Abstract
Background:
The aim of the study was to examine the clinical success of high Dk (oxygen permeability) piggyback contact lens (PBCL) systems for the correction of contact lens intolerant keratoconus patients.
Methods:
Sixteen patients (29 eyes) who were not able to wear gas-permeable rigid lenses were included in this study. Hyper Dk silicone hydrogel (oxygen transmissibility or Dk/t = 150 units) and fluorosilicone methacrylate copolymer (Dk/t = 100 units) lenses were chosen as the PBCL systems. The clinical examinations included visual acuity and corneal observation by biomicroscopy, keratometer reading, and fluorescein staining before and after fitting the PBCL system.
Results:
Indications for using PBCL system were: lens stabilization and comfort, improving comfort, and adding protection to the cone. Visual acuities increased significantly in all of the patients compared with spectacles (P = 0). Improvement in visual acuity compared with rigid lenses alone was recorded in 89.7% of eyes and no alteration of the visual acuity was observed in 10.3% of the eyes. Wearing time of PBCL systems for most of the patients was limited time (mean 6 months, range 3–12 months); thereafter they tolerated rigid lenses alone except for 2 patients.
Conclusion:
The PBCL system is a safe and effective method to provide centering and corneal protection against mechanical trauma by the rigid lenses for keratoconus patients and may increase contact lens tolerance.
Introduction
Several clinical visual conditions that are difficult to correct with conventional rigid or soft contact lenses alone can be corrected with by using soft and hard lenses together. These conditions include keratoconus; postoperative refractive error including irregular astigmatism after corneal perforation or penetrating keratoplasty; ectasia or residual ametropia after refractive surgery; irregular ocular surface occurring with corneal ring implantation for keratoconus; and high korneal astigmatism with anisometropia.Citation1–Citation4 Piggyback or combination lenses are the terms used for the technique of fitting a rigid lens on top of a soft lens that acts as a “bandage”. Adding protection to the apex of the cone increases comfort and stabilization of rigid contact lenses over the irregular corneal surface.Citation5
Piggyback contact lens (PBCL) systems were first described in the early 1970s for patients with keratoconus who could not tolerate their scleral or rigid corneal lenses.Citation5,Citation6 The application of a soft lens as a bandage enables these patients to tolerate the rigid lens over the top of the soft lens. When these lenses were first introduced, the only lens materials available were of relatively low oxygen permeability and were often associated with corneal complications due to hypoxia. Recently, it has been shown that hyper Dk (oxygen permeability) soft and hard contact lens materials can provide enough oxygen to fulfill corneal oxygen requirements in PBCL systems.Citation7 Silicon hydrogel contact lenses have been used successfully in this system. Also hyper Dk rigid gas permeable (RGP) lens materials and aspheric designs are available for use in combination with silicone hydrogel lenses.
Our study was designed to examine the clinical success of this method for the correction of contact lens-intolerant keratoconus patients.
Materials and methods
Twenty-nine eyes of 16 patients (n) who were unable to wear gas-permeable rigid lenses with keratoconus were included in this prospective study.
Routine ophthalmogical examination was performed for all the patients before and after fitting the PBCL system. The clinical examinations included visual acuity (Snellen) and corneal observation by biomicroscopy, fluorescein staining, keratometer reading, and corneal topography (Nidek Magellan MapperR, Japan).
A first-generation silicone lotrafilcon A hydrogel lens with Dk/t (oxygen transmissibility) = 150 units (Focus Night and DayR; CIBA Vision, Atlanta, FL) with a steep base curve (8.40 mm) was selected to enable a more stable keratoconic topography; positive high diopters maintained better centering of the RGP lenses because of their steeper anterior surface while +0.50 D or plano soft lenses were fitted under the patients’ own RGP lenses. We also used negative powered lenses for patients who wanted to be able to use their soft lenses alone without their rigid lens on. A fluorosilicone methacrylate RGP copolymer with Dk/t = 100 units (Conflex keratoconus 100 UVR, Germany) was our RGP lens of choice.
The best soft bandage lens fit was determined until good centering was achieved. The suitable carrier soft lens was inserted, and keratometry readings were measured over the lens. To create the combination lens, the rigid lens with an aspheric posterior surface was placed on the soft contact lens according to the flat K value measured over the soft contact lens.
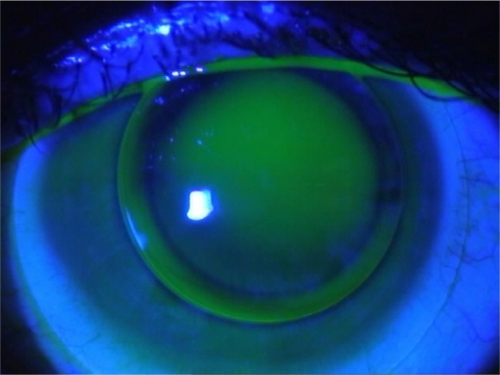
We considered that PBCL fitting was optimal when the rigid and soft lenses moved independently and correctly at each blink as determined by biomicroscopic examination and an acceptable fluorescein pattern with no touch ( and ). Lens fitting was successful during the first trial in most cases, but further attemps with various combinations were occasionally necessary.
Figure 1 A view of optimal piggyback contact lens fitting. The rigid and soft lenses move independently and correctly at each blink as shown by biomicroscopic examination.
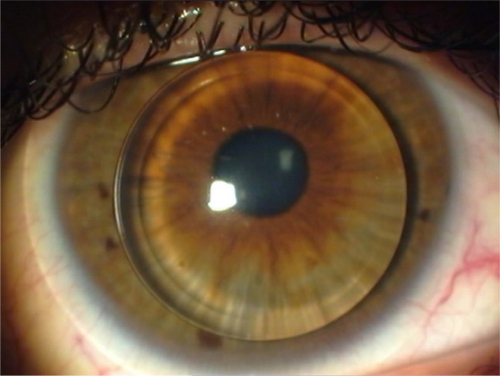
Figure 2 Fluorescein pattern of optimal piggyback contact lens fitting.
The patients were interviewed about changes in lens comfort before and after the fitting of soft contact lenses. They were instructed to clean their hard and soft contact lenses with the same soft contact lens cleaning solution to make wearing of 2 different lenses more practical. Patient education covered possible complications of the technique and they were required to have monthly examinations for at least 9 months.
Statistical analysis were performed with SPSS version 16.0 for Windows. Decriptive analysis was presented as mean ± standart deviation. Values were compared with Wilcoxon t-test. P values < 0.05 were regarded as statistically significant.
Results
The mean age was 28.3 ± 9.1 and male/female ratio was 10/6.
The mean values of the keratometric readings for K1, K2, and mean K were: 48.0 ± 63.7, 53.07 ± 5.1 and 50.4 ± 4.2 D in keratoconus patients. Twenty-nine keratoconic eyes were graded according to the Amsler classificationCitation8 as mild to very severe forms: 3 eyes mild, 16 eyes moderate, 9 eyes severe, and 1 eye very severe.
Soft lens dioptric powers ranged from +4.00 to −3.50 D (mean = 0.72 ± 1.6). Rigid gas permeable lenses mean base curves were 7.23 ± 0.64 mm (range: 6.0–7.90) in group 1 and RGP lenses diameters ranged from 8.50 to 9.80 mm (mean: 9.35 ± 0.40). Fluorescein pattern was acceptable in all of the patients with no touch and adequate movement. Indications for using PBCL system were as follows: 13 eyes for the purpose of lens stabilization and comfort, 5 eyes for improving comfort, and 11 eyes for adding protection to the cone ().
Table 1 Indications of the optimal piggyback contact lens system
Visual acuity with glasses ranged from 0.05 to 0.6 Snellen lines with a mean of 0.27 ± 0.15 lines (0.64 ± 0.29 logMAR) in keratoconus patients. Mean visual acuity with RGP lenses was 0.61 ± 0.14 lines (0.22 ± 0.11 logMAR), while mean visual acuity with piggyback lenses was 0.83 ± 0.12 lines (0.08 ± 0.06 logMAR) ().
Table 2 Visual acuity with glasses, rigid gas-permeable (RGP) lenses, and piggyback contact lenses according to Snellen lines and logMAR
Improvement in visual acuity compared with that of rigid lenses alone was recorded in 89.7% of eyes and no alteration of the visual acuity was observed in 10.3% of the eyes. Visual acuity of eyes was significantly better with piggyback lenses (W = −4.7, P = 0) than visual acuity of uncorrected and RGP-lens corrected eyes (W = −4.6, P = 0).
Wearing time per day ranged from 3 to 16 hours (mean 11.7 ± 2.8 hours).
PBCL systems for most patients were used for a limited time (mean 6 months, range 3–12 months); thereafter they continued with rigid keratoconus lenses (with aspheric or multicurve posterior surface design; Rose K brand lenses) alone as described before.Citation9 Two patients (3 eyes) have been using this system and cannot tolerate their hard lenses alone.
Complications observed were giant papillary conjunctivitis in 2 eyes, corneal epithelial erosions in 1 eye, and lost lens in 1 eye. Vascularization, which has been reported with low Dk lenses, was not seen in any patient. Complications after wearing the PBCL are shown in .
Table 3 Complications after wearing piggyback contact lenses
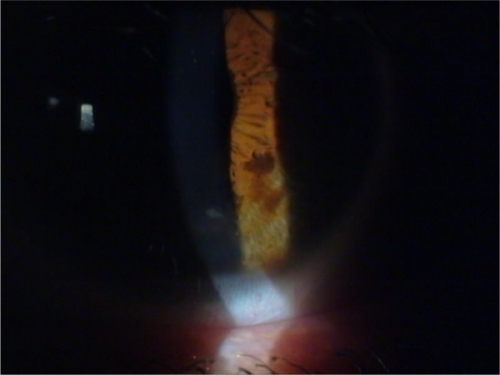
In 1 case, inferior paracentral epithelial erosions developed. after successfully using the PBCL system for a 7-month period. The patient stopped using the lenses for 3 days, then continued with a new steeper base curve RGP lens after the the epithelial erosions had been healed by the use of a bandage lens ().
Figure 3 Inferior paracentral epithelial erosions which developed as a complication of using the optimal piggyback contact lens fitting system successfully for a 7-month period.
Discussion
Rigid contact lenses offer significant improvements in optical performance over spectacle and hydrogel lenses for irregular corneas. The rigid front surface provides a regular spherical refractive surface.Citation10 However, the edge of the lens provokes lid sensation and may cause greater corneal insult, due to increased mechanical friction of the lens on the corneal epithelial surface and a greater degree of discomfort compared with hydrogel lenses. Hard contact lenses were difficult to wear because of the rigidity of the material and irregularity of ocular surface in our patients, which may make contact lens wearing uncomfortable and unstable in irregular corneal astigmatic conditions such as keratoconus.
The keratoconic cornea has multiple curves, a flatter superior paralimbal surface, an inferior paracentral ectatic area, and a steeper inferior paralimbal surface. As a result rigid lenses tend to slip inferiorly and stay without movement on the inferior part of the cornea and adhere to the corneal surface with the help of the pressure of eye lids during the blinking movement. Because of these comfort and stability problems some patients with irregular astigmatism, especially keratoconics, are unhappy and tend to quit their rigid lenses before they adapt to them and search for more radical surgical solutions for their condition. The main reasons for penetrating keratoplasty are contact lens intolerance (83%), frequent contact lens displacement (8.5%), and unsatisfactory visual acuity despite good contact lens fit (8.5%) in keratoconus patients.Citation11 Lens comfort and stability may be increased with other fitting options by the use of hybrid lens designs, scleral lenses, and piggyback lens systems. However the relatively low oxygen transmissibility and high cost of the hybrid lenses and lack of experience with scleral lenses limit their use.Citation12
The advantages of the PBCL system is that it reduces the mechanical trauma of the hard lens materials, improves patients’ tolerance, and heals the epithelial erosions, in combination with the comfort of a silicone hydrogel lens with the optical superiority of a rigid lens. In addition the system maintains optimal lens fitting and centering in patients with corneal irregularities, ectatic conditions (including unsuccessful refractive surgery), intracorneal rings, and penetrating keratoplasty.Citation2–Citation4
There have been few clinical studies on patients fitted with piggyback lenses and most of these have used the lenses to correct irregular astigmatism and contact lens intolerance. Mehta et alCitation13 published sucessful results in patients with irregular corneas: penetrating corneal keratoplasty (in 3 patients), penetrating corneal injury (in 1 patient), scarred cornea following herpes zoster (in 1 patient), and in 8 keratokonus patients fitted with a modified countersunk lens pigyback system. Randleman et alCitation14 has published a case report of piggyback hyper O2 contact lenses after severe alkali injury.
Soft lenses have a smoothing out effect on the multicurved irregularities of the corneaCitation1 and can act as a glider for a rigid lens of aspheric design with a rapid flattening effect at the periphery for a more optimal fit. On the other hand, Burger et alCitation15 propose that the irregular corneal topography is transmitted to the hydrogel lens front surface, which detracts from the fit of the rigid lens. This compromise in rigid lens fit results in poor centering and stability of the rigid lens, with too much movement leading to poor optical performance and too little movement preventing an adequate supply of oxygen to the corneal surface, thus compromising ocular health. For optimal fit, the rigid and soft lenses must move independently, which is of great importance in maintaining a sufficient supply of oxygen to the cornea.Citation1,Citation16
To make the soft lens more suitable to the ectatic and steep cornea, it has been suggested that a soft lens must have as steep a curve as possible. Kok and MilCitation1 used a soft bandage lens with a mean base curve radius of 8.90 mm (8.30–9.20); in our series we preferred a steeper fit mostly with 8.40 mm base curves, and we obtained optimal soft lens fitting in all cases.
It has also been suggested that a soft lens should have a positive dioptric power with a central steeper anterior surface to make the rigid lens stay more stable and move adequately on the surface of the soft lens.Citation17 We used positive diopter soft lenses in 22 eyes for this reason, but also used negative powered lenses for those who wanted to be able to use their soft lenses alone without their rigid lens on.
In our study, we included patients who were not able to tolerate gas-permeable rigid lenses because of their irregular corneal surface astigmatism. Wearing time of PBCL systems for most of the patients was limited (mean 6 months, range 3–12 months); thereafter they continued with rigid keratoconus lenses (with aspheric or multicurve posterior surface design) alone. We think that besides healing of the epithelial erosions by the use of a bandage lens, decreased sensitivity during PBCL wear may be the reason for the increase in RGP lens tolerance in these patients.
The main goal in fitting RGP lens is the optical correction of the irregular cornea, since spectacle correction is inadequate in this group of patients. In our study, visual acuities increased significantly in all patients compared with those with spectacles. It was thought that the reason for this improvement may be the decrease in irritation, lacrimation, and photophobia as a result of the mechanical effect of rigid lenses.
There are two main problems with PBCL systems: low oxygen transmission that can cause hypoxia and corneal vascularization;Citation18 and difficulties with using two different contact lenses. Another reported disadvantage of the piggyback lens system is lens displacement and loss.
Piggyback lenses result in a double barrier to oxygen supply over the corneal surface.Citation20 Therefore, both soft contact lenses and RGP lenses must have high oxygen permeability and optimal mobility. Research has indicated that the optimal oxygen transmissibility of the PBCLS must be greater than 60 mm Hg for daily use. Weissman and YeCitation19 calculated the tear oxygen tension under contact lenses offering resistance in series, and showed that soft and hard lenses with Dk/t values of 140 and 100 units, respectively, maintain oxygen tensions of 114 to 125 mm Hg, values that are much higher than the critical oxygen pressure of 100 mm Hg necessary for the cornea.
Due to their higher oxygen transmission, silicone hydrogel lenses are ideal for the PBCL system. With the hyper Dk silicone hydrogel (Dk/t = 150 units) and fluorosilicone methacrylate copolymer (Dk/t = 100 units) lenses used in this study we did not observe any sign of hypoxia such as hyperemia, vascularization, and corneal edema.
A limitation of the present study is the small sample size. Studies of contact lens-intolerant patients with larger sample sizes and comparing patients with other fitting options such as hybrid lens designs and scleral lenses with PBCLs may be helpful.
Our study shows that the PBCL system is a safe and effective method to provide centering and corneal protection against mechanical trauma for keratoconus patients and may also increase contact lens tolerance.
Disclosure
The authors have no financial interest with any of the products mentioned in the text.
References
- KokJHCMilCPiggyback lenses in keratoconusCornea19931260668458233
- O’DonnellCWelhamLDoyleSContact lens management of keratectasia after laser in situ keratomileusis for myopiaEye Contact Lens20043014414615499234
- SmithKACarrellJDHigh Dk piggyback contact lenses over intacts for keratoconus: A case reportEye Contact Lens20083423824118787433
- WietharnBEDriebeWTFitting contact lenses for visual rehabilitation after penetrating keratoplastyEye Contact Lens200430313314722466
- WesterhoutDThe combination lens and therapeutic uses of soft lensesContact Lens1973439
- PolseKADeckerMRSarverMDSoft and hard contact lenses worn in combinationAm J Optom Physiol Optics197754660665
- AlemanyAlMeijomeJMGAlmediaJBParafitaMARefojoMFOxygen transmissibility of piggyback systems with conventional soft and silicone hydrogel contact lensesCornea20062521421916371786
- AmslerMKeratocone classique et keratocone fruste, arguments unitariesOphthalmology194611196101
- Buyru ÖzkurtYŞengörTKurnaSRose K contact lens fitting for keratoconusInternational Ophthalmology20082839539817955181
- EdwardsKToric rigid lens problem solvingOptician19992172025
- LimNVogdtUCharacteristics and functional outcomes of 130 patients with keratoconus attending a specialist contact lens clinicEye200216545911913889
- OwensHWatersGGambleGEffect of softperm lens wear on corneal thickness and topography: a comparison between keratoconic and normal corneaeCLAO J200228838712054377
- MehtaMBhagwanjeeAHilliarOA clinical and optical evaluation of a modified lens for irregular corneaeClin Exp Optom2006891303616430438
- RandlemanJBWardMAStultingRDVisual rehabilitation after severe alkali injury with piggyback hyper contact lensesCornea2003218118312605059
- BurgerDSContact lens alternatives for keratoconus: an overviewCL Spectrum199334954
- FattIOxygen transmissibility considerations for a hard-soft contact lens combinationAm J Optom Physiol Optics197754666672
- O’DonnellCCodinaCMA hyper-Dk contact lens system for keratoconusEye Contact Lens200430444814722470
- DepaolisMDShovlinJPAkermanDHHybrid materials and designsBennettESWeissmanBAClinical Contact Lens PracticePhiladelphiaLippincott Williams & Wilkins2005475485
- WeissmanBAYePCalculated tear oxygen tension under contact lenses offering resistance in series: piggyback and scleral lensesContact Lens and Anterior Eye20062923123717064950
- FlorkeyLNFinkBAMitchellGLHillRMCorneal oxygen uptake associated with piggyback contact lens systemsCornea20072632433517413961