Abstract
Purpose:
To present the functional and anatomic changes after intravitreal bevacizumab in eyes with macular edema (ME) due to branch retinal vein occlusion (BRVO).
Design:
The study was a retrospective study.
Materials and methods:
The study included 31 patients with ME due to BRVO. We compared the examination findings of patients with ME before and after intravitreal bevacizumab therapy at 12 months. The study included patients who had macular edema secondary to BRVO treated with bevacizumab. The therapy was started in the first week after occlusion. The initial therapy was three intravitreal bevacizumab injections at monthly intervals with 1.25/0.05 mL bevacizumab. Patients with a baseline visual acuity less than 0.5 (logarithm of the minimum angle of resolution [logMAR] 0.30), central macular thickness (CMT) more than 290 μm, and no neovascularization were included. Patients with diabetes mellitus or a history of intravitreal triamcinolone or grid laser photocoagulation therapy or ischemic BRVO were excluded. The retreatment criteria were as follows: increased CMT more than 100 μm combined with a loss of visual acuity of five or more letters. The statistical analysis of this study was carried out by paired samples t-test (SPSS). A P value of less than 0.05 was considered to be statistically significant.
Results:
This retrospective study included 33 eyes of 31 patients (20 women, 11 men; mean age was 55.30 ± 9.62 years (range 36–75 years). Patients received a mean of 5.3 injections during 12 months of follow-up. The best corrected visual acuity increased from 0.66 ± 0.20 (logMAR) at baseline to 0.22 ± 0.13 (logMAR) (t = 15.42; P < 0.001) at month 12. The CMT decreased from 494.15 ± 104.16 μm at baseline to 261.79 ± 45.36 μm at month 12 (− 232.36 ± 109.98 μm); P < 0.001). No bevacizumab-related systemic or ocular adverse effects following intravitreal drug injections were observed. The majority of patients required reinjection(s) treatment for ME (84.9%).
Conclusion:
Intravitreal therapy using bevacizumab appears to be an effective primary treatment option for ME due to BRVO. No serious ophthalmologic or systemic side effects were observed for intravitreal bevacizumab therapy. The main disadvantage of bevacizumab therapy is the requirement of multiple injections in order to maintain visual and anatomic improvements.
Introduction
Retinal vein occlusion (RVO) is the most common retinal vascular disease after diabetic retinopathy. Although the pathogenesis is still not fully clear, several risk factors have been associated with RVO, including age, diabetes mellitus, atherosclerotic retinal vessel changes, hypertension, and open-angle glaucoma.Citation1–Citation4
The most common sequela of branch retinal vein occlusion (BRVO) is the development of cystoid macular edema (ME) with a consecutive deterioration in vision. The major stimulus for the formation of ME and neovascularization in patients with RVO seems to be hypoxia-induced production of vascular endothelial growth factor (VEGF), an angiogenic factor that promotes angiogenesis and increases vascular permeability.Citation5
The only proven treatment method for eyes with ME secondary to BRVO is macular grid laser photocoagulation. However, according to the Branch Vein Occlusion Study (BVOS), only patients with ME associated with BRVO and a visual acuity of 20/40 or less showed a significant visual benefit compared with the untreated control group.Citation6
An alternative therapy for patients with ME secondary to BRVO is intravitreal anti-VEGF injection. The first report of the efficacy of intravitreal bevacizumab (a recombinant monoclonal antibbody binding to all isoforms of VEGF) in a patient with ME secondary to BRVO was in 2005.Citation7
Several studies have evaluated the efficacy of intravitreal triamcinolone in the treatment of ME secondary to BRVO, but were only able to show stabilization or a moderate improvement in visual acuity.Citation8–Citation10 However, the main limitation of intravitreal triamcinolone therapy is the high rate of side effects, such as cataract formation or increased intraocular pressure. No complications or serious side effects were observed in recent studies of bevacizumab therapy.Citation11–Citation14
Several retrospective and prospective studies have shown the benefit of anti-VEGF treatment, with an improvement in visual acuity and a decrease of retinal thickness in patients with ME associated with RVO.Citation11–Citation13,Citation15–Citation22
We have designed a retrospective clinical study to present the effect of intravitreal bevacizumab therapy in patients with ME secondary to BRVO at 12 months.
We reviewed data of patients who had ME secondary to BRVO who were treated with bevacizumab (Avastin 1.25 mg/0.05 mL) and followed up with regular visits (every month) during at least 12 months.
Materials and methods
The study included 31 patients with ME secondary to BRVO. The inclusion criteria were: ME secondary to BRVO, initial therapy started in the first week with Avastin, a baseline visual acuity below 0.5 (logarithm of the minimum angle of resolution [logMAR] 0.3), central macular thickness (CMT) more than 290 μm, and no neovascularization. Patients with diabetes mellitus, a history of intravitreal triamcinolone injection(s) or grid laser photocoagulation therapy, or ischemic BRVO were excluded from this study. All eyes had a complete ophthalmologic evaluation at baseline, day 1, day 7, month 1, and at monthly intervals during follow-up. Examinations included best corrected visual acuity (BCVA); testing using Early Treatment Diabetic Retinopathy Study (ETDRS) charts at 4 meters in the logMAR values; slit-lamp and fundus examination, including tonometry; standardized optical cohorence tomography imaging (OCT) (Optovue, Inc Freemont, CA); and color fundus photography. Fluorescein angiography was performed at baseline and at 12 months to identify the presence of BRVO, active extravasation, and the extent of retinal nonperfusion.
All patients received three initial Avastin (bevacizumab 1.25 mg/0.05 mL) injections at monthly intervals. Patients were examined monthly after three injections. The retreatment was performed when there was an increase in 1 mm CMT as measured by OCT macular mapping of at least 100 μm with/without a vision loss for at least five ETDRS letters.
All intravitreal injections were performed in the operating room under sterile conditions. Bevacizumab was filled and packed under sterile conditions by the institutional pharmacy, using tuberculine syringes containing a total volume 1.25 mg/0.05 mL. Avastin was injected into vitreous body via pars plana using a 27 G needle at inferior temporal area at 3.5 mm distance from limbus. The visual acuity and mean CMT are expressed as mean ± standard deviation. The data at baseline and after injections at 12 months were evaluated statistically. The statistical analysis of this study was carried out by the paired samples t-test (SPSS; SPSS, Inc., Chicago, IL). A P value of less than 0.05 was considered to be statistically significant.
Results
This retrospective study included 33 eyes of 31 patients (20 women, 11 men; mean age was 55.30 ± 9.62 years (range 36–75 years). The frequency of bevacizumab injections into vitreous body is presented in .
Table 1 Distribution of number of reinjections
The mean BCVA was 0.66 ± 0.20 LogMAR at baseline and improved to 0.22 ± 0.13 LogMAR at 12 weeks; the mean 1 mm CMT was 494.15 ± 104.16 μm (range 343–771).
After 12 months of follow-up, the mean logMAR values of BCVA had increased significantly to 0.66 ± 0.20 (t = 15.42; P < 0.001), whereas mean CMT had decreased to 261.79 ± 45.36 μm (− 232.36 ± 109.98 μm; P < 0.001) ().
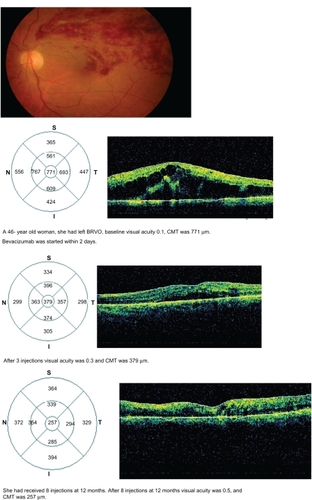
Figure 1 The result of bevacizumab therapy in a patient with macular edema secondary to branch retinal vein occlusion (BRVO). A 46-year-old woman had left BRVO, baseline visual acuity of 0.1, and central macular thickness (CMT) of 771 μm. Bevacizumab was started within 2 days. After three injections, visual acuity was 0.3 and CMT was 379. She had received eight injections at 12 months. After eight injections at 12 months, her visual acuity was 0.5 and CMT was 257 μm.
No major ophthalmologic (retinal detachment, ocular hypertension, glaucoma, uveitis, endopthalmitis, retinal artery occlusion) or systemic (thromboembolic events, systemic hypertension, myocardial infarction) side effects occurred. Neovascularization of the retina, optic disc, or iris have not been recorded.
Discussion
In this study we compared data of baseline values and after therapy with bevacizumab (injections 3–8) at 12 months. The results of this retrospective study showed that intravitreal bevacizumab treatment in patients with ME secondary to BRVO was associated with a significant improvement in visual acuity (from 0.66 ± 0.20 to 0.22 ± 0.13 logMAR) and with a marked decrease in CMT (− 232.36 ± 109.98 μm; P < 0.001) at 12 months.
During 12 months of follow-up, no severe ocular adverse effects, such as endophthalmitis, retinal detachment, traumatic cataract, ocular hypertension, glaucoma, uveitis, and central retinal artery occlusion, were observed.
We did not encounter any serious side effects related to bevacizumab. However, serious side effects of bevacizumab have been reported.Citation15–Citation17,Citation23
A recent study showed that the results of therapy with bevacizumab were better than those with grid laser therapy in ME secondary to BRVO.Citation24,Citation25 However, cataract, ocular hypertension, and glaucoma are frequently encountered with triamcinolone therapy.Citation26–Citation29 We did not observe cataract or glaucoma in our study.
A decrease in CMT as seen by OCT and a reduction in the area of leakage with fluorescein angiography were observed. Avascular areas were stable and they did not progress after treatment with Avastin.
Although nearly all patients showed an important response to intravitreal Avastin treatment with an increase in visual acuity and a reduction in CMT initial therapy, the ME had not resolved completely in 84.9% of all patients after three injections. The majority of patients required retreatment for ME.
The main disadvantage of Avastin is short duration of the therapeutic effect and the requirement of reinjections.Citation11,Citation19,Citation21,Citation22 We did not measure anti-VEGF levels, but some studies also showed a close correlation between aqueous VEGF levels and the severity of ME in patients with RVO.Citation30,Citation31
Finally, intravitreal bevacizumab therapy appears to be an effective and safe treatment option for ME secondary to BRVO. The main disadvantage is the requirement for multiple injections in order to maintain good visual acuity and macular thickness.
Disclosure
The authors involved in this study have no proprietary or material conflicts of interest to declare in relation to this work.
References
- CugatiSWangJJRochtchineEMitchellPTen-year incidence of retinal vein occlusion in an older population: the Blue Mountain Eye studyArch Ophthalmol200612472673216682596
- HayrehSSZimmermanBMc CarthyMJPodhajskyPSystemic diseases associated with various types of retinal occlusionAm J Ophthalmol2001131617711162981
- BlondJGlacet-BernardABayaniNRetinal vein occlusion and hyperhomocysteinemiaJ Fr Opthalmol200326249253
- RathEZFrankRNShinDHKimCRisk factors for retinal vein occlusion. A case-control studyOphthalmology1992995095141584567
- AielloLPAveryRLArrigPGVascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disordersN Engl J Med1994331148014877526212
- Branch Retinal Vein Occlusion Study GroupArgon laser photocoagulation for macular edema in branch vein occlusionAm J Ophthalmol1984982712826383055
- RosenfeldPJFungAEPuliafitoCAOptical cohorence tomography findings after an intravitreal injection of bevacizumab (Avastin) for macular edema from central vein occlusionOphthalmic Surg Lasers Imaging20053633633916156153
- AvitabileTLongoAReibaldiAIntravitreal triamcinolone compared with macular grid photocoagulation for the treatment of cystoid macular edemaAm J Ophthalmol200514069570216226521
- KaracorluMKaracorluSAOzdemirHIntravitreal triamcinolone acetonide for treatment of serous macular detachment in central vein occlusionRetina2007271026103018040239
- GregoriNZRosenfeldPJPuliafitoCAOne-year safety and efficacy of intravitreal triamcinolone acetonide for the managment of macular edema secondary to central vein occlusionRetina20062688989517031288
- PragerFMichelsSKriechbaumKIntravitreal bevacizumab (Avastin) for macular oedema secondary to retinal vein occlusion: 12-month results of prospective clinical trialBr J Ophthalmol20099345245619074916
- AhmadiAAChuoJYBanashkevichAThe effects of intravitreal bevacizumab on patients with macular edema secondary to branch retinal vein occlusionCan J Ophthalmol20094415415919491948
- KimJYParkSPComparison between intravitreal bevacizumab and triamcinolone for macular edema secondary to branch retinal vein occlusionKorean J Ophthalmol20092325926520046685
- HouJTaoYJiangYRIntravitreal bevacizumab versus triamcinolone acetonide for macular edema due to branch retinal vein occlusion: a matched studyChin Med J (Eng)200912226952699
- IturradleCBSpaideRFMeyerleCBIntravitreal bevacizumab (Avastin) treatment of macular edema in central retinal vein occlusion: a short-term studyRetina20062627928416508427
- HsuJKaiserRSSivalingamAIntravitreal bevacizuma (Avastin) in central vein occlusionRetina2007271013101918040237
- RabenaMDPieramiciDJCastellarinAAIntravitreal bevacizumab (Avastin) in the treatment of macular edema secondary to branch retinal vein occlusionRetina20072741942517420692
- AbeggMTappeinerCWolf-SchnurrbushUTreatment of branch retinal vein occlusion induced macular edema with bevacizumabBMC Ophthalmol200881818823536
- FigueroaMSContrerasINovalSArruabarrenaCResults of bevacizumab as the primary treatment for retinal vein occlusionsBr J Ophthalmol2010941052105620679089
- GuthoffRMeigenTHennemannKSchraderWComparison of bevacizumab and triamcinolone for treatment of macular edema secondary to branch retinal vein occlusion in pair-matched analysisOphthalmologica201022431932420424494
- WuLArevaloJFBerrocaiMHComparison of two doses intravitreal bevacizumab as primary treatment for macular edema secondary to branch retinal vein occlusions: results of the Pan American Collaborative Retina Study Group at 24 monthsRetina2009291396140319898177
- AchTHoehAESchaalKBLong-term follow-up of OCT-guided bevacizumab treatment of macular edema due to retinal vein occlusionGraefes Arch Clin Exp Ophthalmol20092471635164119633982
- FungAERosenfeldPJReichelEThe International Intravitreal Bevacizumab Safety Survey: using the internet to assess drug safety worldwideBr J Ophthalmol2006901344134916854824
- RussoVBaroneAConteEBevacizumab compared with macular laser grid photocoagulation for cystiod macular edema in branch retinal vein occlusionRetina2010301324132520827152
- CekicOCakırMYazıcıATA comparison of three different intravitreal treatment modalities of macular edema due to branch retinal vein occlusionCurr Eye Res20103592592920858114
- RezendeMPDiasAFOshimaAStudy of visual acuity and intraocular pressure in the treatment of macular diabetic edema with intravitreous triamcinoloneArq Bras Oftalmol20107312913420549040
- Vasconcelos-SantosDVNehemyPGSchachatAPNehemyMBSecondary ocular hypertension after intravitreal injection of 4 mg of triamcinolone acetonide: incidence and risk factorsRetina20082857358018398360
- GilliesMCIslamFMLarssonJTriamcinolone-induced cataract in eyes with diabetic macular oedema: 3-year prospective date from a randomised clinical trialClin Experiment Ophthalmol20103860561220528977
- IslamMSVernonSANegiAIntravitreal triamcinolone will cause posterior subcapsular cataract in most eyes with diabetic maculopathy within 2 yearsEye (Lond)20072132132316543927
- NomaHFunatsuHYamasakiAqueous humour of cytocines are correlated to vitreous levels and severity of macular oedema in branch retinal vein occlusionEye (Lond)200822424816826241
- NomaHMinamotoAFunatsuHIntravitreal levels of vascular endothelial growth factor and interleukin-6 are correlated with macular edema in branch retinal vein occlusionGraefes Arch Exp Ophthalmol2006244309315