Abstract
Background
Follicular lymphomas of the ocular adnexa are very rare in Japan, with only two reported cases.
Case
A 44-year-old woman visited our clinic for treatment of ocular adnexal tumors in both eyes.
Findings
Histologic examination showed that the neoplastic lesions consisted of atypical lymphoid cells, and the tentative diagnosis was malignant lymphoma. Immunophenotypic analyses by flow cytometry and immunohistochemistry showed that the atypical lymphoid cells expressed CD45, bcl-2, CD10, CD19, CD20, IgM, and kappa light chains. The cells were negative for CD5 and other T, natural killer, or myelomonocyte antigens. Southern blot hybridization demonstrated gene rearrangement bands in the immunoglobulin JH region. Fluorescence in situ hybridization studies showed a translocation at t(14,18)(q32,q21). Systemic evaluations detected enlargements of both the inguinal lymph nodes and parabronchial lymph nodes.
Conclusion
Our results show that flow cytometry, molecular genetic analyses, and chromosomal examination can be useful in differentiating follicular lymphoma from marginal zone B cell lymphoma of mucosa-associated lymphoid tissue and reactive lymphoid hyperplasia.
Introduction
The classification of lymphomas has been controversial, and the Non-Hodgkin’s Lymphoma Pathologic Classification ProjectCitation1 has classified lymphomas by morphologic characteristics, eg, cell size, cell shape, and growth pattern. This classification was developed before immunologic or genetic techniques were available, and it created heterogenous diagnostic categories. This then resulted in relatively low reproducibility in the diagnosis among pathologists. Since the early 1980s, it has become apparent that the use of more accurate characterizations of diseases would reduce the subjectivity of morphologic diagnosis and improve the rate of correct diagnosis. Thus, increasing the information about the biology of malignant lymphomas has led to significantly better diagnosis of diseases, and newer methods, such as immunohistochemistry and molecular biology, now being used routinely in pathology laboratories.
The classification of lymphoid tumors was improved in the Revised European-American Lymphoma (REAL) classification,Citation2 which was presented by the International Lymphoma Study Group in 1994. This classification was based on an update of the original Kiel classifications.Citation3,Citation4 This formed the basis of the new World Health Organization (WHO) classification of lymphomas in 2008,Citation5 the latest classification of lymphoma, which is based upon the foundations laid within REAL.
The majority of lymphomas occurring in the ocular adnexa are B cell non-Hodgkin’s lymphomas. These are predominantly marginal zone B cell lymphomas of mucosa-associated lymphoid tissues according to the new WHO classification. According to the WHO, lymphomas that occur in the ocular adnexa are the third most common B cell lymphomas occurring in Western Europe and North America.
Follicular lymphomas of the ocular adnexa are very rare in Japan and the other Asian countries.Citation6 They are quite difficult to diagnose by their morphology alone because their low prevalence means that most physicians have not had first-hand experience of follicular lymphoma. With the introduction of newer examination techniques, such as flow cytometry, molecular genetic analyses, and chromosomal examinations, the differential diagnosis of follicular lymphomas has become easier and more accurate.
We report a 44-year-old woman who was diagnosed with follicular lymphoma involving the ocular adnexa by flow cytometry, molecular genetic analyses, and chromosomal examinations.
Case history
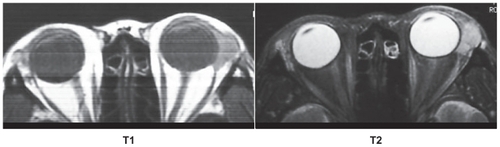
A 44-year-old woman visited the Tohoku University Hospital in March 2003 complaining of painless left upper eyelid swelling. She had no relevant medical history, although her father had stomach cancer. The initial ocular examination showed that her best-corrected visual acuity was 20/20 in each eye, and her eye movements were full in both eyes. Examination of the anterior and posterior segments of both eyes was normal. Magnetic resonance imaging scans of both orbits showed a well-defined 15 × 10 × 10 mm tumor in the region of the left lacrimal gland and a 3 × 5 × 3 mm tumor in the right lacrimal gland (). A gallium scintigram showed high uptake spots corresponding to the ocular adnexal tumors and also in both inguinal lymph nodes.
Figure 1 Magnetic resonance imaging scans of both orbits showing a well defined 15 × 10 × 10 mm tumor in the region of the left lacrimal gland and a 3 × 5 × 3 mm tumor in the right lacrimal gland. Signals higher than that of the external muscles in T1 image (right), and about the same intensity as brain cortex in the T2 image (left).
At that point, we tentatively diagnosed her with malignant lymphoma. Laboratory examinations showed serum lactate dehydrogenase of 310 IU/L (normal = 119–229) and 465 U/mL of soluble interleukin-2 receptor (normal = 127–582).
In April 2003, a biopsy of the left ocular adnexal tumor was performed by an anterior percutaneous approach, and the tissue was forwarded to the registration-examination-analysis-description (READ) system, which is a comprehensive diagnostic laboratory for lymphoproliferative disorders (Koutou Biseibutsu Laboratories and Special Reference Laboratories, Tokyo, Japan). The results of their histologic examinations and other analyses of the biopsied tissues led to a diagnosis of follicular lymphoma.
The patient was referred to the Hematology Department for consultation, staging of the tumors, and further treatment. The staging investigations included full blood count, chest x-rays, computed tomography (CT) of the thorax, abdomen, head, and neck, and bone marrow biopsy. CT scans revealed enlargements of both the inguinal lymph nodes and parabronchial lymph nodes. Bone marrow biopsy was negative for lymphoma infiltration, and the patient was reported to be at Stage IIIA by the Ann Arbor clinical staging system.
The patient was treated with three cycles of chemotherapy consisting of cyclophosphamide, hydroxydaunorubicin (Adriamycin®), vincristine (Oncovin®), and CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) combined with rituximab. Rituximab is a synthetic antibody that was developed using cloning and recombinant DNA technology of human and mice genes. This therapy led to a regression of the tumors and the lymphadenopathy. At the time of the last medical examination in July 2010, the patient remained in complete remission.
Materials and methods
Histologic analysis
The biopsied tissues were fixed in 20% formalin and embedded in paraffin. Sections were stained with hematoxylin and eosin, and immunochemical staining was performed with monoclonal antibodies to bcl-2, CD3, CD10, CD20, and CD21 (Dako Japan Co, Ltd, Kyoto, Japan).
Flow cytometry
Single-cell suspensions were prepared by cutting and teasing unfixed tissues in phosphate-buffered saline. The washed cells were incubated with the different monoclonal antibodies and then injected into a Cytron Absolute flow cytometer (Ortho Diagnostic Systems, Raritan, NJ).
Cytogenetic analyses
Cells were cultured overnight in RPMI1640 with 15% fetal calf serum without mitogenic stimulation. The G-banded metaphases of the cells were determined by trypsin-treated Giemsa stain or hybridized with chromosomal specific fluorescence probes and then karyotyped.
Fluorescence in situ hybridization
Double-labeled, two-color fluorescence in situ hybridization (FISH) was performed on cells fixed in Carnoy’s fixative. The primers used were Vysis LSI IGH/BCL2 Dual Color, Dual Fusion Translocation Probe (probe for 14q32 region Immunoglobulin Heavy Chain Locus and 18q21), and Vysis LSI API2/MALT1 t(11;18)(q21;q21) Dual Color, Dual Fusion Translocation Probe (probe for 11q21 region and 18q21 region, Abbott Laboratories, Abbott Park, IL). The chromosomal probes were labeled by nick translation. After hybridization, the probes were detected by incubation for IgH gene and BCL2 gene. Nuclei were identified by 4–6-diamidino-2-phenylindole stain. The fluorescent signals were examined under a Nikon microscope (Nikon, Japan).
Southern blot analyses
High molecular weight genomic DNA was extracted from the tissues. Ten micrograms of digested DNA was electrophoresed, blotted on a nylon membrane, and then hybridized with a 32P-labeled probe for the JH gene of the immunoglobulin heavy (μ) chain. After washing, the membrane was dried and exposed to x-ray film.
Results
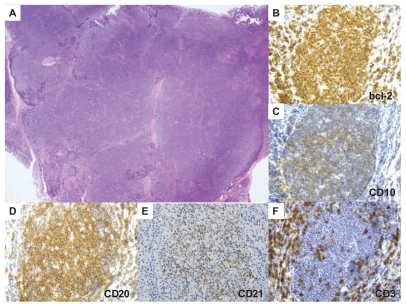
Histologic examination of the biopsied tissues showed diffuse proliferation of atypical cells with occasional follicular pattern (). The cells resembled small lymphocytes and more like marginal zone cells than centrocytes. The follicular dendritic cell meshwork was relatively dispersed rather than condensed. Immunohistochemical analysis showed that the tumor cells expressed bcl-2, CD10, CD20, and CD21. CD10 stained only a small proportion of the cells in the nodule. The presence of CD21-positive follicular dendritic cells was consistent with the follicle-like structure, and these cells were recognized as CD3-positive T cells ().
Figure 2 Histologic and immunohistochemical analyses. A) Hematoxylin and eosin image. There is a diffuse proliferation of atypical cells with occasional follicular pattern. B–F) Immunohistochemical images. The tumor cells expressed bcl-2 (B) and CD10 stains only a small proportion of the cells in the nodule (C), CD20 (D), and CD21 (E). A follicular pattern can be seen with CD3+ T cells (F). A) magnification × 2; B–F), magnification × 40.
Flow cytometry analyses showed that the atypical lymphoid cells expressed CD45, bcl-2, CD10, CD19, and CD20, IgM, and kappa, and were negative for CD5 and other T, natural killer, and myelomonocyte antigens (data not shown).
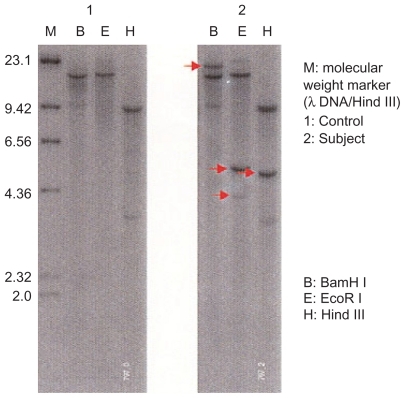
G-banded chromosome analyses were performed on 12 cells in metaphase, and a clonal cytogenetic abnormality, a 48, XX,+X,add18(q21),+add(18)[11]/46,XX[1], was identified in 11 of 12 cells (). Although the abnormality included the 18q21 locus, its partner allele locus of translocation was not clear for unknown reasons. However, the fusion FISH assay showed yellow signals which consisted of the fusion of green (IgH gene) and red (BCL2 gene) signals which suggested a t(14,18)(q32,q21) translocation. This was detected in 49/50 cells (). No split signal was detected with split FISH assay for the MALT1 gene and cyclin D1 gene (data not shown). Southern blot analysis showed monoclonal rearranged bands in the immunoglobulin JH region ().
Figure 3 G-banded cytogenetic and spectral karyotyping. G-banded metaphase analysis revealed a 48,XX,+X,add18(q21),+add(18)[11]/46,XX[1] karyotype.
![Figure 3 G-banded cytogenetic and spectral karyotyping. G-banded metaphase analysis revealed a 48,XX,+X,add18(q21),+add(18)[11]/46,XX[1] karyotype.](/cms/asset/5d8f00c7-caa5-4c31-93dc-1fdceaf37e34/doph_a_15219_f0003_b.jpg)
Figure 4 Analysis using fluorescence in situ hybridization demonstrated fusion yellow signals consisting of green (IgH gene) and red (BCL2 gene) signals, which directly suggested a t(14,18)(q32,q21) translocation, in 49/50 cells.

Figure 5 Southern blot analysis. Monoclonal rearranged bands were detected in the immunoglobulin JH region.
Discussion
Differentiating mantle cell lymphoma, marginal zone lymphoma, and follicular lymphoma is difficult because the differentiating characteristics are based on morphologic features, such as cell size, cell shape, and growth pattern in tissues stained with hematoxylin and eosin. Thus, mantle cell lymphoma, marginal zone lymphoma, and follicular lymphoma were placed in the same group with the same morphologic features. With the development of new techniques, such as genetic, molecular, and immunological methods, the differentiation is easier and more accurate. The 4th edition of the World Health Organization classification of tumors of hematopoietic and lymphoid tissuesCitation5 reported some new subtypes or variants of follicular lymphoma with distinct clinicopathologic and molecular genetic characteristics. Some of the early or precursor lesions of follicular lymphomas in situ are discussed.
The differentiation of follicular lymphoma from mantle cell lymphoma, marginal zone lymphoma, and reactive lymphoid hyperplasia is important because these lymphomas exhibit different clinical behaviors and outcomes. The results of G-banded cytogenetics of our case showed chromosomal abnormality in chromosome 18q21, but no translocation partner was identified in any chromosome including the IgH/14q32 locus. However, FISH analyses using probes for BCL2 and IgH provided direct evidence for their translocation. Our case was genetically characterized by a t(14,18)(q32,q21) translocation. This is particularly relevant because the IgH/BCL2 translocation has also been reported in extranodal mucosa-associated lymphoid tissue lymphomas in the stomachCitation6–Citation8 and skin.Citation9 In addition, a MALT1 gene abnormality and IgH/cyclin D1 gene fusion was not detected in the FISH analysis. Therefore, we diagnosed the tumors as a follicular lymphoma.
In diseases such as the chronic lymphoproliferative disorders which are characterized by a very low proportion of mitotically active abnormal cells, traditional cytogenetic analysis is more likely to identify the karyotype of the normal dividing cells, and may miss the rare abnormal cell in mitosis. FISH can identify abnormalities missed by conventional cytogenetics and is helpful in the diagnosis, prognosis, and evaluation of therapy for chronic lymphoproliferative disorders such as chronic lymphocytic leukemia.Citation10 FISH appears to be a more useful technique than other techniques and can provide the most reliable and accurate data. Immunohistochemical positivity for CD10 in the follicular lymphoma cells and their relationship with the BCL2 gene in FISH could be good evidence to diagnose our case as follicular lymphoma. On the other hand, a lack of an association with the cyclinD1 gene was evidence to exclude mantle cell lymphoma. In addition, no association with the MALT1 gene and the relationship with the BCL2 gene in FISH would be evidence to exclude marginal zone lymphoma. Dierlamm et al showed that the API2 gene, and a novel gene on 18q21, characterized by several Ig-like C2-type domains named MLT, are recurrently rearranged in t(11;18). They suggested that the t(11;18)(q21;q21) appeared to be the key genetic lesion and is found in approximately 50% of cytogenetically abnormal low-grade mucosa-associated lymphoid tissue lymphomas.Citation11
Thus, we diagnosed our case as follicular lymphoma from a combination of the results of all of these tests.
Follicular lymphomas are found less frequently in Asian countries than in Western countries (11%–33%),Citation12 with lower rates having been found in Japan (6.7%–18%),Citation13,Citation14 Korea (5.88%),Citation15 Hong Kong (8%),Citation16 Taiwan (14%),Citation17 and Thailand (3.8%–11.1%).Citation18,Citation19 The incidence of follicular lymphoma in Japan is less than 30% of the cases in Western countries. Notably, the incidence of follicular lymphoma in mainland Europe (11%–18%) is substantially less than that in North America and the UK. The reason for these differences is not known. Non-Hodgkin’s lymphomas in the ocular adnexal lymphomas are rare, and they are reported to account for only about 2% of all cases of non-Hodgkin’s lymphoma and about 5%–15% of all cases of non-Hodgkin’s lymphoma at extranodal sites.Citation20–Citation22 In addition, follicular lymphomas are known to occur in 23%–31%Citation23–Citation25 of ocular adnexal lymphomas. So the prevalence of follicular lymphoma in the ocular adnexa in the Japanese is very low. To the best of our knowledge, only two cases of follicular lymphoma derived from the conjunctiva have been reported.Citation26,Citation27 In our case, the tumor was bilateral and were localized in the lacrimal glands, and is thus not related to follicular lymphomas of the conjunctiva. However, in the analysis of the follicular lymphomas of the conjunctiva, polymerase chain reaction using the tumor DNA has detected a fusion product of the major breakpoint region of the BCL2 gene and IgH J region.Citation27 Because of the rareness and small sample of the ocular tumor, it was difficult to diagnose such a case as follicular lymphoma by conventional methods.
Recently, the efficacy of rituximab therapy for follicular lymphomas has been evaluated. A few clinical trials using rituximab alone for untreated follicular lymphomasCitation28 and a few cases of conjunctival follicular lymphomas treated with rituximab alone have been reported.Citation27 Generally, the common side effects of rituximab are not severe, and no side effect of rituximab was observed in our case.
In summary, our case with tumors in both eyelids was diagnosed as follicular lymphoma with a combination of the findings of immunohistochemical and molecular genetic techniques. We conclude that the insights into the pathogenesis of lymphoid malignancies through new techniques such as genetic, molecular, and immunologic methods would help as complementary methods for the diagnosis, and lead to more accurate diagnosis and proper treatment.
Acknowledgment
The authors thank Dr Duco I Hamasaki for editing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- National Cancer Institute sponsored study of classification of non-Hodgkin’s lymphomas: Summary and description of a Working Formulation for clinical usageThe Non-Hodgkin’s Lymphoma Pathologic Classification ProjectCancer198249211221356896167
- HarrisNLJaffeESStainHA revised European-American classification of lymphoid neoplasms: A proposal from the International Lymphoma Study GroupBlood199484136113928068936
- Gerard-MarchantRHamlinILennertKClassification of non-Hodgkin’s lymphomaLancet19742406408
- StansfeldADieboldJNoelHUpdated Kiel classification for lymphomasLancet198812922932893097
- SwerdlowSHCampoEHarrisNLWHO Classification of Tumours of Haematopoietic and Lymphoid Tissues4th edLyonIARC Press2008
- LibraMGloghiniAMalaponteGAssociation of t(14;18) translocation with HCV infection in gastrointestinal MALT lymphomasJ Hepatol20084917017418538438
- LibraMde ReVGloghiniAFrequency of bcl-2/IgH translocation in patients with non-Hodgkin’s lymphoma and chronic hepatitis C virus infectionMinerva Gastroenterol Dietol20055116517015990705
- NakamuraSYeHBaconCMGastric MALT lymphoma with t(14;18)(q32;q21) involving IGH and BCL2 genes that responded to Helicobacter pylori eradicationJ Clin Pathol2007601171117317906071
- PalmedoGHantschkeMRüttenAPrimary cutaneous marginal zone B-cell lymphoma may exhibit both the t(14;18)(q32;q21) IGH/BCL2 and the t(14;18)(q32;q21) IGH/MALT1 translocation: An indicator for clonal transformation towards higher-grade B-cell lymphoma?Am J Dermatopathol20072923123617519619
- GlassmanABHayesKJThe value of fluorescence in situ hybridization in the diagnosis and prognosis of chronic lymphocytic leukemiaCancer Genet Cytogenet2005158889115771912
- DierlammJBaensMWlodarskaIThe apoptosis inhibitor gene API2 and a novel 18q gene, MLT, are recurrently rearranged in the t(11;18)(q21;q21) associated with mucosa-associated lymphoid tissue lymphomasBlood1999933601360910339464
- AndersonJRArmitageJOWeisenburgerDDEpidemiology of the non-Hodgkin’s lymphomas: Distributions of the major subtypes differ by geographic locations. Non-Hodgkin’s Lymphoma Classification ProjectAnn Oncol199897177209739436
- Lymphoma Study Group of Japanese PathologistsThe World Health Organization classification of malignant lymphomas in Japan: Incidence of recently recognized entitiesPathol Int20005069670211012982
- AokiRKarubeKSugitaYDistribution of malignant lymphoma in Japan: Analysis of 2260 cases, 2001–2006Pathol Int20085817418218251781
- KoYHKimCWParkCSREAL classification of malignant lymphomas in the Republic of Korea: Incidence of recently recognized entities and changes in clinicopathologic features. Hematolymphoreticular Study Group of the Korean Society of Pathologists. Revised European-American lymphomaCancer1998838068129708949
- HoFCToddDLokeSLClinico-pathological features of malignant lymphomas in 294 Hong Kong Chinese patients, retrospective study covering an eight-year periodInt J Cancer1984341431486381328
- ChenCYYaoMTangJLChromosomal abnormalities of 200 Chinese patients with non-Hodgkin’s lymphoma in Taiwan: With special reference to T-cell lymphomaAnn Oncol2004151091109615205204
- IntragumtornchaiTWannakrairojPChaimongkolBNon-Hodgkin’s lymphomas in Thailand. A retrospective pathologic and clinical analysis of 1391 casesCancer199678181318198859197
- SukpanichnantSSonakulDPiankijagumAMalignant lymphoma in Thailand: Changes in the frequency of malignant lymphoma determined from a histopathologic and immunophenotypic analysis of 425 cases at Siriraj HospitalCancer199883119712049740086
- DecaudinDde CremouxPVincent-SalomonAOcular adnexal lymphoma: A review of clinicopathologic features and treatment optionsBlood20061081451146016638927
- FisherSGFisherRIThe epidemiology of non-Hodgkin’s lymphomaOncogene2004236524653415322522
- KnowlesDMJakobiecFAMcNallyLBurkeJSLymphoid hyperplasia and malignant lymphoma occurring in the ocular adnexa (orbit, conjunctiva, and eyelids): A prospective multiparametric analysis of 108 cases during 1977 to 1987Hum Pathol1990219599732394438
- FungCYTarbellNJLucarelliMJOcular adnexal lymphoma: Clinical behavior of distinct World Health Organization classification subtypesInt J Radiat Oncol Biol Phys2003571382139114630277
- JakobiecFAOcular adnexal lymphoid tumors: Progress in need of clarificationAm J Ophthalmol200814594195018405875
- FerryJAFungCYZukerbergLLymphoma of the ocular adnexa: A study of 353 casesAm J Surg Pathol20073117018417255761
- AzumiAHiraiKTamuraYA case of follicular lymphoma derived from the conjunctivaNippon Ganka Gakkai Zasshi200210642042512187826
- TakahiraMOkumuraHMinatoHPrimary conjunctival follicular lymphoma treated with the anti-CD20 antibody rituximab and low-dose involved-field radiotherapyJpn J Ophthalmol20075114915117401629
- CohenYSolal-CelignyPPolliackARituximab therapy for follicular lymphoma: A comprehensive review of its efficacy as primary treatment, treatment for relapsed disease, re-treatment and maintenanceHaematologica20038881182312857561