol199010811157215762173898
- JainVKSharmaROjhaSTrabeculectomy with mitomycin-C in patients with iridocorneal endothelial syndrome: a case seriesJ Clin Diagn Res2016105NR05NR0627437260
- DoeEABudenzDLGeddeSJImamiNRLong-term surgical outcomes of patients with glaucoma secondary to the iridocorneal endothelial syndromeOphthalmology2001108101789179511581050
- ChandranPRaoHLMandalAKChoudhariNSGarudadriCSSenthilSOutcomes of primary trabeculectomy with mitomycin-C in glaucoma secondary to iridocorneal endothelial syndromeJ Glaucoma2016257e652e65625943731
- LanzlIMWilsonRPDudleyDAugsburgerJJAslanidesIMSpaethGLOutcome of trabeculectomy with mitomycin-C in the iridocorneal endothelial syndromeOphthalmology2000107229529710690828
- KimDKAslanidesIMSchmidtCMJrSpaethGLWilsonRPAugsburgerJJLong-term outcome of aqueous shunt surgery in ten patients with iridocorneal endothelial syndromeOphthalmology199910651030103410328409
- ShieldsMBMcCrackenJSKlintworthGKCampbellDGCorneal edema in essential iris atrophyOphthalmology197986815331550396496
- SheybaniALenzhoferMHohensinnMReitsamerHAhmedIIPhacoemulsification combined with a new ab interno gel stent to treat open-angle glaucoma: pilot studyJ Cataract Refract Surg20154191905190926482822
- SheybaniADickHBAhmedIIEarly clinical results of a novel ab interno gel stent for the surgical treatment of open-angle glaucomaJ Glaucoma2016257e691e69626561420
- TanSZWalkdenAAuLOne-year result of XEN45 implant for glaucoma: efficacy, safety, and postoperative managementEye (Lond)201832232433228862254
- HohbergerBWelge-LüenUCLämmerRICE-syndrome: a case report of implantation of a microbypass Xen gel stent after DMEK transplantationJ Glaucoma2017262e103e10427841796
- AlvimPTCohenEJRapuanoCJPenetrating keratoplasty in iridocorneal endothelial syndromeCornea200120213414011248814
- BuxtonJNLashRSResults of penetrating keratoplasty in the iridocorneal endothelial syndromeAm J Ophthalmol19849832973016383056
- CrawfordGJStultingRDCavanaghHDWaringGO3rdPenetrating keratoplasty in the management of iridocorneal endothelial syndromeCornea19898134402647408
- YildizEHHoskinsEFramNThird or greater penetrating keratoplasties: indications, survival, and visual outcomesCornea201029325425920118784
- ChangPCSoongHKCoutoMFMeyerRFSugarAPrognosis for penetrating keratoplasty in iridocorneal endothelial syndromeRefract Corneal Surg1993921291328494813
- QuekDTWongCWWongTTGraft failure and intraocular pressure control after keratoplasty in iridocorneal endothelial syndromeAm J Ophthalmol20151603422.e1429.e126032193
- FajgenbaumMAHollickEJDescemet stripping endothelial keratoplasty in iridocorneal endothelial syndrome: postoperative complications and long-term outcomesCornea201534101252125826203744
- BradleyJCMcCartneyDLDescemet’s stripping automated endothelial keratoplasty in intraoperative floppy-iris syndrome: suture-drag techniqueJ Cataract Refract Surg20073371149115017586368
- GroatBYingMSVromanDTFernández de CastroLEDescemet-stripping automated endothelial keratoplasty technique in patients with anterior chamber intraocular lensesBr J Ophthalmol2007916714
- PriceMOPriceFWJrDescemet stripping with endothelial keratoplasty for treatment of iridocorneal endothelial syndromeCornea200726449349717457204
- LeeWBJacobsDSMuschDCKaufmanSCReinhartWJShteinRMDescemet’s stripping endothelial keratoplasty: safety and outcomes: a report by the American Academy of OphthalmologyOphthalmology200911691818183019643492
- ChaurasiaSRamappaMGargPMurthySISenthilSSangwanVSEndothelial keratoplasty in the management of iridocorneal endothelial syndromeEye (Lond)201327456456623348727
- MohamedAChaurasiaSMurthySIEndothelial keratoplasty: a review of indications at a tertiary eye care centre in South IndiaAsia Pac J Ophthalmol (Phila)20143420721026107758
- BaharIKaisermanIBuysYRootmanDDescemet’s stripping with endothelial keratoplasty in iridocorneal endothelial syndromeOphthalmic Surg Lasers Imaging2008391545618254352
- KymionisGDKontadakisGAAgorogiannisGIBennettMAngelidouFDescemet stripping automated endothelial keratoplasty combined with phacoemulsification in Chandler syndromeEur J Ophthalmol201121449549721218389
- EzonIShihCYRosenLMSutharTUdellIJImmunologic graft rejection in descemet’s stripping endothelial keratoplasty and penetrating keratoplasty for endothelial diseaseOphthalmology201312071360136523531352
- AnshuAPriceMOPriceFWDescemet’s stripping endothelial keratoplasty: long-term graft survival and risk factors for failure in eyes with preexisting glaucomaOphthalmology2012119101982198722705345
- AldaveAJChenJLZamanASDengSXYuFOutcomes after DSEK in 101 eyes with previous trabeculectomy and tube shunt implantationCornea201433322322924322807
- HuangTWangYJiJGaoNChenJDeep lamellar endothelial keratoplasty for iridocorneal endothelial syndrome in phakic eyesArch Ophthalmol20091271333619139335
- WellerJMTourtasTKruseFEFeasibility and outcome of Descemet membrane endothelial keratoplasty in complex anterior segment and vitreous diseaseCornea201534111351135726382893
- SiebelmannSBachmannBLappasAIntraoperative optical coherence tomography in corneal and glaucoma surgical proceduresOphthalmologe2016113864665027436117
- PhillipsDLGoinsKMGreinerMAAlwardWLKwonYHWagonerMDBoston type 1 keratoprosthesis for iridocorneal endothelial syndromesCornea201534111383138626398156
- KhngCSnyderMEIris reconstruction with a multipiece endocapsular prosthesis in iridocorneal endothelial syndromeJ Cataract Refract Surg200531112051205416412914
- BurkSEDa MataAPSnyderMECionniRJCohenJSOsherRHProsthetic iris implantation for congenital, traumatic, or functional iris deficienciesJ Cataract Refract Surg200127111732174011709244
- KimJHLeeDHahnTWChoiSKNew surgical strategy for corneal tattooing using a femtosecond laserCornea2009281808419092411
- AlióJLRodriguezAEToffahaBTPiñeroDPMorenoLJFemtosecond-assisted keratopigmentation for functional and cosmetic restoration in essential iris atrophyJ Cataract Refract Surg201137101744174721865008