
Clinical refractive astigmatism (RA) and topography-measured anterior corneal astigmatism (ACA) are rarely identical in magnitude and axis.Citation1 This difference, when expressed vectorially, is termed ocular residual astigmatism (ORA).Citation1 What accounts for this difference remains a topic that needs further research, and has implications as to what refraction to treat with topography-guided excimer laser ablations in order to maximize outcomes.Citation1 This research letter investigates aspects of two contributing factors: posterior corneal astigmatism (PCA) and anterior corneal higher-order aberrations (CHOAs).
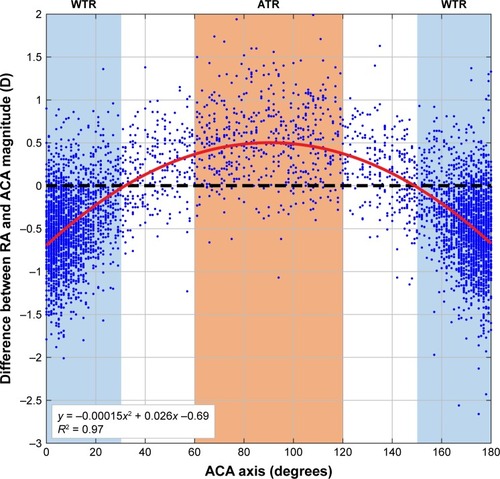
We compared RA to ACA magnitude in 5,403 eyes to reveal that 87% with-the-rule (WTR) corneal cylinder eyes had less RA magnitude than ACA magnitude, and 89% against-the-rule (ATR) corneal cylinder eyes had RA magnitude greater than ACA magnitude (). Published data show that 87% of corneas have ATR posterior corneal astigmatism,Citation5 which, if additive to ACA, could explain the decreased RA seen in most WTR corneal cylinder eyes, and the increased RA in most ATR corneal cylinder eyes (). Furthermore, our data show that the ACA axis location correlates to the amount of difference between RA and ACA (), supporting the notion that the interaction between ACA and PCA impacts RA by modifying the total corneal astigmatism.
Figure 1 Difference between RA and ACA magnitude (ie, RA magnitude – ACA magnitude) in relation to the ACA axis and quadratic fitting of this relationship (red curve). Data points (blue dots) above the black dashed line indicate eyes where the ACA is smaller than the RA magnitude, and below show eyes where the ACA is greater. Blue-shaded area: WTR-ACA eyes; red-shaded area: ATR-ACA eyes.
A recent paperCitation2 claimed that PCA does not contribute significantly to RA, while other publications have reported that PCA compensates between 22% and 31% of the ACA.Citation3,Citation4 A large cohort study revealed that PCA accounts for more than −0.5 D in 9% of eyes.Citation5 This magnitude of PCA cannot be taken as clinically negligible, particularly for eyes with a greater amount of cylinder. It is also why PCA is now used for intra-ocular lens surgical planning, with improved outcomes.Citation6 With topography-guided treatments, only treating the Contoura-measured ACA could allow the PCA to manifest as RA post-operatively, as can be seen with TORIC IOL surgery that ignores PCA.Citation6
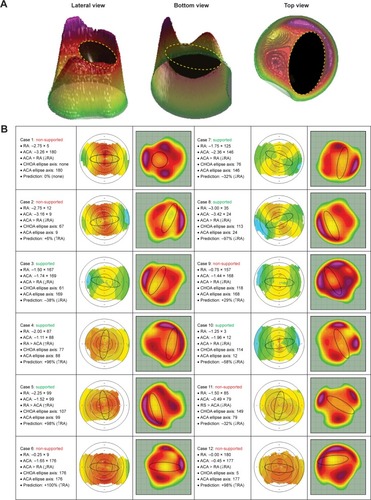
A recent series examined six eyes with significant ORA and theorized that anterior CHOAs were the cause of the discrepancy between RA and ACA.Citation2 For illustrative purposes, the author characterized CHOAs as creating an ovalization of the central cornea, interacting with an ovalization produced by ACA.Citation2 Depending on how these two ovals are aligned, the net RA will summate or negate.Citation2 To objectively investigate this claim, we developed an advanced algorithm that analyzed the Contoura (WaveLight® EX-500; Alcon Laboratories, Inc., Fort Worth, TX, USA) CHOA ablation profile in 3D, accurately detailing the CHOA ellipse (). We then studied the vectorial relationship between the calculated CHOAs and ACA ellipses in 12 eyes (). While we found six of 12 cases that supported the summation notion, we also found six contradictory cases, and could therefore not validate this theory (). This was illustrated in cases 2, 6, 9, and 12, where ellipses with similar orientations should have summated and increased the RA, but did not. For case 11, the ellipses with perpendicular orientation should have partially canceled each other, but did not. Case 1 is an example that could not be fitted by an ellipse as the pattern was circular. While we agree that CHOAs also affect RA, a concept previously reported by Zhou et al,Citation7 the claim that ORA is mainly accounted for by anterior CHOAs in the large majority of eyesCitation2 is not supported by the current research letter’s findings or by previous litterature.Citation1,Citation3–Citation6
Figure 2 (A) Objective algorithm-based identification of a 3D ellipsoid in a representative Contoura CHOA ablation profile visualized at different angles. The CHOAs’ ellipse axis was calculated using the top view. (B) Case series of 12 eyes used to test Motwani’s claim. Left column, eye parameters; middle column, topographical corneal astigmatism where the ovalization is indicated by a black ellipse; right column, CHOAs’ profile where the ovalization is indicated by a black ellipse as in Motwani’s work.Citation2 Vectorial analyses were used to predict the effect of the interacting ellipses on RA as a positive or negative percentage change, setting both ellipses at equal magnitude. “Supported” and “Non-Supported” identify cases where Motwani’s claim is validated or not, respectively.
The difference between RA and ACA is thought to be attributed to several factors, including anterior CHOAs, PCA, anterior and posterior lenticular astigmatism, refractive index variability, decentration of the crystalline lens, as well as from retinal tilt and cortical perception.Citation1 Contoura topography-guided software determines the anterior CHOAs and the true ACA from a high resolution Placido disc topographer. The Contoura-measured ACA does not consider the manifest RA and does not supply information on how anterior CHOAs influence RA. RA encompasses all sources of astigmatism, from the anterior cornea to the brain. Since Contoura treatments partially remove anterior CHOAs, to produce a more accurate nomogram for topography-guided ablations, one would need to fully elucidate – possibly using ray tracing technology – the contribution of anterior CHOAs to manifest RA, as well as the effects of PCA and the remaining internal optics.
Disclosure
The authors report no conflicts of interest in this work.
References
- AlpinsNPractical Astigmatism Planning and AnalysisSLACK IncorporatedThorofare, NJ, USA2017
- MotwaniMThe use of WaveLight® Contoura to create a uniform cornea: the LYRA Protocol. Part 1: the effect of higher-order corneal aberrations on refractive astigmatismClin Ophthalmol20171189790528553069
- AtchisonDAMarkwellELKasthuriranganSPopeJMSmithGSwannPGAge-related changes in optical and biometric characteristics of emmetropic eyesJ Vis2008829429120
- DubbelmanMSicamVAvan der HeijdeGLThe shape of the anterior and posterior surface of the aging human corneaVision Res2006466–7993100116266736
- KochDDAliSFWeikertMPShirayamaMJenkinsRWangLContribution of posterior corneal astigmatism to total corneal astigmatismJ Cataract Refract Surg201238122080208723069271
- ReitblatOLevyAKleinmannGAbulafiaAAssiaEIEffect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: Comparison of methodologiesJ Cataract Refract Surg201642221722527026445
- ZhouWStojanovicAUtheimTPAssessment of refractive astigmatism and simulated therapeutic refractive surgery strategies in coma-like-aberrations-dominant corneal opticsEye Vis2016313