Abstract
Background:
This study aimed to find the strength of the correlation between ORange® (intraoperative wavefront aberrometer) objective refraction during pseudophakic cataract surgery (Gen 1) and 1-week objective autorefraction postcataract surgery in order to establish the clinical degree of confidence in the ORange. Gen 1 was used because Gen 2 was not available at the time of the study. However, Gen 1 can still be a good reference.
Methods:
Thirty-two consecutive eyes were included in this prospective nonrandomized study. ORange was used after phacoemulsification and intraocular lens implantation. There were no complications and no withdrawals from the study. The refraction data from the ORange were recorded in spherical equivalents and put into Excel. One week postoperatively, autorefraction was done and the data were again recorded in spherical equivalents and put into Excel. Both sets of data were then transferred to SPSS for a correlation study. Because ORange is an objective refractor, it is necessary to use another objective refractor, such as the Zeiss Autorefractor, for comparison. Measurement at 1 week postoperatively is for cornea clearance for autorefraction and is the closest time to intraoperative assessment for comparison.
Results:
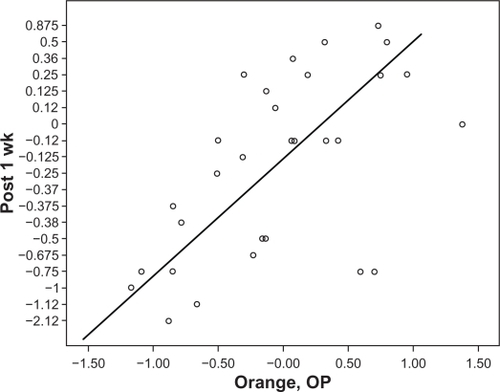
The Pearson correlation was r = +0.56, P < 0.01, which qualifies for a moderate or good correlation (0.5–0.75).
Conclusion:
Intraoperative refraction using the ORange Gen 1 after cataract surgery and intraocular lens implantation is moderate to good when correlated with objective autorefraction 1 week after cataract surgery.
Introduction
The intraoperative wavefront aberrometer (ORange®; WaveTec Vision Inc, Aliso Viejo, CA) incorporates a Talbot–Moiré interferometer to enable cataract surgeons to check a patient’s refraction during surgery. The Talbot–Moiré interferometer is different from other wavefront technologies, such as Hartmann–Shack, in that it uses optical and mathematical principles to capture and analyze a wavefront. The wavefront passes through a pair of gratings set at a specific distance and angle offset to each other. The diffraction of the wavefront as it passes through the grating pair produces a fringe pattern. Aberrations cause distortions in the fringe pattern, and after being analyzed, are translated into the refractive value. Using this equipment at the time of surgery, cataract surgeons can achieve more precise power in the intraocular lens or change the axis of a toric intraocular lens and make sure the power of the intraocular lens is reasonably correct during the operation. It can also adjust limbal relaxation incision in both length and axis to enhance correction of astigmatism.Citation1 Surgeons will be more confident using ORange when pursuing precision of refraction outcome after cataract surgery with a premium intraocular lens to achieve independence of glasses.
Figure 1 Scatter plot of ORange® refraction in surgery against 1-week postoperative refraction with Zeiss autorefractor.
The Gen 1 ORange can perform real-time refraction after intraocular lens implantation (pseudophakic) while Gen 2 can perform refraction before intraocular lens implantation (aphakic).Citation2,Citation3 The problem with Gen 1 is that the surgeon needs to exchange the intraocular lens if the refraction reading from the ORange is unacceptably different from the proposed refraction. It would require a high level of confidence in the ORange for surgeons to be able to decide to exchange the intraocular lens during surgery.
Many limitations apply in performing the ORange, including too small a pupil, corneal disease, foveal disease, wound leakage, nystagmus, local block, and use of lidocaine gel. Because the ORange is an objective refractor in the operating room and the Zeiss autorefractor (Humphrey automatic refractor keratometer Model 599) is a popular objective refractor in the office, it is reasonable to correlate the two sets of refractive data. However, there are many differences in refraction between the ORange and Zeiss autorefractor, including the patient’s position, corneal edema, and pupil size. Because of a shortage of nonbiased published comparative studies of the ORange and other refractors, this study aimed to determine the direction and strength of the correlation between pseudophakic refraction measurement using the Gen 1 ORange during intraoperative cataract surgery and measurement at 1-week postcataract surgery in pseudophakic refraction using the Zeiss autorefractor in order to establish a degree of confidence in the usage of the ORange.
Methods
Thirty-two consecutive eyes from an equal number of male and female patients aged 58–85 years were included in this prospective study done in July 2009. Gen 1 ORange was used after cataracts were removed by phacoemulsification, with intraocular lens implantation (pseudophakic) by one surgeon at the Surgical Suite, Honolulu, Hawaii. All the subjects had standard phacoemulsification of 2.4 mm cornea temporal incision, a 5.5 mm capsulorhexis with implantation of an Acrysoft single-piece intraocular lens (Alcon, Fort Worth, TX) in the bag. The aim was to standardize the intraocular lens in the bag.
Inclusion criteria were: being scheduled for cataract surgery with a standard intraocular lens; availability to be followed up at 1 week after cataract surgery; and willingness to participate in the study. Exclusion criteria were: cataract surgery with complications, eg, vitreous loss, dislocation of intraocular lens, or intraocular lens placed in the ciliary sulcus; abnormal pupil, eg, irregular pupil (due to inflammation or surgical complication), tonic pupil, or pupil smaller than 1 mm to take away the pupil factor in affecting refraction; abnormal cornea, eg, cornea opacity, keratoconus, to take away the cornea factor in affecting refraction; abnormal active vitreous retina disease, eg, vitreous hemorrhage, retinopathy; severe refractive errors, eg, high myopia, hyperopia, or astigmatism; being scheduled for multifocal, accommodative, or toric intraocular lens implantation after cataract surgery; mature or hypermature cataract; and previous refractive surgery. The study was approved by the Institutional Review Committee of the University of Hawaii for ethical issues and adhered to the tenets of the Declaration of Helsinki.
There were no complications or withdrawals from the study. Refraction data after cataract surgery with intraocular lens implantation by the ORange (objective) were recorded in spherical equivalents and put into Excel (Microsoft, Redmond, WA) by a nurse in the operating room. One week postoperatively, refraction was measured by a technician in the office using a Zeiss autorefractor (objective) and the data were entered as spherical equivalents into Excel. A single designated Zeiss autorefractor was used for autorefraction and was performed by a single designated technician. The technician was blinded by being given a numbered form with no record of the subject’s name, intraocular lens type, or any other information accompanying the printout of the refraction. This form was also used to maintain patient anonymity. Use of a single surgeon, a single surgical center, a single technician, and single equipment prevented the possibility of interrater disagreement. Because ORange Gen 1 is an objective refractor, the Zeiss autorefractor was utilized for the purposes of comparison. The Zeiss autorefractor is designed to measure refraction errors in human eyes objectively by using infrared light at 880 nm. The unit was made by Carl Zeiss (Zeiss AG, Stuttgart, Germany) in 1997. There are over 20,000 such units in the US. The designated unit for this study had been serviced and calibrated for accuracy about three months earlier. Both sets of data entered into Excel were then transferred to SPSS software (SPSS Inc., Chicago, IL) for statistical analysis.
Table 1 Results
Because the surgeon selected the intraocular lens power preoperatively mostly for mild myopia, both the ORange and Zeiss autorefractors had minus power in spherical equivalents. One week postoperatively the pupil had already constricted, which might be the reason why the Zeiss autorefractor had more negative readings.
Discussion
Despite many differences between intraoperative ORange and postoperative Zeiss refraction, the Pearson correlation coefficient showed a moderate to good correlation between the two instruments. It is reasonable to use the ORange Gen 1 intraoperatively as a reference for difficult cases, eg, outliers from previous refractive surgery or with a cornea abnormality. The optimization of ORange or A constant of the intraocular lens in Gen 2 for aphakia can minimize the difference to establish a higher correlation. Gen 2 ORange can be used for aphakic eyes to verify the power of the intended intraocular lens before implantation to avoid the need for future lens exchange. It has been reported that 93% of patients with a history of Lasik evaluated with ORange Gen 2 during cataract surgery showed a difference of less than 1 D between predicted intraocular lens power and one-month postoperative refraction.Citation5
Further correlation between the suggested intraocular lens power by ORange Gen 2 from intraoperative aphakic refraction and the intraocular lens master suggested intraocular lens power is currently being studied by the author. Because the intraocular lens master has already established a high level of accuracy in intraocular lens power, if the power from Gen 2 can demonstrate a high correlation with the intraocular lens power suggested by the intraocular lens master, we can establish a good level of confidence in the ORange.
Conclusion
ORange Gen 1 can be used to verify intraocular lens power during surgery to prevent “surprise” postoperative refraction. The intraoperative refraction with ORange in pseudophakic (Gen 1) is positively correlated to a moderate to good degree with postoperative refraction measured by the Zeiss autorefractor 1 week postoperatively.
Disclosure
The author reports no conflict of interest in this work.
References
- PackerMEffect of intraoperative aberrometry on the rate of postoperative enhancement: A retrospective studyJ Cataract Refract Surg201036574775520457365
- Data on file at WaveTec Vision; Aliso Viejo, CA. 80022, 80020, 80037, 80036.
- WileyWRetrospective and prospective comparison of outcomes before and after initial use of ORangePresented at the 113th annual meeting of the American Academy of OphthalmologySan Francisco, CAOctober 24–27, 2009
- FinkAHow to Analyse Survey DataThousand Oaks, CASage Publications1995
- SolomonRA study in the ORange intraoperative wavefront aberrometer (WaveTec Vision Systems) to make IOL power calculations in eyes that had undergone laser vision correctionPresented at the American Society of Cataract and Refractive Surgery annual meetingSan Diego, CAApril 28–May 2, 2001