Abstract
Purpose:
To investigate the role of postoperative topical 0.05% cyclosporine A (CsA) eye drops (Restasis®, Allergan Pharmaceutical) in the prevention of recurrence among patients with primary pterygium treated with bare-sclera technique.
Methods:
In this prospective randomized controlled study, 36 eyes (34 patients) with primary pterygium were randomized into two groups: Group I comprised 18 eyes (18 patients), and Group II comprised 18 eyes (16 patients). Bare sclera technique was performed in both groups. In Group I, 0.05% CsA was administered postoperatively at 6-hour intervals for 6 months, and Group II did not receive any cyclosporine treatment. The patients were assessed for recurrence, side effects, and complications at postoperative 1 and 7 days as well as each month during the following year. Conjunctival advances which showed a limbus higher than 1 mm were recognized as recurrence.
Results:
Recurrence occurred in four patients (22.2%) in Group I and in eight (44.4%) patients in Group II.
Conclusion:
Postoperative application of low-dose CsA can be effective for preventing recurrences after primary pterygium surgery.
Introduction
Pterygium is a common ocular surface disease characterized by tissue remodeling, cellular proliferation, neovascularization, and inflammation.Citation1,Citation2 A stromal overgrowth of fibroblast and blood vessels are accompanied by an inflammatory cell infiltrate and abnormal extracellular matrix accumulation.Citation3–Citation6 Although several hypotheses have been associated with its etiology, its pathology still remains to be explained. Secretion of proinflammatory cytokines such as interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor (TNF)-α secondary to chronic ultraviolet (UV) radiation, is a widely recognized etiological factor in pathogenesis of this lesion.Citation6,Citation7 These cytokines can stimulate proliferation of cultured Tenon’s capsule fibroblasts and induce expression of matrix metalloproteinases in cultured pterygium; specifically, IL-1 plays an important role in the development process of pterygium.Citation6,Citation7
The vascular endothelial growth factor (VEGF) family, which is known to have a role in angiogenesis, has been shown to exhibit an increase in pterygium epithelium and vascular endothelium.Citation8–Citation13 VEGF is believed to be stimulated by a mediation of TNF-α through UVB (ultraviolet B) induction.Citation14
Cyclosporine A (CsA) shows a selective effect against T-helper cells and prevents the synthesis and secretion of ILs.Citation16 CsA has also been shown to block angiogenic factors induced by VEGF.Citation15–Citation17 Based on these studies, we thought CsA might have an effective role on treatment of pterygium.
The aim of this study was to investigate the influence of postoperative topical CsA use on recurrence.
Method
This study was a prospective randomized controlled study on 36 consecutive eyes of primary pterygium. Written informed consent was obtained from all the patients. All pterygia were located nasally. Ocular diseases and surgical history of the patients are shown in . The patients were randomized into two groups: 18 eyes of 18 patients were included in Group I, and 18 eyes of 16 patients were included in Group II. Female/male ratio was the same in both groups (nine female, nine male).
Table 1 Ocular diseases and surgical history of the patients
The inclusion criteria were:
Diagnosis of primary pterygium
Pterygium size ≥2 mm (the horizontal length of the tissue from limbus to cornea was measured by slit lamp biomicroscopy)
Ocular discomfort refractory to medical treatment
Visual loss induced by pterygium.
Patients who had a recurrent pterygium or allergy to topical CsA, and those who were pregnant, were excluded from the study.
Bare sclera method was performed in both groups. Surgical procedures were performed under local anesthesia using an operation microscope. The pterygium head was taken off the cornea by blunt dissection with a crescent knife. The body of pterygium was dissected and excised with Westcott scissors. Minimal cautery was used to maintain hemostasis. The conjunctiva was closed together with a size 8/0 vicryl suture, leaving a 4-mm bare sclera. The eyes were closed with a rondel after the application of antibiotic ointment. In all of the patients, antibiotic drops were given for 15 days and steroid drops were given for 1 month. In Group I, 0.05% CsA (Restasis®, Allergan Pharmaceutical) was administered postoperatively at 6-hour intervals for 6 months. In Group II, patients did not receive CsA. All patients were followed up at postoperative 1 day, 7 days, and then every month. Minimum duration of the follow-up periods was 12 months. In each follow-up, patients were assessed for recurrence and postoperative complications such as persistent corneal defect, infection, scleral melting, and drop intolerance. The recurrence was defined as fibrovascular tissue invading the cornea ≥1 mm).Citation17,Citation18
Statistical analyses
NCSS (Number Cruncher Statistical System) 2007 and PASS (Power Analysis and Sample Size) 2008 statistical software (NCSS, Kaysville, UT) was used for the statistical analyses. The study data were expressed by definitive statistics (mean, standard deviation, median). Quantitative data were compared by independent samples t-test and Mann–Whitney U test. The relationship between the pterygium size and the recurrence time was evaluated by Spearman’s rank correlation analysis. Recurrence-free survival time was evaluated by Kaplan–Meier survival analysis. Categorical data were evaluated by Chi-square test. P < 0.05 was recognized as statistically significant.
Results
Our study was performed on 36 eyes in total (18 eyes in Group I and 18 eyes in Group II). None of the groups demonstrated scleral thinning, necrosis, or any other visually significant complication. The CsA group (Group I) showed no adverse reaction other than a mild burning sensation and irritation at the time of the application. There was no statistically significant difference between the groups with regard to age (P > 0.05). Mean age was 57.05 ± 11.65 in Group I and 53.27 ± 10.88 in Group II. No statistically significant difference was determined between the groups in terms of pterygium size (P > 0.05). Mean pterygium size was 3.00 ± 0.57 mm in Group I and 2.73 ± 0.61 mm in Group II. We observed no statistically significant difference between the recurrence times of the groups (P > 0.05). Mean recurrence time was 2.62 ± 0.95 months in Group I and 1.87 ± 0.83 months in Group II. There was no statistically significant difference between the groups relative to gender distribution (P > 0.05). Although recurrence rate was higher in Group II than in Group I, the difference was not statistically significant (P > 0.05) . No statistically significant difference was determined between the cases with and without recurrence in terms of pterygium size (P > 0.05) .
Table 2 Evaluations relative to the groups
Table 3 Evaluation of the pterygium sizes relative to recurrence rates
In view of all cases with recurrence, although pterygium size and recurrence time showed a considerable positive correlation, it was not statistically significant (r = 0.343; P > 0.05) . In Group I, pterygium size and recurrence displayed a negative correlation in four cases with recurrence; however, due to the low number of cases, it was not found to be statistically significant (P > 0.05). In Group II, pterygium size and recurrence showed a significant positive correlation (68.4%) in eight cases with recurrence (pterygium size elevated parallel to the increases in recurrence time).
Table 4 The relationship between the pterygium size and the recurrence time
In Group I, while four cases exhibited recurrence , 14 (77.8%) did not show recurrence, and the mean recurrence-free follow-up time was 9.92 ± 0.92 months. In Group II, while eight cases exhibited recurrence, 10 (55.6%) cases did not show recurrence, and the mean recurrence-free follow-up time was 7.50 ± 1.19 months . Recurrence-free survival rates were evaluated by logrank test and no statistically significant difference was determined between the 12-month survival rates (P = 0.130, P > 0.05) .
Figure 1 The relationship between pterygium size and recurrence time in Group II.
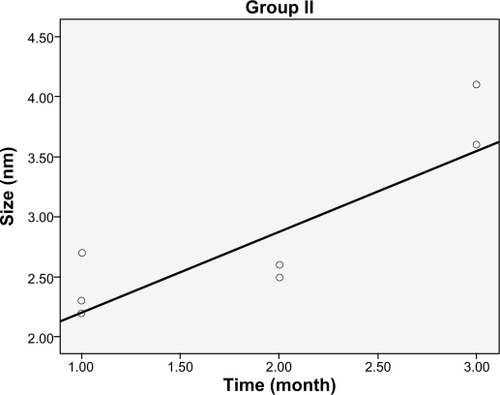
Figure 2 Distribution of the recurrence-free follow-up times.
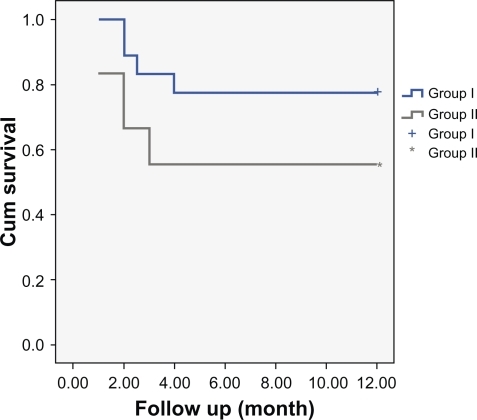
Table 5 Survival rate during recurrence-free follow-up time
Discussion
Previously, pterygium was recognized as a degenerative condition; recently, as a result of the latest studies, it is thought to be a growth disorder, and mainly proliferative factors are investigated for revealing the true etiopathogenesis.Citation5,Citation17 Therefore, surgical treatments aim to replace limbal stem cells, whereas adjuvant therapies target preventing proliferation and angiogenesis. Despite those studies, a definitive treatment method which shows no recurrence, along with the least degree of complications, has yet to be found. The most widely recognized proposal for pathogenesis is that UV increases release of certain multifactorial cytokines, IL-6 and IL-8, from pterygium epithelium, which leads to the initialization of neovascularization and chronic inflammation.Citation5–Citation7 IL-6 has been shown to increase angiogenesis via VEGF induction.Citation19 Despite considerable contribution of UV and environmental factors, occurrence of pterygium is varied in people living in the same environment. Hypersensitivity is a powerful factor in pathogenesis, and the amount of immunoglobulin E (IgE) has been found to exhibit an elevated level in pterygium tissue.Citation19 IgE rise leads to release of cytokines, causing thrombocyte aggregation, which causes release of growth factors leading to epithelium proliferation. Although previous studies demonstrate that T lymphocytes are rarely identified in conjunctiva, they are found to be in elevated levels in pterygium tissue.Citation19 All those data show the importance of T-lymphocyte-mediated strong cellular immunity in pterygium pathogenesis. CsA selectively suppresses functions of T-helper lymphocytes and production of both inflammatory cytokines and inflammatory mediators.Citation20,Citation21 In animal studies, it has been shown to suppress IgE production in a T-cell-dependent manner and inhibit histamine release from basophil and mast cells.Citation21 In vivo and in vitro studies have showed that CsA inhibits angiogenesis triggered by VEGF. We believed that inhibiting all those paths with CsA, which are thought to have a role over pterygium pathogenesis, might be effective in preventing recurrence.Citation22 CsA 0.05% is found to be effective in inhibiting the proliferation in Tenon’s capsule fibroblasts.Citation23 In a study similar to ours, thiotepa and cyclosporine have been compared following pterygium surgery and CsA was found to be significantly more effective than thiotepa.Citation24
The recurrence rate was 44.4% for bare sclera technique and 22.2% for bare sclera technique + topical 0.05% CsA. None of our cases demonstrated a serious complication. Moreover, recurrence rate was observed to decrease. Our study group was comprised of glaucoma or diabetic retinopathy patients who had a history of vitreoretinal or glaucoma surgery in whom we could not perform a treatment with conjunctival or limbal autograft. Therefore, we were unable to deliver mitomycin and other adjuvant therapies and thus had the chance to evaluate efficacy of CsA in a surgical procedure associated with high recurrence rates. Because of this study design, we believe that our study obtained more reliable results on the effects of CsA over recurrence rates.
Similar studies have been performed by using conjunctival autografts. Tok et al used CsA following primary excision in primary pterygium cases, and the recurrence rate was determined to be 12.9%.Citation25 In a study by Aydin et al, CsA was found to be effective in reducing recurrence and preventing postoperative pain and complications.Citation26 However, Aydin et al used CsA after applying limbal conjunctival autograft and observed a recurrence rate of 3.4%. Ibáñez et al preferred to apply the combination of mitomycin + conjunctival autograft and determined a recurrence rate of 7.5%.Citation27 In our study, the recurrence rate was 22.2%.
While our study appears to be similar with that of Tok et al our recurrence rate is higher. We believe that by applying more effective surgical techniques, such as conjunctival autograft and limbal autograft, we could have obtained better results. Moreover, although a remarkable decrease was observed in the recurrence rate of the patient group, the results were not statistically significant due to the low number of cases. However, since it is known to be a safe method, it can be performed among patients with a history of major surgery or in candidates of such surgeries. In conclusion, we believe that more effective results can be achieved by using topical CsA at higher doses.
Disclosure
This study was performed at Umraniye Education and Research Hospital, Ophthalmology Clinic, Istanbul, Turkey. The study was not presented at any meeting. There was no public or private financial support. None of the authors has a financial or proprietary interest in a product, method, or material used in the study.
References
- CoroneoMTGirolamoNWakefieldDThe pathogenesis of pterygiaCurr Opin Ophthalmol19991028228810621537
- HillJCMaskeRPathogenesis of pterygiumEye198932182262695353
- CameronMEHistology of pterygium: an electron microscopic studyBr J Ophtalmol198367604608
- ChanCMLiuYPTanDTOcular surface changes in pterygiumCornea200221384211805505
- WangIJLaiWTLiouSWImpression cytology of pterygiumJ Ocular Pharmacol Therap200016519528
- Di GirilomaNChuiJCoreneoMTWakefieldDPathogenesis of pterygia: role of cytokines, growth factors, and matrix metalloproteinasesProg Retin Eye Res200423219528915094131
- GirolamaNDKumarRKCorneaMTWakefieldDUVB. Mediated indication of interleukin-6 and 8 in pterigia and cultured human pterigium epithelial cellsInves Opthalmol Vis Sci200214311934303437
- DushkuNReidTWP53 expression in altered limbal basal cells of pingueculae, pterygia, and limbal tumorsCurr Eye Res19971612117911929426949
- TanDTTangWYLiuYPGohHSSmithDRApoptosis and apoptosis related gene expression in normal conjunctiva and pterygiumBr J Ophthalmol200084221221610655200
- WeinsteinORosenthalGZirkinHMonosTLifshitzTArgovSOverexpression of p53 tumor suppressor gene in pterygiaEye200216561962112194078
- LeeDHChoHJKimJTChoiJSJooCKExpression of vascular endothelial growth factor and inducible nitric oxide synthase in pterygiaCornea200120773874211588427
- MarcovichALMoradYSandbankJAngiogenesis in pterygium: morphometric and immunohistochemical studyCurr Eye Res2002251172212518239
- Van SettenGAspiotisMBlalockTDGrotendorstGSchultzGConnective tissue growth factor in pterygium: simultaneous presence with vascular endothelial growth factor – possible contributing factor to conjunctival scarringGrafes Arch Clin Exp Ophthalmol20032412135139
- YosihadaSOnoMShonoTInvolvement of interleukin-8, vascular endothelial growth factor, and basic fibroblast growth factor in tumor necrosis factor alpha-dependent angiogenesisMol Cell Biol1997177401540239199336
- PucciNNovembreECiaferoniAEfficacy and safety of cyclosporine eyedrops in vernal keratoconjunctivitisAnn Allergy Asthma Immunol200289329830312269651
- StrongBFarleyWSternMEPflugfelderSCTopical cyclosporine inhibits conjunctival epithelial apoptosis in experimental murine keratoconjunctivitis siccaCornea2005241808515604871
- Al FayezMFLimbal versus conjunctival autograft transplantation for advanced and recurrent pterygiumOphthalmology200210991752175512208727
- MutluFMSobaciGTatarTYildirimEA comparative study of recurrent pterygium surgery: limbal conjunctival autograft transplantation versus mitomycin C with conjunctival flapOphthalmology1999106481782110201608
- NakamuraMNishidaTDifferential effects of epidermal growth factor and interleukin 6 on corneal epithelial cells and vascular endothelial cellsCornea199918445245810422859
- SolomonASImmunologic basis for the pathogenesis of pterygiumAm J Optalmol198599216217
- NussenblattRBPalestineAGCyclosporine: immunology, pharmacology and therapeutic usesSurv Opthalmol198631159169
- OkudairaHSakuraiYTeradoKCyclosporin A-induced suppression of ongoing IgE antibody formation in the mouseInt Arch Allergy Appl Immunol1986791641813484729
- HerculesLAViveirosMMSchelliniSACadeiasJPadovaniCRExposure of Tenon’s capsule fibroblasts of pterygium to cyclosporin 0.05%Arg Bras Oftalmol200669831834
- WuHChenGCyclosporine A and thiotepa in prevention of postoperative recurrence of pterygiumYan Ke Xue Bao1999152919212579708
- Yalcin TokOBurcu NurozlerAErgunGAkbas KocaogluFDumanSTopical cyclosporine A in the prevention of pterygium recurrenceOphthalmologica2008222639139618765950
- AydinAKaradayiKAykanUCanGColakogluKBilgeAHEffectiveness of topical ciclosporin A treatment after excision of primary pterygium and limbal conjunctival autograftJ Fr Ophtalmol200831769970418971855
- IbáñezMEugarriosMFCalderónDITopical cyclosporin A and mitomycin C injection as adjunctive therapy for prevention of primary pterygium recurrenceOphthalmic Surg Lasers Imaging200940323924419485286