
Abstract
Purpose
To report cost reductions of vitrectomy under local anesthesia.
Patients and methods
This was a retrospective cohort study using medical records of consecutive patients undergoing vitrectomy surgery for retinal detachment under general or local anesthesia. Data of patient’s fulfilling the inclusion criteria were included in the study. The patients were divided into two groups: Group 1 (local anesthesia) and Group 2 (general anesthesia). The preoperative data were checked and validated by a peer group consisting of two ophthalmologists, two internists, and two anesthesiologists independently in a blind manner. The calculation of the cost was done using the cost minimization analysis. The cost data were obtained from the finance division of the hospital for each individual treatment. The cost data included unit cost of laboratory tests, surgery, and medications.
Result
There were 100 subjects (50 subjects in each group) assessed by peer groups and declared eligible to undergo surgery under either local or general anesthesia. Both groups were equal. The total average cost for vitreous surgery under general anesthesia for each patient was $322.17, whereas for local anesthesia it was $220.57. The mean difference was $101.60 (46.06%) saving on local anesthesia.
Conclusion
Vitrectomy surgery under local anesthesia can reduce the cost by almost half that of general anesthesia. The present study showed that the type of anesthesia determined the ultimate cost for the surgery. Hence, surgery under local anesthesia appears affordable and cost-effective, especially in a developing country like Indonesia.
Introduction
The prevalence of blindness in Indonesia is currently estimated at 3.2% based on Rapid Assessment of Avoidable Blindness (RAAB) research in several provinces in Indonesia.Citation1 Of these, some were permanent, and the rest was treatable blindness. Incurable blindness was mostly due to late presentation and inadequate treatment, secondary to retinal diseases, glaucoma, infections, and other diseases.
The incidence of retinal detachment (RD) is estimated as one case in every 10,000 per year.Citation2 A population-based study in Singapore reported that out of 1,126 vitrectomized patients in 3 years (1993–1996), the incidence based on their ethnic origin was 7.0 per 100,000 in Malays, 11.6 per 100,000 in Chinese, and 3.9 per 100,000 in Indians.Citation3 This is similar to the ethnicity group in Indonesia. Based on the above report, it can be estimated that RD in Indonesia is between 17,500 and 25,000 new cases per year. However, the national report of the number of RD surgeries per year is not available in Indonesia.
Ideally, the sufficient number of ophthalmologists required to serve a population should be one in every 28,000, as reported by Bellan and BuskeCitation4 using the Canadian Medical Association Physician Resource Evaluation template. Based on the ratio of retinal physician/ophthalmologist ratio being 1:3–5, approximately 1,600–2,800 vitreoretinal (VR) doctors are required in Indonesia to serve its population of 230 million people. Currently, there are 46 ophthalmologists who can perform VR surgery in Indonesia [InaVRS-Perdami 2017, official communication]. Since the number of VR surgeons in Indonesia is limited, management of treatable VR disease requires optimization in terms of time, affordability, cost-effectiveness, and access to care. One such factor could be reduction of operating time by using local anesthesia, thus allowing the treating surgeon to perform more surgeries as well as possibly reduce the cost burden to the patients and the health care system.
It is known that the risk and cost are less with local anesthesia. There are several benefits of vitrectomy performed under local anesthesia as opposed to general anesthesia. The benefits include shortened duration of hospitalization, simpler preoperative preparation, cutting down of operating costs, and shorter operating times from preoperative preparation until the patient leaves the operating room (OR).
Previously, no researchers have ever reported the magnitude of cost reductions of vitrectomy under local anesthesia.Citation5 We conducted this study to answer this query. With the above hypothesis, we conducted a retrospective analysis of medical records data with the aim of assessing the cost-effectiveness of VR surgery for RD under local and general anesthesia in a developing country like Indonesia.
Patients and methods
This was a retrospective cohort study using medical records of consecutive patients undergoing vitrectomy surgery for RD using general anesthesia (Cipto Mangunkusumo General Hospital) and local anesthesia (Cikini CCI Hospital) in the city of Jakarta, Indonesia. The study was conducted in compliance with the tenets of the Declaration of Helsinki. The Christian University of Indonesia Institutional Review Board granted approval for this retrospective study. Patients’ informed consents were waived from this study since there was no patient intervention done and the study ensured patient data confidentiality.
The inclusion criteria were primary surgery for RD, complete availability of laboratory presurgery data, compliance to payment, preanesthetic chest and cardiac examination, and consent for the surgery. Only patients operated on once and who had completed 3-month follow-up were included.
Patients with systemic diseases such as diabetes or cardiac disease that may affect the choice of surgery were excluded in the data analysis. Patients who sought treatment for two or more ocular problems were also excluded. This was to avoid any extra cost in cost analysis for RD surgery. The patients were divided into two groups, Group 1 (Local Anesthesia) and Group 2 (General Anesthesia). Only cases that were operated on by surgeons with 2 or more years of experience were included. Therefore, the surgeries conducted at each eligible hospital and the preoperative conditions were comparable.
The baseline characteristics for each patient included age, education, socioeconomic background, and the general condition of the subject. Ocular examination data included initial visual acuity, posterior segment status (proliferation/ inflammation, retinal tear size, RD duration), and presence of cataract.
Preanesthetic examination included patient’s physical examination, laboratory examination, and chest and cardiac examination. Laboratory investigations included complete blood count, echocardiogram, and chest X-ray for local anesthesia and complete blood count, echocardiogram, chest X-ray, Serum Glutamic Oxaloacetic Aminotransaminase/Aspartate Aminotransferase/Serum Glutamic Pyruvic Transaminase (SGOT/SGPT), blood urea/creatinine and electrolyte, and urinalysis for general anesthesia.
The eligibility for either local or general anesthesia was checked and validated by the peer groups consisting of two ophthalmologists, two internists, and two anesthesiologists independently in a blind manner following the agreement, and then the patient was included in the study analysis. A subject would become a case study only if two doctors from each peer group were in agreement on the choice of anesthesia, after reviewing the retrospective data. A mixture of 2 mL of 2% lidocaine and 3 mL of bupivacaine was injected in the peribulbar space through incisure supraorbital and infraorbital notch. The activity-based pricing of general anesthesia for 2 hours as agreed by the anesthesiologists peer group included premedication (midazolam injection, fentanyl injection, ondansetron injection), anesthesia induction (propofol injection, atracurium injection), maintenance, recovery, and disposable goods.
Cost minimization analysis approach was used in this study. The calculation of the cost was from the hospital’s perspective. The cost data were obtained from the finance division, because each hospital already has a unit cost of each data sought including the unit cost of laboratory tests, surgery, and treatment. Direct medical costs calculated in Indonesian Rupiah were converted to US dollars for each of the patients. It was divided into three categories namely 1) preparation costs including consulting fees, medicines, and investigations (laboratory, X-rays, etc); 2) operating costs including the cost of local or general anesthesia, consumables, and cost of physician services; and 3) the cost of care, consultation, and medication after surgery. Based on the calculations, the lowest cost was the procedure of choice.
The data were analyzed using the SPSS version 21 (IBM Corporation, Armonk, NY, USA). Assuming a 5% significance level (α=0.05) and power of 80% (β=0.20) to detect proportional differences in cost between two groups, a sample size of 50 patients per group was required. Statistical analysis was performed by using Student’s t-tests. A P-value <0.05 was considered statistically significant.
Results
There were 55 subjects from the group of patients who underwent surgery under local anesthesia that met the inclusion criteria. Of these, three subjects were excluded because of comorbidities, diabetes mellitus (one subject), hypertension (one subject), and renal disease (one subject). Of the remaining 52 subjects, two subjects were excluded because of incomplete records (one subject), and optical media opacity (one subject). A total of 50 subjects were finally included in the study (Group 1: local anesthesia).
In the general anesthesia group, 71 subjects were eligible based on the inclusion criteria. After screening, only 63 were eligible. A total of eight subjects were excluded because of accompanying illnesses, namely diabetes mellitus (3), hypertension (3), and other diseases (2) that required examination and treatment other than vitrectomy surgery. Of the 63 subjects 13 were again excluded because of incomplete records. Hence, total of 50 subjects were included in Group 2 (general anesthesia). shows the baseline characteristics of both Groups 1 and 2.
Table 1 The characteristics of the basic preoperative conditions comparison between patients with general anesthesia and a local anesthetic
Local anesthesia and general anesthesia cost components were the same, covering the cost of preoperative (physician services, screening), intraoperative (anesthesia physician services and anesthetic materials), and postoperative (treatment, drugs) procedures. The finance division of both the hospitals had a unit cost data, and that data were obtained.
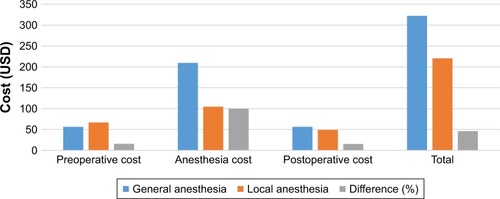
From the calculations, the total cost for general anesthesia (Group 2) was USD 322.17, and it was USD 220.57 for local anesthesia (Group 1) (). The total cost savings was equal to 46.06%. Based on the calculation, local anesthesia was the procedure that was found to be more affordable by the patients (). Anesthesia procedure is the biggest driver of cost. It was thus shown that the use of local anesthesia as opposed to the use of general anesthesia can reduce the cost by 100% ().
Table 2 The compiled cost data and differences between the two anesthetic methods
Figure 1 Comparison of cost component, showing that anesthesia cost has greater difference, as cost driver between local vs general anesthesia.
Discussion
Bupivacaine and lidocaine are local anesthesia agents commonly used. Bupivacaine has the advantage of a long duration of action, but it is inferior for the onset of anesthesia when used alone.Citation6,Citation7 Meanwhile, lidocaine provides a rapid onset of analgesia and akinesia, but has a shorter duration.Citation8 So, the mixture with equal volumes of bupivacaine and lidocaine is often used for a quick onset of anesthesia and a prolonged duration of action. This duration of action can be prolonged by additional subtenon injection of lidocaine during local anesthesia surgery, or during general anesthesia for pediatric VR surgery.Citation9,Citation10 In this study, we used a mixture of 2% lidocaine 2 mL and 3 mL bupivacaine injected through two point peribulbar injections (supraorbital and infraorbital notch).
The local anesthesia also has become a choice or alternative to general anesthesia in other procedures. It was also reported in cardiac procedures,Citation11 biopsies of brain,Citation12 and umbilical hernia.Citation13 The recovery time after local anesthesia is faster compared to general anesthesia, and it can be different based on the general anesthetic agent being usedCitation14 or type of procedure done.Citation15 One of the major complications of local anesthesia injection is inadvertent globe penetration.Citation16
In terms of adverse events, the most important surgeon-controlled factors are surgical time, type of anesthesia, and site of surgery.Citation17,Citation18 As long as the outcome is comparable, local anesthesia is the choice. Although there are reports of topical anesthesia for vitrectomy, their use is limited to symptomatic floaters, and using 27 G instruments.Citation19,Citation20 So far, local anesthesia is still an alternative and a safe procedure compared to general anesthesia, as also shown in other studies.Citation21
Rhegmatogenous RD has long been the defining target of surgical retinal efforts. Chang and SmiddyCitation22 have reported the parameters of cost-effectiveness using Markov decision tree analysis for methods of RD repair. The analysis demonstrated that when factors included clinical visits and subsequent cataract surgery, the cost of repair of RD ranged from $2,763 to $7,940 depending on the treatment modality, practice, and surgical setting. The study demonstrated high level of cost-effectiveness of RD repair regardless of technique being used. A primary pars plana vitrectomy without scleral buckling was assumed in this model to have a 90% success rate. For facility cases performed in a hospital OR, the Markov analysis demonstrated a modeled cost of $5,425 in this setting. Primary pars plana vitrectomy in the nonfacility setting, operated in an Ambulatory Surgery Center (ASC) OR, with the same success rate as described above, demonstrated a weighted cost of $4,048.
It is necessary to explore cost minimization analysis of the vitrectomy, performed under local vs general anesthesia. In our study, anesthesia procedure () was the largest cost driver. Our results shows that the use of local anesthesia can reduce the cost by 100% compared to general anesthesia, and the total cost of the procedure was reduced by 46.6%. If extrapolated to the population in Indonesia, there will be a saving nationally of USD 1,778,000–2,590,000 per year for RD vitrectomy procedures alone.
The drawback of a retrospective cohort study is, instead of starting from exposure, the data are available without any prior design. However, there was no difference in equality comparison made, as analyzed in the laboratory result, declared by anesthesiologist and internal medicine doctor. The eye condition itself was also equal, as declared by the peer group of ophthalmologists, so that no differences were seen in the choice of undergoing either general or local anesthesia.
There were several limitations to this study. First, the study obtained primary data from two hospitals only, both tertiary care centers, which may not be representative of all Indonesian hospitals. A larger sample drawn from more diverse health institutions is recommended. The Indonesian Ministry of health hospitals should consider the actual cost instead of subsidised cost. Second, this study addressed only direct medical costs incurred in the ward, operating theater, pharmacy, and outpatient clinic.
Conclusion
In conclusion we report that vitrectomy under local anesthesia can reduce the cost by almost half that of general anesthesia. Thus, VR surgery for RD repair under local anesthesia appears more cost-effective than general anesthesia, especially in developing countries.
Acknowledgments
We thank Djonggi P Panggabean and Esther Sianipar for editing the language.
Disclosure
The authors report no conflicts of interest in this work.
References
- DasTAcklandPCorreiaMIs the 2015 eye care service delivery profile in Southest Asia closer to universal eye health need!Int Ophthalmol201838246948028255837
- MichaelsonICSteinRA study in the prevention of retinal detachmentAnn Ophthalmol1969149
- WongTYTielschJMScheinODRacial difference in the incidence of retinal detachment in SingaporeArch Ophthalmol1999117337938310088817
- BellanLBuskeLOphthalmology human resource projections: are we heading for a crisis in the next 15 years?Can J Ophthalmol2007421343817361238
- LicinaASidhuSXieJWanCLocal versus general anaesthesia for adults undergoing pars plana vitrectomy surgery. Cochrane Database Syst Rev20169CD00993627641718
- BusbeeBGBrownMMBrownGCSharmaSCost-utility analysis of cataract surgery in the second eyeOphthalmology2003110122310231714644712
- ZandFRazavizadehMRAzematiSComparative study of onset and duration of action of 0.5% bupivacaine and a mixture of 0.5% bupivacaine and 2% lidocaine for epidural anaesthesiaActaMedicaIranica200442256258
- OjiEOjiABupivacaine and lignocaine for ophthalmic surgeryBr J Ophthalmol198771166683814573
- ChhabraASinhaRSubramaniamRChandraPNarangDGargSPComparison of sub-Tenon’s block with i.v. fentanyl for paediatric vitreoretinal surgeryBr J Anaesth2009103573974319706631
- GhaiBRamJMakkarJKWigJKaushikSSubtenon block compared to intravenous fentanyl for perioperative analgesia in pediatric cataract surgeryAnesth Analg200910841132113819299775
- JabbarAKhuranaAMohammedALocal Versus General Anesthesia in Transcatheter Aortic Valve ReplacementAm J Cardiol2016118111712171627692595
- Quick-WellerJKonczallaJDuetzmannSGeneral Anesthesia Versus Local Anesthesia in Stereotactic Biopsies of Brain Lesions: A Prospective Randomized StudyWorld Neurosurg201797162027671885
- JairamAPKaufmannRMuysomsFJeekelJLangeJFThe feasibility of local anesthesia for the surgical treatment of umbilical hernia: a systematic review of the literatureHernia201721222323128108822
- MirAHShahNFDinMULangooSAReshiFAEffectiveness of sodium thiopentone, propofol, and etomidate as an ideal intravenous anesthetic agent for modified electroconvulsive therapySaudi J Anaesth2017111263128217049
- JainRAShettyANOakSPWajekarASGarasiaMBEffects of avoiding neuromuscular blocking agents during maintenance of anaesthesia on recovery characteristics in patients undergoing craniotomy for supratentorial lesions: A randomised controlled studyIndian J Anaesth2017611424728216703
- WearneMJFlaxelCJGrayPSullivanPMCoolingRJVitreoretinal surgery after inadvertent globe penetration during local ocular anesthesiaOphthalmology199810523713769479301
- MazinaniBARajendramAWalterPRoesslerGFDoes surgical experience have an effect on the success of retinal detachment surgery?Retina2012321323722198301
- GoldfarbCABansalABrophyRHAmbulatory Surgical Centers: A Review of Complications and Adverse EventsJ Am Acad Orthop Surg2017251122228002212
- LinZMoonasarNWuRHSeemongal-DassRR27-Gauge Vitrectomy for Symptomatic Vitreous Floaters with Topical AnesthesiaCase Rep Ophthalmol201781353928203195
- LamDSLeungHYLiuSRadkeNYuanYLeeVYTwo-Port Pars Plana Anterior and Central Core Vitrectomy (Lam Floaterectomy) in Combination With Phacoemulsification and Intraocular Lens Implantation Under Topical Anesthesia for Patients with Cataract and Significant Floaters: Results of the First 50 Consecutive CasesAsia Pac J Ophthalmol2017613336
- SimanjuntakGWSSurgical Result of Pseudophakic Retinal Detachment in Cikini CCI Hospital-School of Medicine Christian University of IndonesiaJ Ophthalmol Indonesia2009725256
- ChangJSSmiddyWECost-effectiveness of retinal detachment repairOphthalmology2014121494695124411577