Abstract
Background:
The purpose of this study was to assess the repeatability and reproducibility of the PT100 noncontact tonometer and to compare its consistency with the Goldmann applanation tonometer (GAT) in measuring intraocular pressure (IOP).
Methods:
Triplicate IOP measurements were obtained on two separate occasions using the PT100 and GAT from randomly selected eyes in 66 healthy volunteers aged 22 ± 1 years. The repeatability and reproducibility of each techniques was assessed. Agreement between the techniques was statistically quantified using intrasession repeatability for each technique as the basis for comparison.
Results:
Both techniques returned equal IOP values in the first measurement session (15 ± 3 mmHg). The second session showed a mean difference in average IOP (1 ± 0.71). The 95% limits of agreement between the techniques were −5.2 to 5.5 mmHg and −4.0 to 4.7 mmHg (sessions 1 and 2, respectively). These mean differences were not statistically significant (P > 0.05, paired t-test), with the PT100 underestimating IOP measurement by 1.00 mmHg. The mean intrasession IOP for GAT sessions 1 and 2 was 0 ± 0.90 mmHg and 0.04 ± 1.06 mmHg, respectively, and the corresponding mean IOP measurement difference for the PT100 was −0.06 ± 0.96 and −0.39 ± 0.94 mmHg (sessions 1 and 2, respectively; P > 0.05, paired t-test). Repeatability coefficients for the GAT IOP measurements were 1.8 mmHg and 2.1 mmHg for sessions 1 and 2, while the PT100 repeatability coefficient was 1.9 mmHg and 1.8 mmHg for sessions 1 and 2, respectively. The intrasession repeatability coefficient of both techniques for test–retest differences were within ±5 mmHg.
Conclusion:
The PT100 noncontact tonometer produced greater repeatability than the GAT in assessment of IOP, whereas GAT resulted in more reproducible results. Both techniques showed a close level of agreement on comparison, with the PT100 underestimating IOP measurement by 1.0 mmHg only, although this was not clinically or statistically significant. Of importance is that the IOP measurements using these techniques could be interchangeable in the IOP range studied here.
Introduction
Intraocular pressure (IOP) measurement is a compulsory routine procedure in a complete eye care examination, and determination of IOP is essential in the evaluation of ocular health, because it is the main risk factor for developing glaucoma. The Advanced Glaucoma Intervention StudyCitation1 reported that decreasing the IOP in patients with glaucoma to <20 mmHg is beneficial, but noted it may not be enough to preserve the visual field, because some patients require a further decrease in IOP to <18 mmHg to avoid visual field damage. The Collaborative Initial Glaucoma Treatment StudyCitation2 found a significantly reduced loss of visual field if the IOP is kept to <18 mmHg,Citation2 affirming that a decrease in IOP delays visual field damage caused by glaucoma.
The Goldmann applanation tonometer (GAT) is currently the most widely used instrument for measuring IOP,Citation3 and is considered the “gold standard”.Citation4,Citation5 However, the GAT has two disadvantages. First, the instrument probe must come into direct contact with the cornea, which can increase the risk of infection. Second, use of the GAT requires a local anesthetic, and some patients, especially children, are unwilling or unable to tolerate drug instillation. With these factors in mind, several noncontact tonometers have been developed to facilitate measurement of IOP during vision screening.
Recently, several portable noncontact tonometers have been developed, ie, the TGDc-01 (Ryazan, Russia), the ICARE tonometer (TA01, Helsinki, Finland), the Tonopen (Mentor, Santa Barbara, CA), and the PT100 tonometer (Reichert Ophthalmics Inc, Depew, NY). The PT100 noncontact tonometer is a battery-operated hand-held portable tonometer weighing approximately 1.3 kg. Because of the key role of tonometry in glaucoma screening and the periodic need to assess IOP outside the clinic, these portable devices have found their usefulness in the heart of active ophthalmology and in optometry practices where nonmedical personnel take IOP measurements.
Several comparative studies have demonstrated the reliability and accuracy of IOP measurements obtained with noncontact tonometers (both desktop and portable) and their correlation with measurements obtained with the GAT in subjects with and without glaucoma.Citation3–Citation9 Only two studies have reported comparable IOP measurements with the PT100 noncontact tonometers and the GAT.Citation10,Citation11 The study by Salim et al was a comparative study of the PT100 and the GAT, but there was a large age variation among the recruited subjects, which may have affected the accuracy of the results. Murase et al focused on the effect of central corneal thickness on IOP measurements obtained by the PT100 and the GAT. However, neither the Salim nor the Murase study was able to verify the repeatability and reproducibility of IOP measurements in normotensive subjects obtained by the PT100 noncontact tonometer when compared with the “gold standard” of GAT. Therefore, the purpose of this study was to assess further the reliability, repeatability, and reproducibility of IOP measurements obtained with the PT100. We also verified the correlation of IOP measurements obtained by the PT100 and the GAT.
Subjects and methods
The study participants were 66 patients (46 men, 20 women) aged 20–25 (22 ± 1) years, who presented for routine oculovisual examinations at the King Saud University optometry clinics.
The study protocol was designed according to the principles of the Declaration of Helsinki and was approved by the ethics committee of the College of Applied Medical Sciences. After verbal instruction about the procedures involved in data collection, all subjects gave their informed consent to participate in this study.
IOP measurements were obtained only from one randomly selected eye of each subject. Randomization was carried out using random numbers generated on a Microsoft Excel spreadsheet. Exclusion criteria were a positive history of ocular disease, systemic disease with ocular implications, ocular surgery, total astigmatism which exceeded 3 D, or participation in a similar study carried out earlier at the same institution. A comprehensive ocular examination was carried out to screen each patient for eligibility. No subject was excluded from the study, but seven subjects were lost to follow-up.
For the assessment of IOP using the Reichert PT100 noncontact tonometer, measurements were made in triplicate and averaged to get the IOP reading for one eye. GAT measurements were made in triplicate and averaged to get the IOP for the selected eye. The period of corneal contact with the applanation probe was approximately five seconds (each time) to minimize simultaneously the effects of aqueous massage on repeated applanation readingsCitation11,Citation12 and the possible errors caused by oscillatory fluctuations in IOP, due mainly to the ocular pulse and respiratory cycles.Citation13–Citation16
Noncontact tonometry readings were always made before applanation with the GAT to eliminate the possible effect of ocular massage, which has been reported with the GAT but found to be absent with noncontact tonometers.Citation15–Citation19
Repeatability was assessed using all IOP measurements for each technique per subject. Reproducibility was assessed by a re-evaluation of each subject’s IOP during a second measurement session taken approximately one week later. The average IOPs for both sessions using one method were compared to assess the reproducibility of that method. The agreement between both techniques was statistically quantified using the repeatability (for each technique) as the basis for comparison.
The data for this study were masked so that the clinician (TA) who performed the GAT never knew the IOP of a subject before performing the procedure on him/her, and the IOP data records were maintained by another clinician, who also performed noncontact tonometry using the PT100 in the first session. In the second measurement session, these roles were switched. Each time a Goldmann IOP measurement was made, it was read off the scale by the second clinician, who then reset the scale to an arbitrary zero between 7 and 10 mmHg. This procedure was adopted to avoid any tactile clues which might aid the tonometrist to determine the endpoint of a reading.Citation3
All IOP measurements were made between 2 pm and 4 pm to ensure that the IOP, although still susceptible to diurnal fluctuations, was assessed at the time of the day when it is most stable.Citation20
Statistical analysis
IOP measured with PT100 versus GAT
The limits of agreementCitation23 between the PT100 and the GAT were assessed. To determine the presence or absence of a statistically significant difference between the IOP values returned by both methods, the average IOP using the PT100 was compared with the average IOP using the GAT for each subject at each measurement session. To ensure that each method was consistent and to measure the consistency of the PT100 noncontact tonometer against that of the GAT, the within-session differences for the noncontact tonometer in the first and second measurement sessions and the within-session differences for the GAT in both sessions were compared with each other in other columns (repeated-measures one-way analysis of variance).
Repeatability
Both tonometers were assessed for repeatability using all three readings for each subject to generate an average IOP and a mean difference. The column of the differences was plotted against the column of average IOPs to determine the limits of repeatability for each technique. Using the formula of Bland and Altman,Citation23 the repeatability coefficient (1.96*standard deviation [SD]within-session differences) was computed twice for each technique (once per session).
Reproducibility
The difference between the mean IOP in sessions 1 and 2 was determined for each subject, as was the average IOP between sessions. The column of differences was plotted against the column of averages to determine the limits of reproducibility for each technique. The reproducibility of the PT100 was compared with that for the GAT (paired t-test) to assess the reproducibility of IOP measured by the PT100. Using the formula of Bland and Altman,Citation23 the between-session reproducibility coefficient (1.96*SDbetween-session differences) was computed once for each technique. To determine if there was a significant variation in IOP for the subjects between the two measurement sessions, the average IOPs for each subject, measured by both methods, in session 1 were compared with the average IOP measured in session 2 (four columns) using repeated-measures one-way analysis of variance.
For each paired comparison of averages, a paired comparison was also performed for the corresponding within-subject standard deviations to determine if any potential difference between averages could be explained by a greater variability of the within-subject standard deviations of either average.
Calculations based on a pilot sample of 14 subjects suggested that the number of subjects necessary to achieve a statistical power of 95%, at a statistical level of significance of 5%, was 61. The sample size calculation was determined from an initial sample of 15 subjects using the statistical freeware G*Power (version 3.0.5), downloaded from the Internet and used as described elsewhere.Citation23 Statistical analyses were made using the Graphpad Instat for Windows program, version 3.00 (Graphpad Software Inc, San Diego, CA, www.graphpad.com).
Results
The mean subject age was 22 ± 1 (range 20–25) years. There were 46 (69.7%) men and 20 (30.3%) women in the study group.
IOP measurement by PT100 versus GAT
The mean IOP readings, SDs, range of values, and repeatability coefficients obtained by each technique in the two measurement sessions are described in . While both techniques returned equal IOP values in the first measurement session, there was a mean difference in the average IOP at the second measurement session (1 ± 0.71). These mean differences were not statistically significant (P > 0.05, paired t-test), with the PT100 underestimating the IOP measurement by −1.00 mmHg.
Table 1 Intraocular pressure values and difference between the tested techniques in mmHg
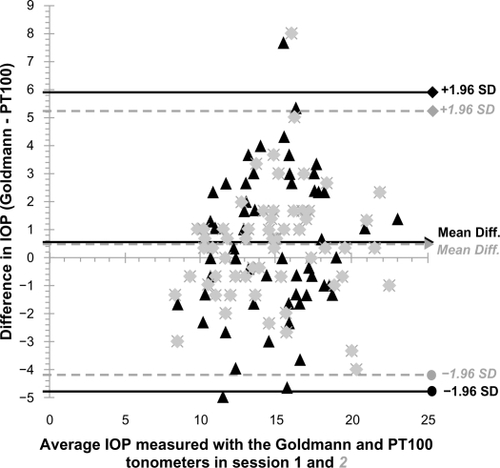
The limits of agreement between the techniques are shown in . The coefficient of agreement between the techniques was 7.5 mmHg for the first measurement session and 6.1 mmHg for the second measurement session. About 97.2% of the mean IOP measurements obtained by both instruments were in agreement by ≤3 mmHg on intersession analysis.
Figure 1 Intrasession variation of IOP with the Goldmann applanation tonometer in sessions 1 and 2. The mean difference of triplicate IOP measurements for each subject; 95% limits of agreement are depicted by the three lines.
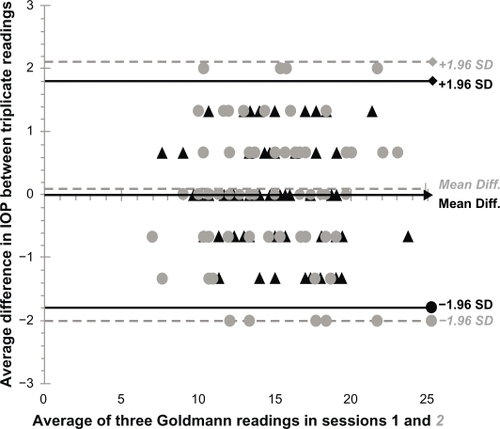
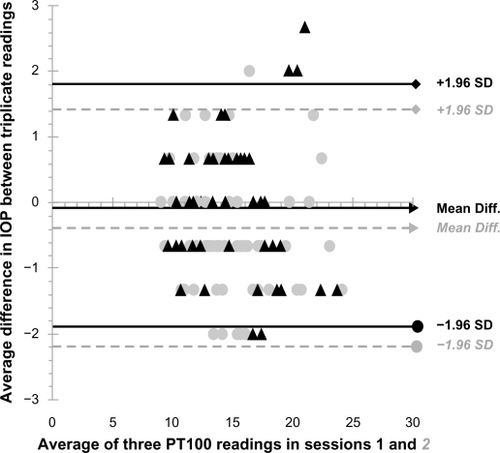
Figure 2 Intrasession variation of IOP with the PT100 noncontact tonometer in sessions 1 and 2. The mean difference of triplicate IOP measurements for each subject; 95% limits of agreement are depicted by the three lines.
In the comparison of six columns of differences, there was no statistically significant difference (P > 0.05, repeated measures one-way analysis of variance). The six columns computed were the column of differences for the PT100 in sessions 1 and 2, the column of differences for the GAT in sessions 1 and 2, and the between-technique difference in sessions 1 and 2.
Repeatability and reproducibility
The intrasession IOP mean difference for GAT sessions 1 and 2 was 0 ± 0.90 mmHg and 0.04 ± 1.06 mmHg, respectively. The corresponding mean difference in IOP measurement for PT100 sessions 1 and 2 was −0.06 ± 0.96 and −0.39 ± 0.94 mmHg, respectively. The variation between the intrasession difference columns was not statistically significant (P > 0.05, paired t-test).
When repeated, the repeatability coefficients for the GAT and PT100 noncontact tonometer IOP measurements were quite close, as shown in . A Bland–Altman analysis for the two measurement sessions using the 66 subjects returned an estimated bias with the GAT and the PT100 noncontact tonometer of 0. 49 mmHg (95% confidence interval, −0.36 to 1.61 for both techniques) with 95% limits of agreement of −2.0 to 2.1 and −2.2 to 1.8. The repeatability differences in IOP as assessed with the PT100 did not vary significantly from those of the GAT (P > 0.05, paired t-test).
The repeatability coefficient for test–retest differences using both techniques was within ±5 mmHg for both the GAT and the PT100 noncontact tonometer ().
Figure 3 Test-retest variation of the Goldmann applanation tonometer and the Reichert PT100 IOP measurements. The mean differences between both sessions, and the 95% limits of agreement are depicted by the three lines.
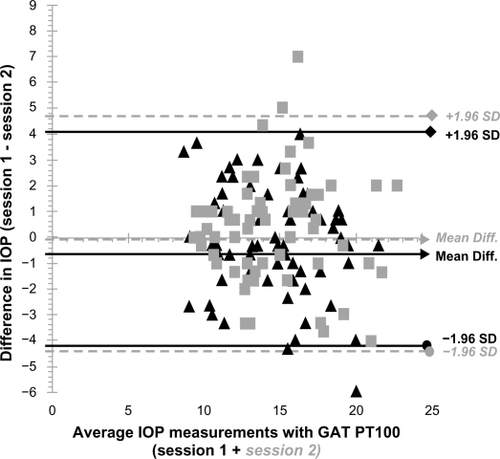
Figure 4 Differences in IOP, measured in 1st and 2nd sessions, between the Goldmann tonometer and the PT100 noncontact tonometer plot against their average, with the mean difference and 95% limits of agreement depicted by the three lines.
In assessing the reproducibility of the two techniques when measurements were taken by two different observers, the reproducibility coefficients in mean difference for both the GAT and the PT100 noncontact tonometer on a Bland–Altman plot was −0.115 mmHg, which did not vary significantly (P > 0.05, paired t-test). There was no significant correlation (P > 0.05, Pearson’s r) between the magnitude of IOP measurements within sessions for the same technique ( and ), between sessions for the same technique (), and between techniques ().
The within-subject standard deviation derived from a comparison of every paired comparison of averages revealed the variation was insignificant (P > 0.05, one-way analysis of variance).
Discussion
The Reichert PT100 noncontact tonometer has a repeatability coefficient similar to that of the GAT. When both instruments are used to measure IOP in the same individual, there is a 95% chance that the difference between the two instruments will not exceed 1 mmHg. The repeatability coefficients found in our study were ±1.8 mmHg and ±2.1 mmHg for the GAT (sessions 1 and 2), and ±1.9 mmHg and +1.8 mmHg for sessions 1 and 2 for the Reichert PT100 noncontact tonometer (sessions 1 and 2). Although the repeatability coefficient for the GAT was 0.1 mmHg superior to the PT100 in the first session, the PT100 was stronger in the second session. Overall, both instruments showed good repeatability, with the PT100 noncontact tonometer being more consistent in repeated measurement sessions. Two other studiesCitation5,Citation6 have also shown similar repeatability coefficients for the GAT, ±2.5 mmHg5 and 3.70 mmHg6 when compared with other noncontact tonometers.Citation5,Citation6
Notable in this study is the identical within-session differences for the PT100 and the GAT for both sessions 1 and 2. This means that both techniques have the same consistency in their measurements and can be interchanged in follow-up situations where a patient’s previous IOP measurements had been taken with either one of the tonometers.
Clinical agreement between the noncontact tonometer and the GAT has been demonstrated in previous studies of normotensive subjects,Citation5,Citation6,Citation29,Citation30 with a propensity for the noncontact tonometer to return about 3 mmHg higher IOP measurements than the GATCitation7,Citation8,Citation27,Citation28 in subjects with IOPs up to 21 mmHg.
In one of the two previous published studies comparing the PT100 and the GAT, a strong agreement was observed between the two instruments.Citation10,Citation11 In the study by Salim et alCitation10 a close level of agreement in the normal range of IOPs was observed, with an increased variation as the magnitude of measurements increased. Ninety-eight subjects aged 62.6 ± 13.8 years had IOP measurements of 15.65 ± 4.26 mmHg and 15.98 ± 5.48 mmHg for the PT100 and the GAT, respectively. While their result is similar to ours, in comparative analysis of the agreement of the two instruments, our subjects’ mean IOP measurements varied slightly from theirs (15 ± 3 mmHg, PT100 and GAT) and the mean IOP did not differ in the PT100 and the GAT. The large age variation of the subjects in the study by Salim et al could explain this discrepancy, because all of our subjects were in a younger age group (22 ± 1 years). This shows that the PT100 IOP measurement results are the same as for the GAT in normal healthy young subjects.Citation10
In this study, the average IOP measured by both tonometers was the same, and no significant difference was found between the repeatability and reproducibility coefficients for the GAT and the PT100 noncontact tonometer.
The portability and ease of use of the PT100 noncontact tonometer makes it an ideal IOP measuring device for use in children during screening programs or in situations where a technician has to take IOP measurements in clinic. Just like previous noncontact tonometers, it has some limitations, ie, the need for adequate experience and expertise in order to take accurate measurements, and the absence of a headrest, making proper fixation a necessary requirement to acquire accurate measurements. Of consideration also is the effect of corneal properties on both the GAT and noncontact tonometers, with the latter being more affected by central corneal thickness than the GAT.Citation25,Citation26 Because of the relative low number of subjects, further studies on the reliability of the PT100 noncontact tonometer in subjects with higher IOPs is important and the effects of central corneal thickness on its measurements verified to confirm the report from Murase et alCitation11 that the PT100 is more affected by variations in central corneal thickness than the GAT. However, further study in subjects with higher IOP and elderly patients is needed to confirm the agreement between the two methods.
In summary, this study has shown that the PT100 is an accurate and reliable method for assessing IOP in normotensive young subjects. The PT100 IOP readings are reproducible when two examiners take separate measurements, and are interchangeable with IOP measurements obtained with the GAT.
Acknowledgements
The author would like to thank Dr Kelechi Ogbuehi for his assistance with data collection for this study.
Disclosure
The author reports no conflicts of interest in this work.
References
- The AGIS InvestigatorsThe Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deteriorationAm J Ophthalmol2000130442944011024415
- LitchterPRMuschDCGillespieBWCIGTS Study GroupInterim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgeryOphthalmology2001108111943195311713061
- GuptaVSonyPAgarwalHCSihotaRSharmaAInter-instrument agreement and influence of central corneal thickness on measurements with Goldmann, pneumotonometer and noncontact tonometer in glaucomatous eyesIndian J Ophthalmol200654426126517090879
- LamAKChanRLamCHThe validity of a new noncontact tonometer and its comparison with the Goldmann tonometerOptom Vis Sci200481860160515300119
- AlmubradTMOgbuehiKCThe effect of repeated applanation on subsequent IOP measurementsClin Exp Optom200891652452918651843
- García-ResúaCGiráldez FernándezMJYebra-PimentelEGarcía-MonteroSClinical evaluation of the Canon TX-10 noncontact tonometer in healthy eyesEur J Ophthalmol201020352353020037897
- RegineFScuderiGLCesareoMRicciFCedroneCNucciCValidity and limitations the Nidek NT-4000 non-contact tonometer: A clinical studyOphthalmic Physiol Opt2006261333916390480
- OgbuehiKCAssessment of the accuracy and reliability of the Topcon CT80 non-contact tonometerClin Exp Optom200689531031416907669
- Van der JagtLHJansoniusNMThree portable tonometers, the TGDc-01, the ICARE and the Tonopen XL, compared with each other and with Goldmann applanation tonometryOphthalmic Physiol Opt200525542943516101949
- SalimSLinnDJEcholsJRNetlandPAComparison of intraocular pressure measurements with the portable PT100 noncontact tonometer and Goldmann applanation tonometryClin Ophthalmol2009334134419668588
- MuraseHSawadaAMochizukiKYamamotoTEffects of corneal thickness on intraocular pressure measured with three different tonometersJpn J Ophthalmol20095311619184301
- StockerFWOn changes in intraocular pressure after application of the tonometer; in the same eye and in the other eyeAm J Ophthalmol195845219219613508786
- MosesRARepeated applanation tonometryOphthalmologica196114266366814476465
- BynkeHGSchéleBOn the origin of the ocular pressure pulseOphthalmologica1967153129366049143
- LeydheckerWThe intraocular pressure: Clinical aspectsAnn Ophthalmol1976843893921267312
- PerkinsESThe ocular pulseCurr Eye Res19811119237297091
- KrakauCEWilkeKOn repeated tonometryActa Ophthalmol (Copenh)19714946116145171572
- ChauhanBCHensonDBClinical evaluation of the non-contact tonometer Mark IIAm J Optom Physiol Opt19886597517563189501
- BaudouinCGastaudPInfluence of topical anesthesia on tonometric values of intraocular pressureOphthalmologica199420863093137845645
- AlmubradTMOgbuehiKCOn repeated corneal applanation with the Goldmann and two non-contact tonometersClin Exp Optom2010932778220406256
- LiuJHKripkeDFTwaMDTwenty-four-hour pattern of intraocular pressure in the aging populationInvest Ophthalmol Vis Sci199940122912291710549652
- BlandJMAltmanDGStatistical methods for assessing agreement between two methods of clinical measurementLancet1986184763073102868172
- BlandJMAltmanDGMeasuring agreement in method comparison studiesStat Methods Med Res19998213516010501650
- FaulFErdfelderELangAGBuchnerAG*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciencesBehav Res Methods200739217519117695343
- TonnuPAHoTNewsonTThe influence of central corneal thickness and age on intraocular pressure measured by pneumotonometry, non-contact tonometry, the Tono-Pen XL, and Goldmann applanation tonometryBr J Ophthalmol200589785185415965165
- KoYCLiuCJHsuWMVarying effects of corneal thickness on intraocular pressure measurements with different tonometersEye (Lond)200519332733215258603
- JorgeJDíaz-ReyJAGonzález-MéijomeJMAlmeidaJBParafitaMAClinical performance of the Reichert AT550: A new non-contact tonometerOphthalmic Physiol Opt200222656056412477021
- JorgeJGonzález-MéijomeJMDíaz-ReyJAAlmeidaJBRibeiroPParafitaMAClinical performance of non-contact tonometry by Reichert AT550 in glaucomatous patientsOphthalmic Physiol Opt200323650350614622352
- Moreno-MontañésJGómez-DemmelELajara-BlesaJAliseda-Pérez de MadridDComparative study of three non-contact tonometers and the Goldmann tonometerOphthalmologica199420831151188065693
- SorensenPNThe noncontact tonometer: Clinical evaluation on normal and diseased eyesActa Ophthalmol (Copenh)19755345135211242275