Abstract
Objective:
To determine the indications and rate of acceptance for destructive eye surgeries at the ophthalmology unit of the Yaoundé Gynaeco-Obstetric and Paediatric Hospital.
Methods:
A retrospective consecutive case series in which the medical records of all patients consulting in this unit over a 9-year period (2002 to 2010) were reviewed. Records in which destructive surgery was recommended were retained. Information collected included demographic data, eye affected, clinical diagnosis, acceptance or refusal of surgery, and the outcome in those in whom surgery was performed.
Results:
A total of 48 patients had a recommendation for destructive eye surgery, of whom 30 (62.5%) were males and 18 (37.5%) were females. Mean age was 43.78 (SD = 28.11; range 1 month to 91 years). Children <10 years comprised 23.10%. The leading causes were endophthalmitis/panophthalmitis (47.9%), neoplasm (20.8%), and absolute glaucoma (14.6%). Surgery was done in 20 cases (41.7%). Evisceration was the most performed surgical procedure (50%), with endophthalmitis/panophthalmitis and neoplasm combined accounting for 65% of surgeries.
Conclusion:
The high rate of refusal is an indication of the psychological devastation undergone by patients or the families of children in whom eye removal is recommended. Awareness should be raised on preventive measures and the need to rapidly seek eye care.
Introduction
Destructive eye surgeries include evisceration, enucleation, and exenteration. Evisceration is the removal of the internal eye contents, with the sclera left behind; enucleation is the removal of the eyeball, leaving the orbital contents in place; amd exenteration is the removal of the orbital contents, including the eyeball.Citation1
The decision for this surgery is a difficult one for both the patient and the physician, hence these procedures are recommended only as a last resort. Besides the clinical indication, the physician has to consider the visual potential of the eye, the potentials for complications and the patient’s psychology.Citation2 Removal of the eye may be necessary after a severe eye injury, to treat intraocular malignancies, in endophthalmitis/panophthalmitis unresponsive to medical treatment, as relief to a blind painful eye, and in cosmetic improvement of a disfigured eye. Evisceration and enucleation are both excellent in relieving pain in a blind painful eye,Citation3 in treating an infection, or in improving cosmetic appearance.Citation4 Enucleation is the procedure of choice in advanced intraocular tumors and in cases in which conservative therapy has failed.Citation5,Citation6 Exenteration is reserved for orbital tumors and intraocular tumors with spread to orbital contents.
The relative indications for these procedures vary from place to place. In many developed countries, the most important causes are tumors, whereas in developing countries, these are often infectious or traumatic.Citation7 A similar trend was reported by Epee et al at the University Teaching Hospital of Yaoundé.Citation8
It can be psychologically devastating to lose an eye and no study to the best of our knowledge has assessed the rate of acceptance of these procedures, as many patients refuse eye removal despite severe intractable pain or the risk of spread of an infection or malignancy. This study aimed to report the indications for destructive eye surgeries and the rate of acceptance by patients at the Yaoundé Gynaeco-Obstetric and Paediatric Hospital (YGOPH).
Patients and methods
This was a retrospective study over a period of 9 years (January 2002 to December 2010) carried out at the ophthalmology unit of the YGOPH. This hospital is a tertiary referral hospital with different specialties, including ophthalmology. The ophthalmology unit receives patients of all ages and sex. All medical records were reviewed and those in which a recommendation for destructive eye surgery was recorded were included, irrespective of whether or not the surgery was done. Data collected included age, sex, profession, residence, the eye affected, visual acuity, the use of conservative therapy, indication for surgery, and the type of surgical procedure done in those who underwent surgery. Data analysis was done using Epi Info 2004 and Microsoft Office Excel 2007.
Results
Over the 9-year study period, a total of 29,685 new patients were consulted. Destructive eye surgery was recommended in 48 patients, giving a prevalence of 1.62 per 1000. Among these 18 were females (37.5%) and 30 were males (62.5%), giving a sex ratio of 1.67.
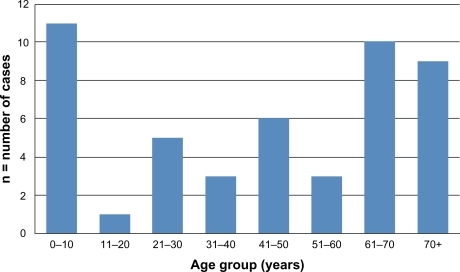
Mean age was 43.78 years (SD = 28.11, range 1 month to 91 years). Children aged 0 to 10 years comprised 23.1% (n = 11), including 7 cases aged <5 years (14.7%), and elderly patients (above 60 years) comprised 39.9% (n = 19) ().
Figure 1 Age distribution.
Retired workers comprised 23.4% (n = 11) of patients and city dwellers 72.9% (n = 35). All indications were monocular and where eyes were considered blind. Excluding 7 cases in which visual acuity could not be evaluated because of age, 82.9% (n = 34) had nil perception of light, 7.3% (n = 3) had light perception, and 9.8% (n = 4) saw hand movements. The right and left eyes were affected in equal proportions.
The most common condition for which a destructive surgery was recommended was endophthalmitis/panophthalmitis (n = 23, 47.9%) followed by neoplasm (n = 10, 20.8%) and absolute glaucoma (n = 7, 14.6%) ().
Table 1 Indications for destructive eye surgery
Late presentation was common with 57.1% presenting at least 2 weeks after the onset of symptoms. Conservative therapy was attempted in 60.4% (n = 29) of cases, mostly in those with endophthalmitis/panophthalmitis and those with absolute glaucoma. Broad spectrum topical and oral antibiotics such as ciprofloxacin and fucidic acid were used in cases with endophthalmitis/panophthalmitis; surgery was proposed only when there was no improvement. Topical or systemic antiglaucoma drugs and retro-bulbar injection of absolute alcohol were used as first- and second-line therapies, respectively, to control pain in absolute glaucoma. Surgery was indicated only after these failed. Surgery was recommended as the first-line therapy in 39.6% of cases (n = 19). This involved all cases with post-traumatic rupture of the globe and those with advanced neoplasm.
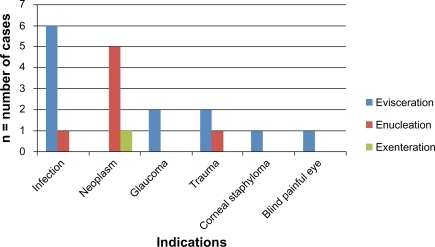
Acceptance rate for surgery was 41.7%. Surgery was done in 20 cases, with evisceration representing 50% of the procedures (n = 10) (). The lone case of exenteration was done following recurrence of retinoblastoma after earlier enucleation. There was no implant placement, and orbital infection occurred in 15.8% (n = 3) of cases in the postoperative period. Postsurgical infection was managed with the use of systemic antibiotics (cloxacillin and ciprofloxacin). In 2 cases, it was controlled within 10 days, but persistence in 1 case prompted sample collection for culture, which revealed a methicillin-sensitive Staphylococcus aureus. Oral antibiotics were continued, daily cleansing and dressing with the use of topical tetracycline was done, and the infection resolved within 3 weeks.
Figure 2 Types of surgery done, and their indications and frequencies.
Histopathology was not routinely requested, but was requested in cases with suspected neoplasm. There was histological confirmation of all cases of retinoblastoma who underwent surgery (n = 5). One case of squamous cell carcinoma in an adult was confirmed by histology. Average length of follow-up of these cases was 4 months and recurrence occurred in 40% (n = 2). Cases of recurrence were referred to the radiation oncology unit for external beam radiotherapy.
Discussion
The mean age of our patients (43.78 years, SD = 28.11) is higher than previously reported in other African series on destructive eye surgeries. Means ranging from 36.4 to 37 years have been reported.Citation1,Citation8,Citation9 The most affected age group was that of 0 to 10 years. A similar finding has been reported in China.Citation10 In Madagascar and Uganda, the most affected age groups in studies on enucleations were that of 21 to 30 and 30 to 39 years respectively.Citation11,Citation12 The age group of 50 to 59 years was the most represented in a series from Jerusalem.Citation13 The elderly comprised 39.9% in this study, but only 12% in the Madagascar series,Citation11 probably due to the fact that trauma was the first cause of enucleation in this Madagascan study. Severe ocular injuries peak in the young as they are in the most active period of their lives and stand greater chances of injury at work or at home.Citation10
The most common cause for recommending a destructive eye surgery in our study was endophthalmitis/panophthalmitis, followed by neoplasm and absolute glaucoma. Epee et al in their study on 32 cases of ocular mutilating surgery in Yaoundé, as well as Gyasi et al in a series of 337 eyes, reported the leading roles of infection and trauma.Citation8,Citation9 Trauma and malignancy were the leading causes of 143 enucleations in Zaire,Citation14 while trauma and corneal diseases were the leading causes in Uganda and Ethiopia.Citation12,Citation15 The high prevalence of severe intraocular infections leading to indications for eye removal could be related to the practice of self-medication among city dwellers and the use of traditional eye medicine by the rural population. Self-medication with over-the-counter eye drops, possibly containing steroids, contributes to worsening infections with poorer outcomes.Citation1,Citation16 The use of traditional eye medicine by peasant farmers has also been reported to influence the incidence of infection-related destructive procedures.Citation16 All our cases of intraocular infections were secondary to trauma; there was no cause of postoperative endophthalmitis requiring eye removal.
The high incidence of neoplasm is related to the large number of children in the study presenting with retinoblastoma. Out of 10 cases of neoplasm, 9 were cases of retinoblastoma occurring in children aged ≤5 years. They all presented at stage 4 or 5 (Reese-Ellsworth classification) when local ophthalmic therapies such as cryotherapy, laser photocoagulation, thermotherapy, or plaque radiotherapy can no longer be of first choice. Enucleation is the therapy of choice in such cases.Citation5 The interval between the onset of symptoms and consultation in our cases ranged from 1 month to 5 years. In a study on enucleations in China, the interval between the onset of symptoms and enucleation in cases with retinoblastoma ranged from 1 day to 3 years.Citation10 Intra-arterial chemotherapy or intravenous chemoreduction are indicated before enucleation and external beam radiotherapy is reserved for the last alternative therapy because of its side effects.Citation6
Penetrating ocular injuries with rupture of the globe accounted for 8.3% (n = 4), including a case of gunshot injury during amateur hunting. Gunshot and other violence-related injuries have been reported to be more frequent in times of war.Citation17
The 41.7% rate of acceptance of destructive eye surgeries in this study is indicative of the fact that the possibility of blindness is frightful and the removal even of a blind eye is a devastating experience for the patient. Patients undergoing eye removal need understanding, support and reassurance to help cope with the psychological effects. The attitude of health workers, family, peers, or co-workers is important. Evisceration was the most performed procedure, similar to findings in other studies.Citation1,Citation8,Citation16 The controversy over enucleation versus evisceration still exists. Intraocular tumor is an absolute contraindication for evisceration and should always be ruled out before evisceration is recommended.Citation4 Fundus examination or B-ultrasonography when the media is opaque should be done to rule out intraocular tumors such as uveal melanoma, which can recur following evisceration.Citation18,Citation19 The choice of the procedure elsewhere depends on the surgeon and the patient. It is generally accepted that motility and cosmetic appearance are better after evisceration and patients usually agree to this.Citation4 Since the eye is an integral part of facial beauty, giving the patient the most normal appearance after such a psychologically and socially devastating surgery cannot be overemphasized. Orbital reconstruction surgery is unfortunately not practised in our setting due to the lack of training in this domain.
Conclusion
The most common indication for destructive eye surgery in our setting is endophthalmitis/panophthalmitis. Most patients refuse surgery probably due to its likely psychological impact. Educating the population on the dangers of late presentation and the need to avoid self-medication can help reduce the need for destructive eye surgeries. Screening programs should also be created and implemented to detect retinoblastoma early in order to avoid the need for enucleation. Technology and training in cyclodestructive procedures such as cyclophotocoagulation and cyclocryotherapy should be offered; this will help reduce the need for enucleations in absolute glaucoma. Ophthalmologists should also be trained in oculoplastics in order to manage cases of orbital reconstruction following eye removal; this will go a long way to reduce the psychosocial burden involved in losing an eye.
Disclosure
The authors declare no conflicts of interest.
References
- EtebuENAdioAOIndications for removal of the eye at a tertiary hospital in south-southern NigeriaEast Afr J Ophthalmol20081922
- MoshfeghiDMMoshfeghiAAFingerPTEnucleationSurv Ophthalmol200044427730110667436
- Shah-DesaiSDTyersAGMannersRMPainful blind eye: efficacy of enucleation and evisceration in resolving ocular painBr J Ophthalmol200084443743810729307
- MiglioriMEEnucleation versus eviscerationCurr Opin Ophthalmol200213529830212218460
- De PotterPCurrent treatment of retinoblastomaCurr Opin Ophthalmol200213533133612218465
- ShieldsCLShieldsJABasic understanding of current classification and management of retinoblastomaCurr Opin Ophthalmol200617322823416794434
- ShapiroAMonseliseMBDestructive ophthalmic procedures, a comparison between a developed and a developing countryAlbrecht Von Graefes Arch Klin Exp Ophthalmol19782074271273311595
- EpeeEMoukouriNEKamegniGOcular mutilating surgery: a case study of 32 patients operated at the university teaching hospitalRev Afr Chir Spec20080020032328
- GyasiMEAmoakuWMAdjuikMCauses and incidence of destructive eye procedures in north-eastern ghanaGhana Med J200943312212620126324
- ChengGYLiBLiLQGaoRRenJXuXLReview of 1375 enucleations in the TongRen Eye Centre, BeijingEye200822111404140917603465
- RaskindrahonaEAndriantsoaVVohanginirinaREtiologies des énucleations: a propos de 83 casMédecine d’Afrique Noire1999462103105
- DavangerMCauses of enucleation in UgandaBr J Ophthalmol197054425255448526
- BattenKLCauses of enucleation as seen in JerusalemBr J Ophthalmol197155317417665575218
- KaimboKCauses of enucleation in ZaireJ Fr Ophtalmol198811106776803243952
- HaileMAlemayehuWCauses of removal of the eye in EthiopiaEast Afr Med J199572117357388904067
- NwosuSNDestructive ophthalmic surgical procedures in Onitsha, NigeriaNiger Postgrad Med J2005121535615827599
- ThachABJohnsonAJCarrollRBSevere eye injuries in the war in Iraq, 2003–2005Ophthalmology2008115237738217904224
- EagleRCJrGrossniklausHESyedNHoganRNLloydWC3rdFolbergRInadvertent evisceration of eyes containing uveal melanomaArch Ophthalmol2009127214114519204229
- LevineRAPuttermanAMKoreyMSRecurrent orbital malignant melanoma after the evisceration of an unsuspected choroidal melanomaAm J Ophthalmol19808945715747369322