
Abstract
Cataract surgery is one of the most commonly performed surgeries worldwide, with nearly 20 million cases annually. Appropriate prophylaxis after cataract surgery can contribute to a safe and quick visual recovery with high patient satisfaction. Despite being the current standard of care, the use of multiple postoperative eye drops can create a significant burden on these patients, contributing to documented and significant non-adherence to the postoperative regimen. Over the past 25 years, there have been a few studies analyzing the use of intracameral dexamethasone (DXM) in controlling inflammation following cataract surgery. This review explores various drug delivery approaches for managing intraocular inflammation after cataract surgery, documenting the strengths and weaknesses of these options and examining the role of intracameral DXM (among these other strategies) in controlling postoperative intraocular inflammation. Intracameral DXM has a particular advantage over topical steroids in possibly decreasing postoperative inflammatory symptoms and objective anterior cell and flare scores. Compared to topical steroids, there may be a slightly less theoretical risk of significant intraocular pressure spikes and systemic absorption. In addition, surveys indicate patients prefer an intraoperative intracameral injection over a self-administered postoperative eye drop regimen. However, there are several adverse effects associated with intracameral DXM delivery that are not seen with the noninvasive topical approach. Although it is unlikely that intracameral DXM will replace topical medications as the standard management for postoperative inflammation, it is seemingly another safe and effective strategy for controlling postoperative inflammation after routine cataract surgery.
Introduction
Vision impairment due to cataract inflicts 20 million individuals worldwide and represents nearly half the individuals with blindness.Citation1,Citation2 Since visual impairment from cataracts cannot be corrected by spectacle wear, contact lenses or medical treatment, cataract extraction is the only option for patients to clear optical media. Cataract surgery is one of the most commonly performed and most successful surgical procedures worldwide.Citation3 As with any intraocular surgery, varying degrees of inflammation occur secondary to mechanical damage from the surgical tissue manipulation and a mild reaction to the foreign intraocular lens (IOL), which may result in significant postoperative inflammation.Citation4,Citation5 The consequences of postoperative inflammation are cystoid macular edema, increased intraocular pressure, posterior capsular opacification, and protein leakage from the breakdown of the blood–aqueous barrier.Citation6 Even in uncomplicated cataract surgeries, the inflammatory sequelae may occasionally lead to chronic uveitis and fibrin formation contributing to an undesirable surgical outcome.Citation7
In a recent study, 34% of patients reported eye pain during the first 24 hours following cataract surgery and 10% of patients reported discomfort for as long as 6 weeks after surgery.Citation8 Postoperative visual symptoms attributed to inflammation include dryness, irritation, and pain, which may delay the postoperative recovery and affect patient satisfaction.Citation9–Citation11 Hence, addressing the inflammation is an important part of the postoperative care.
As early as 1950, the beneficial effect of corticosteroid therapy on inflammatory ocular disease was recognized. It has been well demonstrated that topical corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs) are effective drugs compared to placebo for decreasing anterior chamber inflammation and its sequelae.Citation5 In 2012, a survey of surgeons to the 132 members of the Association of Veterans Affairs Ophthalmologists reported that 97% of respondents were prescribed corticosteroid drops and or NSAID drops after cataract surgery,Citation12 supporting this regimen as a Standard of Care (SOC) in postoperative pharmaceutical treatment after cataract surgery.
Despite the current standard regimen of treatment, the use of postoperative eye drops creates a significant burden on these patients, especially since most postoperative cataract surgery patients are elderly with a limited ability to adhere to this treatment schedule. A study monitoring patient compliance with topical treatment after glaucoma surgery showed that nearly 30% of patients did not adhere to the treatment regimen.Citation13 Some studies imply the level of drug wastage and premature discontinuation of therapy may be higher in cataract surgery patients than any other ophthalmic surgeries.Citation14 Thus, there is a crucial need to develop simpler ways to provide postoperative drug delivery in a safe and effective manner.
The toxicity of intraocular dexamethasone (DXM) was studied in 1974 in the treatment of inflammatory diseases of the eye by Graham and Peyman.Citation15 However, in the past two decades, there have been a small number of studies analyzing the use of intracameral DXM in controlling post-cataract surgery inflammation.Citation16–Citation22 This strategy offers cataract surgeons the option of a single injection of DXM into the eye at the end of surgery. In order to improve the delivery method, two biodegradable DXM delivery systems for managing inflammation following cataract surgery have been developed, one of which received recent approval by the US Food and Drug Administration (FDA). These devices are intended to improve bioavailability, reduce non-adherence, and eliminate dosing miscalculations that can occur in the geriatric population. This review will compare the rationale of various routes of DXM administration in controlling post-cataract surgery inflammation and highlight the strengths and weaknesses of each method with a special emphasis on topical and intracameral DXM usage in various clinical studies. Importantly, it will highlight studies about the effectiveness and safety of intracameral DXM as well as assessing its role in the therapeutic management of inflammation after cataract surgery.Citation16–Citation22
Mechanism of action
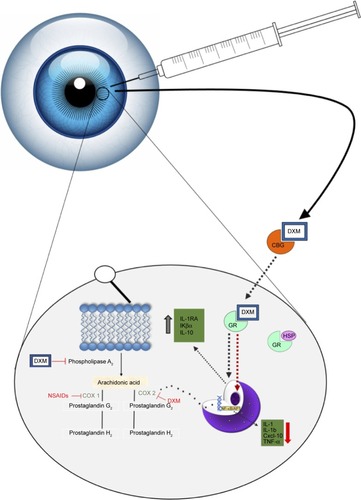
Dexamethasone is one of the most potent glucocorticoid preparations that downregulates a variety of inflammatory mediators. Similar to all glucocorticoids, DXM binds to the intracellular glucocorticoid receptor α after dissociation of the receptor from heat shock protein 90.Citation23,Citation24 This promotes translocation of the complex to the nucleus where it acts as a transcription factor to induce the expression of genes with anti-inflammatory effects, such as lipocortin, IL-1 receptor antagonist, IL-10, and IκBα genes.Citation25,Citation26 In addition, DXM inhibits upstream signaling through NF-κB and AP1 pathways, which prevents production of inflammatory cytokines (ie, TNF-α, IFN-γ, IL-6, etc.), chemokines (ie, CXCL-10, CCL5, etc.), and metalloproteinases (ie, MMP-1, MMP-2, MMP-3, MMP-9, etc.).Citation25 In various types of experimental and clinical ocular inflammatory situations, there is an increase in prostaglandins in the aqueous humor and tear film.Citation27,Citation28 Importantly, we know from prior studies that prostaglan-dins play an important role in mediating pain, hyperemia, photophobia, lacrimation, and decreased vision from cystoid macular edema, symptoms that are commonly exhibited in post-cataract eyes.Citation29,Citation30 DXM, similar to all corticosteroids, inhibits the production of prostaglandins by blocking the enzymatic activity of phospholipase A2-mediated release of arachidonic acid from cell membranes.Citation31 Experimental studies of inflammation have established that prostaglandin production is significantly higher in inflamed eyes compared to the non-inflamed baseline state.Citation31 For instance, in a study of endotoxin-induced uveitis in rabbits, a 60-fold-induction in the amount of prostaglandin was detected in the aqueous humor.Citation27 In contrast to cyclooxygenase-1 (COX-1) enzyme which is responsible for prostaglandin synthesis under baseline physiologic conditions and appears to maintain homeostasis, cyclooxygenase-2 (COX-2) is increasingly expressed after stimulation with proinflammatory cytokines, such as interleukin 1 (IL-1), tumor necrosis factor-alpha (TNF-alpha) and endotoxin in many cell types, including endothelial cells and monocytes/macrophages.Citation32 Therefore, one of the most important anti-inflammatory roles of DXM is suppression of COX-2 mediated production of inflammatory prostaglandins. In animal models of endotoxin-induced inflammation, simultaneous administration of DXM resulted in a five-fold decrease in prostaglandin synthesis.Citation27 Consequently, through various mechanisms of action (), DXM reduces some of the inflammatory-induced eye symptoms that are commonly reported by patients following cataract surgery.
Figure 1 A model of the mechanism of action upon administration of intraocular DXM.
Abbreviations: DXM, dexamethasone; CBG, cortisol-binding globulin; GR, glucocorticoid receptor; HSP, heat-shock protein; IL-1RA, interleukin-1 receptor antagonist; IL-10, interleukin 10; IL-1, interleukin-1; IL-1b, interleukin-1b; Cxcl-10, chemokine (C-X-C motif) ligand; TNF-α, tumor necrosis factor α; COX-1, cyclooxygenase 1; COX-2, cycloxygenase 2.
Routes of administration
An effective DXM treatment regimen needs to maintain a therapeutic concentration at its target site. In aqueous humor, the half-life of DXM is ~3–6 hours in solution.Citation33 The short half-life of DXM is a challenge in dosing, since therapeutic concentrations cannot be maintained for long periods. A discussion of the possible routes of DXM administration after cataract surgery follows, highlighting the advantages and disadvantages of each pharmaceutical preparation ().
Table 1 A summary of the advantages and disadvantages of various routes of DXM delivery to control post-cataract surgery inflammation
Topical drug delivery
Topical ophthalmic drug delivery represents the most popular option among cataract surgeons due to its effectiveness and good safety profile in controlling inflammation after cataract surgery. The major advantages of topical drug delivery include noninvasiveness, ease of administration, and there are a variety of new strategies to increase absorption (eg, prodrugs and nanotechnology). Importantly, it is also easier for the surgeon.
When compared to systemic administration, topical delivery confers certain advantages, such as lower systemic absorption and the avoidance of first pass metabolism.Citation34 However, upon instillation of eye drops, pre-corneal factors and anatomical barriers negatively influence the bioavailability of topical DXM. Examples of pre-corneal factors include tear lake turnover rate, tear film, blinking, induced lacrimation, and pharmaceutical drainage through the nasolacrimal apparatus.Citation35,Citation36 Human tear lake volume is estimated to be seven microliters (7 μL) and the tear sac may contain approximately 30 μL of an administered eye drop. Given the rapid restoration of tear lake every 2–3 minutes, most of the topical eye drops are washed away within 15–30 seconds after instillation.Citation36,Citation37 Additionally, rapid reflex blinking after instillation results in spillage or drainage of a large volume into the nasolacrimal duct and only about 10%–20% of the administered drug is available for corneal absorption, diminishing the total bioavailability in the anterior chamber to ~5%.Citation34,Citation38
Anatomical barriers to eye drop administration include the biphasic cornea, conjunctiva, and sclera with the corneal epithelium and stroma representing the most significant barriers to drug absorption.Citation39 DXM is a highly hydrophobic molecule that easily crosses the lipophilic epithelium. However, the drug is prevented from penetrating deeper into ocular tissue due to the presence of a hydrophilic stroma.Citation34 Multiple rabbit studies analyzed the corneal surface and found transmembrane efflux pumps (eg, P-glycoprotein, multidrug resistance protein, and breast cancer resistance protein) expressed on the corneal surface restrict drug penetration into the aqueous humor.Citation40–Citation42 In contrast, the corneal endothelium contains leaky tight junctions that facilitate passage of DXM between the aqueous humor and stroma, and thus, increases its bioavailability at the target site.Citation24 The conjunctiva is another major barrier to drug penetration. This highly vascularized tissue has an abundance of capillaries and the absorption of drug into the conjunctival blood vessels allows significant drug loss into the systemic circulation. In addition, lipophilic absorption of DXM into the conjunctival lymphatics reduces total drug bioavailability. However, given the globular and hydrophobic nature of DXM, it is capable of limited penetration through the sclera and conjunctival epithelial tight junctions; more so than other macromolecules that may be linear and hydrophilic.Citation43
Improvements in topical drug delivery method
A variety of novel strategies, such as prodrugs, nanosuspen-sions, nanomicelles, and cubosomes, have been developed for topical DXM therapy in order to improve overall bio-availability. A prodrug is a bioreversible derivative of drug molecules and is designed to be therapeutically inactive until enzymatic conversion.Citation34 Specifically, these formulations can evade the aforementioned efflux pumps present on the corneal surface.Citation36 Civiale et alCitation44 investigated a variety of prodrug formulations with DXM and measured the permeability through the corneal surface of rabbit cornea and bovine conjunctival epithelial cells. They reported that permeability of DXM correlated strongly with lipophilicity of the prodrugs. For instance, prodrug formulations, such as acetate, propionate, and butyrate esters, demonstrated higher permeability due to higher lipophilicity with maximum penetration occurring with butyrate esters. Other prodrugs, such as sodium phosphate, have low permeability due to their ionic and hydrophilic structure. Thus, formulations of DXM with butyrate esters or other lipophilic prodrugs may help increase bioavailability of DXM in the anterior chamber. Another strategy to increase bioavailability of topical formulations is via nanoparticle delivery (eg, nanosuspensions, nanomi-celles). Nanosuspensions increase saturation solubility of poorly soluble drugs, increase surface area available for dissolution, and allow for greater bioadhesion and corneal penetration.Citation45 Kassem et alCitation45 demonstrated that DXM nano-suspensions, along with hydrocortisone and prednisolone prepared nanosuspensions, enhanced the rate and extent of drug absorption, with improved drug action when compared to micro-crystalline suspensions and solutions.
Pepić et alCitation46 demonstrated increased anterior ocular tissue bioavailability by 2.4-fold by DXM compounded with nano-micelle formulations using chitosan/pluronic systems relative to unformulated DXM. Nanovehicles of pluronics block copolymers may be used for drug delivery and are combined with chitosan, a cationic polymer. They have proved to be a potent formulation in increasing target area bioavailability. Pluronics significantly improve the solubility and enhance the viscosity of topical drug formulations whereas chitosan improves corneal penetration via the unique ability to open tight junctions.Citation34 Similarly, the in vitro permeability coefficient of DXM formulated in cubosomes, the very stable nanoparticles of the biscontinuous cubic lipid crystalline phase, exhibited a 3.5- to 4.5-fold increase compared to DXM sodium phosphate eye drops. Delivery of DXM cubosomes also exhibited a 1.8-fold and 8.0-fold increase in the area under the curve after 240 minutes when measuring DXM in the aqueous humor relative to DXM eye drops and suspensions, respectively. These novel techniques for topical drug delivery represent strategies to bypass significant barriers in drug penetration. Overall, they increase bioavailability, prolong action, and may possibly minimize adverse effects in the anterior chamber.Citation34,Citation45,Citation46
Periocular drug delivery
The periocular routes include subconjunctival, sub-Tenon’s, retrobulbar, and peribulbar administration and are all less invasive than the intravitreal route. A subconjunctival injection bypasses the cornea–conjunctiva barrier allowing for greater bioavailability into the anterior chamber than topical delivery affords. However, other studies,Citation47 evaluating dynamic barriers, which include conjunctival vessels and lymphatic circulation, document rapid clearance of subconjunctival DXM into the systemic circulation. Hos-seini and colleaguesCitation47 observed the maximum DXM plasma concentration after subconjunctival injection of DXM and an intravitreal injection of a similar DXM concentration was 83.3 nM and 9.3 nM, respectively. Thus, compared to an intravitreal injection, a subconjunctival injection has greater absorption into the systemic circulation, increasing the risk for possible systemic side effects.
Intravitreal drug delivery
Patients with pre-existing non proliferative and proliferative diabetic retinopathy are at a great risk of developing postoperative diabetic macular edema (DME) after cataract surgery even if they do not already have it, or worsening of pre-existing DME.Citation48 Intravitreal DXM injection given postoperatively or in the infusion fluid (64 mg DXM in 500 cc/balanced salt solution) during surgery offers the advantage of decreasing diabetic macular edema after cataract surgery.Citation49,Citation51 Following an intravitreal injection, the drug can be eliminated either via the anterior route from aqueous turnover and uveal outflow or via the posterior route through drug penetration across the blood–retinal barrier.Citation34,Citation36 Drugs that are lipophilic with small molecular weight tend to have a decreased half-life.Citation36 The half-life of DXM is about 3 hours in the vitreous.Citation50 Graham and Peyman demonstrated the safety of administering massive doses of intraocular DXM without producing toxic side effects.Citation15 Particularly, it has been demonstrated that up to 4.8 mg of DXM can be injected in normal phakic eyes without producing a toxic reaction.Citation51 Although very rare, there is the possibility of significant adverse effects, such as endophthalmitis, retinal detachment, and vitreous hemorrhage from the injection.Citation24 Using DXM in the infusion fluid or pre-operative intravitreal DXM for routine and uncomplicated cataract surgery has not been reported in literature, but it is recommended for eyes with diabetic retinopathy (to mitigate exacerbation of DME) and uveitis (to decrease postoperative inflammation and CME).Citation51
Intracameral drug delivery
Although use of intracameral DXM has limited literature regarding its pharmacokinetics, its use intrinsically confers certain advantages. For instance, intracameral DXM is administered at the target site allowing higher drug levels in the anterior chamber. This effectively means less drug is needed to achieve the desired effect and can potentially reduce local side effects, such as increased intraocular pressure.Citation52 In addition, it theoretically reduces corneal and systemic side effects that can occur with topical steroid therapy. Studies have shown that when DXM is injected intracamerally, there is a statistically significant increase in efficacy when compared to other routes of administration, such as subconjunctival or sub-Tenon’s.Citation21,Citation53 In fact, compared to these other modalities of administration, intracameral delivery reduces the risk of skin hypopigmentation, extraocu-lar muscle atrophy, and subdermal fat atrophy.Citation21,Citation52 Nonetheless, there are several disadvantages specific to intracameral drug delivery. A possible concern of such drug delivery is toxic anterior segment syndrome (TASS), a sterile postoperative inflammatory reaction caused by a noninfectious substance that enters the anterior segment.Citation54 This results in toxic damage to intraocular tissues. Since any medication injected around the eye, and especially, in proximity to the anterior chamber can be implicated with this condition, this adverse effect should certainly be at the forefront of any surgeon’s mind. More commonly, this is seen with the use of intracameral anesthetics or antibiotics. To date, there have been no reports of TASS from intracameral injection of DXM (or any other corticosteroid). However, the use of biodegradable sustained-release implants in the anterior chamber (see below) may be a risk factor for TASS. Another adverse effect to consider is the damage to and/or loss of endothelial cells from intracameral injection (discussed in further detail under “Clinical Studies”).
Systemic absorption of DXM after intracameral injection
Aqueous humor outflow ultimately enters the systemic circulation from the episcleral vasculature and is the main source of systemic absorption of drugs injected intracamerally.Citation55 Systemic exposure to DXM was evaluated in two studies.Citation56 One study reported DXM plasma concentrations at several time intervals within the first 30 days, postoperatively. The intracameral injection of 342 mcg or 517 mcg of DXM at the end of cataract surgery resulted in a plasma concentration on postoperative day 1 that ranged from 0.09 to 0.86 ng/mL and 0.07 to 1.16 ng/mL, respectively. The second study, reported the day 1 plasma concentration for patients who received 517 mcg of intracameral DXM ranged from 0.349 to 2.79 ng/mL. In both reports, these plasma concentrations were significantly below any known toxic plasma concentration of steroids.Citation57 Additionally, very few patients had measurable levels of DXM in plasma at early postoperative intervals, in contrast to periocular and intravitreal injections.Citation47 Hence, despite its potency, the use of intracameral DXM is unlikely to cause significant systemic side effects.
Improvements in intracameral drug delivery method
To control inflammation after cataract surgery, two biodegradable anterior segment drug devices have been developed – one of which has been recently approved by the FDA. These implantable sustained release devices are advantageous for anterior segment inflammation because they deliver effective drugs to the target area and reduce the need for frequent intraocular injections. Continuous release is achieved by imbedding a bulk-eroding biodegradable polymer with the DXM. When the polymer is subsequently degraded slowly, the DXM is released.Citation58 Since polylactic acid (PLA) takes from 1 to 5 years to degrade, it is combined with polyglycolic acid (PGA) to form poly-lactide-co-glycolide (PLGA), which accelerates degradation time. By varying the ratio of PLA to PGA, one can select degradation time. However, since PLGA is a bulk-erosion polymer, it potentially draws significant water into its core, resulting in possible destruction of the medication. Another drawback is auto-catalysis, in which the core polymer is degraded too quickly, resulting in rapid drug release and adverse effects, including a sudden spike in intraocular pressure.Citation58
Surodex® (Oculex Pharmaceuticals, Inc., Sunnyvale, CA, USA) is a rod-shaped biodegradable implant (1.0 × 0.5 mm) that is placed in either the inferior anterior chamber angle or in the ciliary sulcus of the posterior chamber.Citation59,Citation60 The implant is injected using a 25-gauge needle intracamerally and provides a sustained drug release of 60 μg of DXM with near zero-order kinetics over 7–10 days.Citation60 Surodex significantly reduces the total dose delivered. The total dose in one pellet of Surodex (60 μg of DXM) is roughly equivalent to that in just one drop of 0.1% DXM.Citation61 The physician can then visually monitor the status and rate of delivery while also tailoring the treatment to the individual patient. Additionally, if there are any significant complications, the implant can be removed if needed. Suro-dex has completed phase three clinical trials in the US, and although the status of pursuit for FDA approval in the US is currently unknown, Surodex has been popular and approved for use in Singapore, China, and many other countries.Citation62
The Dexycu® (Icon Bioscience, Inc. Sunnyvale, CA, USA) treatment is applied as a single intracameral injection at the end of cataract surgery using Icon’s Verisome™ (Icon Bioscience, Inc.) drug delivery technology to dispense a biodegradable extended-release formulation. For up to 21 days, the controlled delivery of DXM is given, although depending on surgeon preference, it can be customized to dispense anywhere from 1 week to over 9 months duration with a single injection.Citation22 The procedure involves the surgeon injecting a 5-μL droplet of the IBI-10090 suspension of DXM via an intracameral injection into the anterior chamber using the standard 30-gauge needle.Citation59 In early 2018, Dexycu was the first long-acting intracameral product to be approved by the FDA in the US for treating inflammation following cataract surgery.Citation22
With the use of these devices, the advantages should be weighed against the disadvantages, which include possible angle or corneal endothelium damage from physical migration of the device, localized damage at the site of implantation, and difficult extraction, if removal is required.Citation16 Additionally, if intraocular pressures remain high, the physician may find it more difficult to control and monitor such devices over topical formulations, which may be easily discontinued.
These delivery methods have been implemented for other uses and are very effective. In the treatment of glaucoma, intracameral administration of anti-glaucoma drugs via a sustained-release biodegradable technology has been very efficacious.Citation63 In 2015, Navratil et alCitation64 demonstrated sustained intraocular pressure lowering over the course of 6 months using intracameral sustained-release travoprost. Compared to topical administration, a significantly lower aqueous humor concentration of travoprost was needed.Citation63 Thus, long-term intracameral drug delivery implants, whether for the use of glaucoma or postoperative cataract inflammation, may be beneficial because they require minimal patient compliance, resulting in increased adherence to therapy.
Clinical studies: intracameral DXM
Anterior chamber cells and flare
In 1999, Tan et alCitation16 compared the use of intracameral DXM (60 μg) via a Surodex delivery system to 0.1% DXM eye drops for treatment of postoperative inflammation after cataract surgery using the laser flare photometry instrument as a reproducible assessment of anterior chamber inflammation.Citation65,Citation66 Tan’s study showed mean postoperative flare values lower in the Surodex eyes at all postoperative visits within 30 days after surgery. During the first 14 days, flare values in eyes receiving DXM eye drops were generally twice those of eyes receiving Surodex. However, by 90 days, there was no significant difference between treatment groups. The slit-lamp inflammation assessment of cell and flare scores was also lower in the Surodex group compared to the DXM eye drop group at all postoperative visits. Despite the fact that there was no statistically signifi-cant difference in postoperative inflammation by laser flare between Surodex intracameral DXM and topical steroids, eyes that received Surodex demonstrated less laser flare than those which received topical steroids at all postoperative intervals.Citation18 In a later similar study, Tan et alCitation18 observed no significant differences in anterior chamber cell and flare assessed by slit lamp between Surodex-treated eyes and topical DXM 0.1%. In addition, there was no significant difference between laser flare meter readings between the groups throughout each postoperative interval. Gungor et alCitation20 evaluated the difference in postoperative inflammation management between intracameral DXM (0.4 mg/0.1 mL) and intracameral triamcinolone acetonide (2 mg/0.05 mL). The two treatment regimens both reduced anterior chamber cells and flare equally and effectively without any statistically significant difference at any postoperative interval. In the recent phase III FDA trialCitation22 using the Dexycu delivery system, 63% and 66% of patients showed no anterior chamber inflammation at postoperative day 8 when dosed at 343 μg or 517 μg of DXM, respectively. In contrast, only 25% of the no-treatment group exhibited anterior chamber clearing at postoperative day 8. A significant limitation to this study was the lack of comparison to current standard-of-care treatments, such as topical DXM.
Overall, there are a total of six studies that support that injection of intracameral DXM (either with or without the use of a drug delivery system) significantly reduces postoperative anterior chamber cell and flare.Citation17–Citation20,Citation22,Citation67
Subjective postoperative inflammatory symptoms
Studies have shown that generally fewer patients report postoperative inflammatory symptoms when treated with intracameral DXM. For instance, Surodex-treated groups have reported fewer symptoms of discomfort, pain, photophobia, and lacrimation compared to patients on no therapy.Citation17 Tan et alCitation18 reported a significant decrease in subjective ocular discomfort, photo-phobia, and lacrimation in eyes treated with Surodex compared to those treated with topical DXM. In contrast, Wadood et alCitation19 observed no difference in inflammatory symptoms of conjunc-tival hyperemia or ciliary injection in eyes receiving Surodex compared to eyes receiving DXM eye drops. In other studies, decreased subjective inflammatory symptoms are reported in the first week postoperatively in Surodex-treated eyes. Statistical differences are negligible after that first week when compared to eyes receiving DXM eye drops.Citation17,Citation18 Another study that used intracameral DXM without a drug delivery system showed no significant difference in postoperative subjective visual symptoms between eyes that received intracameral DXM and those that received topical prednisolone and ketoro-lac eye drops after cataract surgery.Citation67 Since some studies have shown topical NSAIDs are more effective than some potent topical steroids in controlling postoperative inflammation,Citation68–Citation70 the use of ketorolac in this study may be a confounding factor resulting in the lack of a significant difference in postoperative inflammatory symptoms.Citation68–Citation70
Visual acuity
Six studies reported a significant improvement in visual acuity in eyes where intracameral DXM was administered.Citation16,Citation18–Citation20,Citation22,Citation67 Four of the six studies reported qualitative improvement while the other two reported quantitative improvement using logMAR (). At postoperative days 30 and 60, the mean respective logMAR was 0.07 and 0.06 for two studies that quantitatively reported the visual acuity of eyes injected with intracameral DXM.Citation19,Citation20 In comparison, five studiesCitation19,Citation71–Citation74 that reported the logMAR visual acuity after post-operative topical steroid use (the type of steroid varied) ranged from −0.066 to 0.15 after approximately 6–8 weeks postoperatively (). The postoperative visual acuity did not differ significantly in eyes receiving intracameral DXM compared to those that received topical steroids. Notably, no eye lost best corrected visual acuity with either intracameral or topical DXM use.
Table 2 A summary of the visual acuity using intracameral DXM and topical steroids at a postoperative interval (~4–6 weeks). Only studies that quantitatively evaluated visual acuity using the logMAR scale were included
Safety and tolerability
Intraocular pressure
One of the problems with administration of intraocular steroids is intraocular pressure (IOP) control. There are several proposed mechanisms of corticosteroid-induced increase in IOP. It is postulated that the glucocorticoid receptor complex causes cross-linking of actin fibers in the trabecular meshwork (TM). There may also be inhibition of proteases and trabecular meshwork endothelial cell phagocytosis that results in impaired drainage from extra material in the TM.Citation75 This leads to a steroid-induced increase in intraocular pressure due to decreased outflow and increased outflow resistance.Citation75 Since direct administration into the anterior or posterior chamber requires a lower drug concentration, it may be inferred that intracameral drug delivery may not elevate IOP as much as topical delivery. Other studies have demonstrated that the mean IOP elevation is generally greater after sub-Tenon’s and/or intravitreal steroid administration. Roth et alCitation76 demonstrated that IOP spikes of greater than 20 mmHg occurred more frequently in glaucomatous eyes after intravitreal triamcinolone acetonide.
Similarly, a sub-Tenon’s injection of triamcinolone more frequently resulted in ocular hypertension refractory to maximum medical therapy.Citation67,Citation77 Topical administration of DXM has also been shown to increase mean IOP. An investigation by Pleyer et alCitation75 demonstrated that 0.1% of DXM drops administered four-times daily for 6 weeks provoked a mean increase in IOP by 8.6 mmHg. The observed increase in IOP with other topical corticosteroids, including newer generation pharmaceuticals (eg, rimexolone, difuprednate, and lotepre-dnol etabonate), had comparable mean changes.Citation75 This value is significantly more than the observed IOP increases using intracameral DXM (injection or sustained-released).Citation18,Citation22
However, there are an insufficient number of randomized-controlled trials evaluating whether there is any difference in postoperative mean IOP between intracameral DXM and topical steroids. The few that have evaluated this outcome show no significant difference (). Other studies using intracameral triamcinolone have reported minimal effect on mean IOP in eyes with no history of glaucoma.Citation78 Chang et alCitation67 observed no significant rise in postoperative IOP after intracameral DXM-treated glaucomatous eyes, but compared intracameral triamcinolone to intracameral DXM and observed a smaller increase in intraocular pressure in the initial postoperative period using triamcinolone.Citation20 This is presumably secondary to the short half-life of intraocular DXM (~3 hours) and rapid aqueous volume turnover, minimizing the risk of steroid-induced intraocular hypertension.Citation79
Table 3 A summary of evidence of all studies that have used intracameral DXM after cataract surgery
Corneal endothelial cells
One of the major complications that stems from an intra-cameral injection is the loss of corneal endothelial cells as the pharmaceutical contacts these fragile cells. Since this layer may not regenerate, a significant reduction of the endothelial cell count causes impairment of the endothelium pumping, resulting in stromal edema.Citation80 Jamil et alCitation21 studied the effects of intracameral DXM on corneal endothelial cell loss. They determined there was no difference between endothelial cell numbers after intracameral injection compared to a subconjunctival DXM injection. Three months postopera-tively, intracameral DXM-treated eyes demonstrated a mean endothelial cell count of 2,471 whereas subconjunctival DXM had a mean endothelial cell count of 2,496 implying intracameral DXM was not harmful for corneal endothelium. Six other studiesCitation17–Citation20,Citation22,Citation67 that reported endothelial cell count after intracameral DXM demonstrated no significant cell loss. In these studies, corneal edema was not significantly higher in eyes that received intracameral DXM compared to those that received placebo.Citation22
Adverse events
When adverse effects occurred in eyes that received intracam-eral DXM, the complications were generally associated with implantation of the biodegradable device. A few eyes that were implanted with Surodex demonstrated mild localized angle changes in proximity to the pellet remnant. In most cases, there were a few degrees of focal peripheral anterior synechiae, but no pupil distortion was noted.Citation18 A few patients who were given Surodex treatment had a mild hyphema clot that resolved after day 1.Citation18 When Surodex was placed in the ciliary sulcus, migration to the anterior chamber often occurred but this event did not affect visual outcomes.Citation18 There was one case that required reposition of iris after traumatic iris prolapse. Eyes that received DXM via the Verisome system had an increased incidence of postoperative dry eyes compared with those without any treatment. However, an adequate analysis could not be made since the patients’ preoperative levels of dry eyes were not measured. In eyes that received a single intracameral DXM injection, no significant complications were reported. The frequency of other adverse events such as posterior capsule opacification, cystoid macular edema, vitreous floaters, iritis, and retinal detachment was similar in eyes that received intracameral DXM compared to those that received any other form of postoperative treatment.Citation19,Citation20,Citation22
A summary of the visual symptoms, anterior cell and flare scores, intraocular pressure changes, corneal endothe-lial cell changes, and any adverse effects from the clinical studies using intracameral DXM after cataract surgery is shown in .
Intracameral DXM: place in therapy
It has been well documented that intracameral DXM after cataract surgery is a safe and effective option in decreasing postoperative inflammation. Intracameral DXM has a particular advantage over topical steroids in decreasing postoperative visual symptoms and anterior cell and flare scores, although some studies show no difference. Compared to some topical steroids at 0.1% solution and more, there may be a slightly lower theoretical risk of significant intraocular pressure spikes and systemic absorption. In addition, certain risks that are classically associated with intracameral administration, such as TASS and corneal endothelial cell loss, are much less likely than initially perceived based on current evidence. Nonetheless, there are certain adverse effects associated with intracameral administration. These are seen when placing a biodegradable sustained-release system, and may include the possibility of iris prolapse, surgical hyphema, focal peripheral anterior synechiae, and implant migration. Importantly, these adverse events are easily resolvable and do not cause any measurable vision loss.
The use of intracameral DXM reduces the burden on patients to maintain their postoperative regime with multiple pharmaceutical drops. Most surgeons use a combination of both steroid and NSAID drops and antibiotic drops. Patients have a difficult time tracking these various bottles and remembering the number of corresponding drops. A small study demonstrated that patients preferred a postoperative injection over the self-administration of drops after cataract surgery, presumably due to elimination of the postoperative drop regimen.Citation81 There are also significant financial implications with purchasing multiple bottles of topical therapy. We know from prior studies that bottle-tip contamination and the elevated risk of ocular surface trauma is particularly problematic in the early postoperative period in cataract patients.Citation82 One study showed that almost 60% of patients touched their eyes with the bottle tip while instilling the drops, while almost 80% did not wash their hands before instillation.Citation82 In the postoperative setting, this can greatly increase the risk of infection or other adverse events.Citation83 Hence, reducing the treatment burden on the patient may help improve patient satisfaction and increase the safety profile. Despite this evidence, topical therapy has been the standard of care for many decades and has an excellent track record of efficacy and safety to support its use. It is noninvasive, compared to the risks associated with intracameral DXM, and there are certain pharmaceuticals that can help improve overall bioavailability at the target site.
In summary, DXM at low doses seldom causes increase in intraocular pressure, when given infrequently, in combination with other anti-inflammatory agents or antibiotics to blunt acute inflammatory processes of the eye.Citation15
Conclusion
The ideal postoperative drug delivery system is one that minimizes systemic side effects, remains confined to a specific target area, minimizes the amount of pharmaceutical needed to reach the therapeutic level, decreases problems of compliance, and maximizes visual recovery. Intracam-eral DXM provides all these benefits as it controls post-surgical inflammation following cataract surgery. Although it is unlikely that intracameral DXM injections will replace topical medications as the standard of care for post cataract inflammation, the evidence demonstrates that its use offers another safe and effective approach.
Disclosure
The authors report no conflicts of interest in this work.
References
- ResnikoffSPascoliniDEtya’aleDGlobal data on visual impairment in the year 2002Bull World Health Organ2004821184485115640920
- BaltussenRSyllaMMariottiSPCost-effectiveness analysis of cataract surgery: a global and regional analysisBull World Health Organ200482533834515298224
- CongdonNO’ColmainBKlaverCCCauses and prevalence of visual impairment among adults in the United StatesArch Ophthalmol2004122447748515078664
- HigashideTSugiyamaKUse of viscoelastic substance in ophthalmic surgery – focus on sodium hyaluronateClin Ophthalmol200821213019668386
- DuanPLiuYLiJThe comparative efficacy and safety of topical non-steroidal anti-inflammatory drugs for the treatment of anterior chamber inflammation after cataract surgery: a systematic review and network meta-analysisGraefes Arch Clin Exp Ophthalmol2017255463964928130595
- DickHBSchwennOKrummenauerFKristRPfeifferNInflammation after sclerocorneal versus clear corneal tunnel phacoemulsificationOphthalmology2000107224124710690818
- da Rocha LimaBPichiFNucciPSrivastavaSKLowderCYFibrin reaction after uveitic cataract surgery: treatment and preventionEur J Ophthalmol201424462662824519510
- Porela-TiihonenSKaarnirantaKKokkiMPurhonenSKokkiHA prospective study on postoperative pain after cataract surgeryClin Ophthalmol201371429143523885165
- Garcia-GutierrezSQuintanaJMAguireUImpact of clinical and patient-reported outcomes on patient satisfaction with cataract extractionHealth Expect201417676577522784407
- FeenyDSpritzerKHaysRDAgreement about identifying patients who change over time: cautionary results in cataract and heart failure patientsMed Decis Making201232227328622009666
- Porela-TiihonenSKokkiHKaarnirantaKKokkiMRecovery after cataract surgeryActa Ophthalmol201694Suppl 2134
- GreenbergPBHavnaerAOettingTAGarcia-FerrerFJCataract surgery practice patterns in the United States Veterans Health AdministrationJ Cataract Refract Surg201238470570922365578
- OkekeCOQuigleyHAJampelHDAdherence with topical glaucoma medication monitored electronically the Travatan Dosing Aid studyOphthalmology2009116219119919084273
- HermannMMUstündagCDiestelhorstMElectronic compliance monitoring of topical treatment after ophthalmic surgeryInt Ophthalmol201030438539020373127
- GrahamROPeymanGAIntravitreal injection of dexamethasone. Treatment of experimentally induced endophthalmitisArch Ophthalmol19749221491544211214
- TanDTCheeSPLimLLimASRandomized clinical trial of a new dexamethasone delivery system (Surodex) for treatment of post-cataract surgery inflammationOphthalmology199910622232319951469
- ChangDFGarciaIHHunkelerJDMinasTPhase II results of an intraocular steroid delivery system for cataract surgeryOphthalmology199910661172117710366088
- TanDTCheeSPLimLThengJvan EdeMRandomized clinical trial of Surodex steroid drug delivery system for cataract surgery: anterior versus posterior placement of two Surodex in the eyeOphthalmology2001108122172218111733254
- WadoodACArmbrechtAMAspinallPADhillonBSafety and efficacy of a dexamethasone anterior segment drug delivery system in patients after phacoemulsificationJ Cataract Refract Surg200430476176815093636
- GungorSGBulamBAkmanAColakMComparison of intracam-eral dexamethasone and intracameral triamcinolone acetonide injection at the end of phacoemulsification surgeryIndian J Ophthalmol201462886125230962
- JamilAZAhmedAMirzaKAEffect of intracameral use of dex-amethasone on corneal endothelial cellsJ Coll Physicians Surg Pak201424424524824709236
- DonnenfeldEHollandEDexamethasone intracameral drug-delivery suspension for inflammation associated with cataract surgery: a ran-domized, placebo-controlled, Phase III trialOphthalmology2018125679980629397189
- CourseyTGHenrikssonJTMarcanoDCDexamethasone nano-wafer as an effective therapy for dry eye diseaseJ Control Release201521316817426184051
- Rodríguez VillanuevaJRodríguez VillanuevaLGuzmán NavarroMPharmaceutical technology can turn a traditional drug, dexamethasone into a first-line ocular medicine. A global perspective and future trendsInt J Pharm20175161–234235127889587
- MogensenTHBergRSPaludanSRØstergaardLMechanisms of dexamethasone-mediated inhibition of Toll-like receptor signaling induced by Neisseria meningitidis and Streptococcus pneumoniaeInfect Immun200876118919717938219
- PrabhuPDubeyAParthVGhateVInvestigation of hydrogel membranes containing combination of gentamicin and dexamethasone for ocular deliveryInt J Pharm Investig201554214
- KulkarniPSMancinoMStudies on intraocular inflammation produced by intravitreal human interleukins in rabbitsExp Eye Res19935632752798386101
- KulkarniPSSrinivasanBDCyclooxygenase and lipoxygenase pathways in anterior uvea and conjunctivaProg Clin Biol Res198931239522508129
- McGheeCNDeanSDanesh-MeyerHLocally administered ocular corticosteroids: benefits and risksDrug Saf2002251335511820911
- AbadiaBCalvoPFerrerasABartolFVerdesGPabloLClinical applications of dexamethasone for aged eyesDrugs Aging201633963964627566619
- MasferrerJLKulkarniPSCyclooxygenase-2 inhibitors: a new approach to the therapy of ocular inflammationSurv Ophthalmol199741Suppl 2S35S409154274
- RazAWycheANeedlemanPTemporal and pharmacological division of fibroblast cyclooxygenase expression into transcriptional and translational phasesProc Natl Acad Sci U S A1989865165716612493647
- BhagatRZhangJFarooqSLiXYComparison of the release profile and pharmacokinetics of intact and fragmented dexamethasone intravitreal implants in rabbit eyesJ Ocul Pharmacol Ther2014301085485825411827
- CholkarKPatelSPVadlapudiADMitraAKNovel strategies for anterior segment ocular drug deliveryJ Ocul Pharmacol Ther201329210612323215539
- TasmanWJaegerEADuane’s OphthalmologyPhiladelphia, PALippincott Williams & Wilkins2009
- GaudanaRAnanthulaHKParenkyAMitraAKOcular drug deliveryAAPS J201012334836020437123
- AhmedIPattonTFImportance of the noncorneal absorption route in topical ophthalmic drug deliveryInvest Ophthalmol Vis Sci19852645845873884542
- UrttiAPipkinJRorkGSendoTFinneUReptaAControlled drug delivery devices for experimental ocular studies with timolol 2. Ocular and systemic absorption in rabbitsInt J Pharm1990613241249
- MannermaaEVellonenKSUrttiADrug transport in corneal epithelium and blood-retina barrier: emerging role of transporters in ocular pharmacokineticsAdv Drug Deliv Rev200658111136116317081648
- KarlaPKEarlaRBodduSHJohnstonTPPalDMitraAMolecular expression and functional evidence of a drug efflux pump (BCRP) in human corneal epithelial cellsCurr Eye Res20093411919172464
- KarlaPKPalDMitraAKMolecular evidence and functional expression of multidrug resistance associated protein (MRP) in rabbit corneal epithelial cellsExp Eye Res2007841536017083930
- DeySPatelJAnandBSMolecular evidence and functional expression of P-glycoprotein (MDR1) in human and rabbit cornea and corneal epithelial cell linesInvest Ophthalmol Vis Sci20034472909291812824231
- KimSHLutzRJWangNSRobinsonMRTransport barriers in transscleral drug delivery for retinal diseasesOphthalmic Res200739524425417851264
- CivialeCBucariaFPiazzaSPeriOMianoFEneaVOcular permeability screening of dexamethasone esters through combined cellular and tissue systemsJ Ocul Pharmacol Ther2004201758415006161
- KassemMAAbdel RahmanAAGhorabMMAhmedMBKhalilRMNanosuspension as an ophthalmic delivery system for certain gluco-corticoid drugsInt J Pharm20073401–212613317600645
- PepićIHafnerALovrićJPirkićBFilipović-GrcićJA nonionic surfactant/chitosan micelle system in an innovative eye drop formulationJ Pharm Sci201099104317432520310026
- HosseiniKMatsushimaDJohnsonJPharmacokinetic study of dexamethasone disodium phosphate using intravitreal, subconjunctival, and intravenous delivery routes in rabbitsJ Ocul Pharmacol Ther200824330130818476800
- KimSJEquiRBresslerNMAnalysis of macular edema after cataract surgery in patients with diabetes using optical coherence tomographyOphthalmology2007114588188917275910
- CalvoPFerrerasAAl AdelFDangboonWBrentMHEffect of an intravitreal dexamethasone implant on diabetic macular edema after cataract surgeryRetina201838349049628196056
- ParisCLPeymanGAGremillionCMBlinderKJIntravitreal dex-amethasone following vitreous surgeryInt Ophthalmol19911531731742050472
- NabihMPeymanGATawakolMENaguibKToxicity of high-dose intravitreal dexamethasoneInt Ophthalmol19911542332351917317
- KanskiJJClinical ophthalmologyA Systematic Approach2nd edBurlington, MAButterworth-Heinemann2007629
- VengatesanMRMittalVNanoparticle- and Nanofiber-Based Polymer Nanocomposites: An OverviewWiley Spherical and Fibrous Filler CompositesWeinheim, GermanyWiley-VCH20161138
- MamalisNEdelhauserHFDawsonDGChewJLeboyerRMWernerLToxic anterior segment syndromeJ Cataract Refract Surg200632232433316565012
- GoelMPiccianiRGLeeRKBhattacharyaSKAqueous humor dynamics: a reviewOpen Ophthalmol J20104525921293732
- United States Food and Drug AdministrationDexycu Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/208912s000lbl.pdfAccessed June 3, 2018
- ShaikhSVermaHYadavNJauhariMBullangowdaJApplications of steroid in clinical practice: a reviewISRN Anesthesiol201220127111
- LeeDJIntraocular implants for the treatment of autoimmune uveitisJ Funct Biomater20156365066626264035
- HaghjouNSoheilianMAbdekhodaieMJSustained release intraocular drug delivery devices for treatment of uveitisJ Ophthalmic Vis Res20116431731922454753
- LeeSSHughesPRossADRobinsonMRBiodegradable implants for sustained drug release in the eyePharm Res201027102043205320535532
- LeeSYCheeSPBalakrishnanVFarzavandiSTanDTSuro-dex in paediatric cataract surgeryBr J Ophthalmol200387111424142614609850
- WangJJiangAJoshiMChristoforidisJDrug delivery implants in the treatment of vitreous inflammationMediators Inflamm2013201318
- DurairajCOcular pharmacokineticsHandb Exp Pharmacol2017242315527787714
- NavratilTGarciaATullyJPreclinical Evaluation of ENV515 (travoprost) Intracameral Implant-Clinical Candidate for Treatment of Glaucoma Targeting Six-Month Duration of ActionInvestigative Ophthalmology & Visual Science2014551335483548
- El-MaghrabyAMarzoukiAMatheenTMSouchekJvan der KarrMReproducibility and validity of laser flare/cell meter measurements of intraocular inflammationJ Cataract Refract Surg199319152558426323
- SawaMTsurimakiYTsuruTShimizuHNew quantitative method to determine protein concentration and cell number in aqueous in vivoJpn J Ophthalmol19883221321423054216
- ChangDTHercegMCBilonickRACamejoLSchumanJSNoeckerRJIntracameral dexamethasone reduces inflammation on the first postoperative day after cataract surgery in eyes with and without glaucomaClin Ophthalmol20093134535519668589
- KesselLTendalBJørgensenKJPost-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: a systematic reviewOphthalmology2014121101915192424935281
- HirneißCNeubauerASKampikASchönfeldCLComparison of prednisolone 1%, rimexolone 1% and ketorolac tromethamine 0.5% after cataract extraction. A prospective, randomized, double-masked studyGraefe’s Arch Clin Exp Ophthalmol2005243876877315756571
- El-HaraziSMRuizRSFeldmanRMVillanuevaGChuangAZA randomized double-masked trial comparing ketorolac tromethamine 0.5%, diclofenac sodium 0.1%, and prednisolone acetate 1% in reducing post-phacoemulsification flare and cellsOphthalmic Surg Lasers19982975395449674003
- AsanoSMiyakeKOtaIReducing angiographic cystoid macular edema and blood-aqueous barrier disruption after small-incision phacoemulsification and foldable intraocular lens implantation: multicenter prospective randomized comparison of topical diclofenac 0.1% and betamethasone 0.1%J Cataract Refract Surg2008341576318165082
- EndoNKatoSHaruyamaKShojiMKitanoSEfficacy of bromfenac sodium ophthalmic solution in preventing cystoid macular oedema after cataract surgery in patients with diabetesActa Ophthalmol201088889690019725815
- MiyanagaMMiyaiTNejimaRMaruyamaYMiyataKKatoSEffect of bromfenac ophthalmic solution on ocular inflammation following cataract surgeryActa Ophthalmol200987330030519183412
- WangQWYaoKXuWBromfenac sodium 0.1%, fluo-rometholone 0.1% and dexamethasone 0.1% for control of ocular inflammation and prevention of cystoid macular edema after phacoemul-sificationOphthalmologica2013229418719423429038
- PleyerUUrsellPGRamaPIntraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same?Ophthalmol Ther201322557225135807
- RothDBRealiniTFeuerWJShort-term complications of intravit-real injection of triamcinolone acetonideRetina2008281667018185140
- InataniMIwaoKKawajiTIntraocular pressure elevation after injection of triamcinolone acetonide: a multicenter retrospective case-control studyAm J Ophthalmol2008145467668118243153
- KaralezliABorazanMAkovaYAIntracameral triamcinolone ace-tonide to control postoperative inflammation following cataract surgery with phacoemulsificationActa Ophthalmol200886218318718162061
- KwakHWD’AmicoDJEvaluation of the retinal toxicity and pharmacokinetics of dexamethasone after intravitreal injectionArch Ophthalmol199211022592661736876
- DineenBBourneRRJadoonZCauses of blindness and visual impairment in Pakistan. The Pakistan national blindness and visual impairment surveyBr J Ophthalmol20079181005101017229806
- FisherBLPotvinRTranszonular vitreous injection vs a single drop compounded topical pharmaceutical regimen after cataract surgeryClin Ophthalmol2016101297130327486301
- AnJAKasnerOSamekDALévesqueVEvaluation of eyedrop administration by inexperienced patients after cataract surgeryJ Cataract Refract Surg201440111857186125248295
- BrownMMBrownGCSpaethGLImproper topical self-administration of ocular medication among patients with glaucomaCan J Ophthalmol1984191256608974