
Abstract
Purpose
Cataract surgery in patients suffering from zonular weakness can be difficult and lead to severe complications. The insertion of capsular tension rings to stabilize the capsular bag along all steps of the phacoemulsification is an option, although can be difficult to remove intra- or post-operatively. A capsular tension ring with a thread is a safe alternative, which allows its easy removal at the end of the surgery.
Patients and methods
Retrospective study of regular practice on 14 patients with zonular weakness who underwent phacoemulsification. Among them, 12 suffered from pseudo-exfoliative syndrome and 2 suffered from a post-traumatic cataract. All benefited from the use of a capsular tension ring with a thread during their surgery.
Results
All surgeries were successful. Capsular tension ring with a thread was all removed at the end of surgery without any complication.
Conclusion
The addition of a thread to the capsular tension ring is a simple modification that enhances its use by facilitating its intraoperative removal if necessary or at the end of surgery.
Introduction
The author estimates that between 150,000 and 200,000 cataract surgeries a year are performed in Algeria. According to the DREES in France, this is the most common surgery performed, with nearly 830,000 completed in 2016.Citation1 One of the main, serious intraoperative complications of cataract surgery is the posterior dislocation of the lens or its nucleus, caused by capsular rupture or zonular disinsertion. This complication is common in patients who have experienced previous zonular fragility and is present in numerous etiologies,Citation2,Citation3 in order of frequency: the zonular degeneration of pseudo-exfoliative syndromes (estimated at 25–30% of the causes in Algeria),Citation4–Citation7 eye injuries,Citation7,Citation8 strong myopia,Citation7 history of vitreoretinal surgery, fibroelastic tissue pathologies in Marfan’s diseaseCitation7,Citation9 or homocystinuria.Citation10
The capsular or zonular tension ring (CTR) was designed in the early 1990sCitation11 to stabilize the capsular bag and consolidate weak zonules during all stages of surgery, including phacoemulsification.Citation3,Citation7,Citation12–Citation15 It distributes the tension forces acting on the still functional zonular fibers and thus reduces the risk of capsular failure and posterior dislocation of the lens.Citation11,Citation15 However, its withdrawal is difficult and can be traumatic. It is therefore generally left in place at the end of surgery or even fixed to the sclera.Citation14 Nevertheless, it is preferable to leave a minimum of foreign bodies in the surgical site, and consequently, CTR is a relatively unused tool even in cases of phacodonesis.
The aim of this study is to describe how the employment of a thread facilitates the use of the tension ring and allows its removal at the end of phacoemulsification on a weak zonule.
Materials And Methods
Surgical Technique
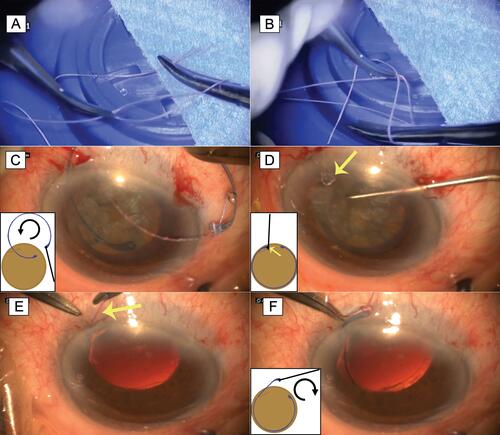
The surgical technique consisted in the use of a thread (Vicryl violet 7/0, Ethicon, NJ, USA) attached to the eye of the CTR (Medicontur, Limas, France), at the end of the medical device, by a knot and a counter-node ( and ). The tension ring was placed inside the anterior chamber, in the capsular bag, under the anterior capsulorhexis by a counterclockwise movement, allowing the zonule to be tensioned ( and ). The thread then came out outside the eye through the incision. The zonule was thus stabilized during all phacoemulsification steps. At the end of the surgery, after the placement of a large diameter implant and cohesive viscoelastic (Provisc, Alcon Laboratories, TX, USA), the ring was removed using the thread sticking out from the incision by a clockwise movement ( and ). A video support is available online at http://youtu.be/9vazuWf0Djg.
Figure 1 (A) Passing of the thread at one end of the capsular tension ring and hanging of the suture with a knot. (B) Counter knot. (C) Placing the ring in the capsular bag under the anterior capsulorhexis, by a counterclockwise movement. (D) Capsular ring in place. The knot is placed inside, under the iris (yellow arrow) and the thread emerges through the incision. (E and F) Removal of the tension ring by pulling of the thread protruding from the incision (yellow arrow) clockwise.
Patients
This real-life retrospective study involved 14 eyes of 14 patients (9 men and 5 women aged between 33 and 80 years) operated on by phacoemulsification by the same surgeon (Dr N. Oudjani) between 12th October 2015 and 2nd November 2017 at the outpatient ophthalmology clinic in Skikda (Algeria). All the patients signed an inform consent form before the cataract surgery. Patient consent to review their medical records was not required by an institutional review board and local law in Algeria for this type of real-life retrospective analysis including a surgery using common devices as the CTR and surgical thread. However, patient data confidentiality and compliance were respected. All had zonular weakness discovered intraoperatively: 12 suffered from pseudo-exfoliation of the capsular and 2 from post-traumatic lesions. All patients were reviewed post-operatively at D1, D3, D15, D30 and every 3 months thereafter.
Results
The phacoemulsifications were carried out without incident and the tension rings with a thread were removed each time without complication at the end of the surgery. No dislocation or subluxation was noted during post-operative follow-up (mean 14.5 months, from 3 to 28 months).
Discussion
Cataract surgery on weak zonules can be risky.Citation16 A solution to zonules weakness is the use of CTR during surgery. However, this practice remains limited due to difficulties relating to its removal, post-operative complications such as dislocation in the vitreous of the capsular bag, implant and ring assembly,Citation2 and the existence of alternative techniques (implantation in the sulcus,Citation17 implant clipped to the irisCitation18). Our technique involving a knotted thread at one end of the ring not only stabilizes the fragile capsular bag, but also allows its removal quickly and safely in the event of complications during installation and permits its safe removal at the end of the surgery. The placement and the removal of the thread are fast (around less than 1 min), without complications on the analyzed series. The post-operative procedure is comparable to a normal one. The thread, out of the eyeball, is sufficiently loose for not exerting any risky traction of the anterior capsule during the surgery and when it is removed even in case of risky situations as very deep anterior chamber (high myopia) or swinging anterior chamber depth or small anterior capsulorhexis.
Conclusion
The CTR is an excellent option for consolidating weak zonules during phacoemulsification procedures. Our suture security technique using a CTR with a thread eliminates the risk of it falling into the vitreous during the procedure and facilitates its removal at the end of the surgery.
Acknowledgments
We would particularly like to thank Victor Lambert, an ophthalmology intern at the University Hospital of Saint-Etienne, for his contribution to the review of this article and his wise advice, as well as Bouchta Karrich of Laboratoires Théa for his bibliographical research.
Disclosure
The authors have declared that no competing interest exists. This study does not include financial support. The authors have no proprietary or commercial interest in any materials discussed in this article and have no conflicts of interest in this work.
References
- De Peretti C, Oberlin P, Villain M, Daien V Le traitement de la cataracte primaire est la plus fréquente des interventions chirurgicales. DREES, Etudes et Résultats. 2018. Available from: https://drees.solidarites-sante.gouv.fr/IMG/pdf/er_1056.pdf. Accessed March 28, 2019.
- Li B, Wang Y, Malvankar-Mehta MS, Hutnik CM. Surgical indications, outcomes, and complications with the use of a modified capsular tension ring during cataract surgery. J Cataract Refract Surg. 2016;42(11):1642–1648. doi:10.1016/j.jcrs.2016.10.007
- Weber CH, Cionni RJ. All about capsular tension rings. Curr Opin Ophthalmol. 2015;26(1):10–15. doi:10.1097/ICU.0000000000000118
- Skuta GL, Parrish RK 2nd, Hodapp E, Forster RK, Rockwood EJ. Zonular dialysis during extracapsular cataract extraction in pseudoexfoliation syndrome. Arch Ophthalmol. 1987;105(5):632–634. doi:10.1001/archopht.1987.01060050050035
- Schlotzer-Schrehardt U, Naumann GO. A histopathologic study of zonular instability in pseudoexfoliation syndrome. Am J Ophthalmol. 1994;118(6):730–743. doi:10.1016/S0002-9394(14)72552-8
- Sein J, Galor A, Sheth A, Kruh J, Pasquale LR, Karp CL. Exfoliation syndrome: new genetic and pathophysiologic insights. Curr Opin Ophthalmol. 2013;24(2):167–174. doi:10.1097/ICU.0b013e32835d5d11
- Jiraskova N, Rozsival P, Urminsky J. [Results of 32 cataract operations using the capsular ring]. Cesk Slov Oftalmol. 2001;57(3):165–168.
- Marin MI, Tejero TR, Dominguez FM, Gutierrez ME. Ocular injuries in midfacial fractures. Orbit. 1998;17(1):41–46. doi:10.1076/orbi.17.1.41.7950
- Mir S, Wheatley HM, Hussels IE, Whittum-Hudson JA, Traboulsi EI. A comparative histologic study of the fibrillin microfibrillar system in the lens capsule of normal subjects and subjects with Marfan syndrome. Invest Ophthalmol Vis Sci. 1998;39(1):84–93.
- Harrison DA, Mullaney PB, Mesfer SA, Awad AH, Dhindsa H. Management of ophthalmic complications of homocystinuria. Ophthalmology. 1998;105(10):1886–1890. doi:10.1016/S0161-6420(98)91035-1
- Menapace R, Findl O, Georgopoulos M, Rainer G, Vass C, Schmetterer K. The capsular tension ring: designs, applications, and techniques. J Cataract Refract Surg. 2000;26(6):898–912. doi:10.1016/S0886-3350(00)00446-6
- Gimbel HV, Sun R, Heston JP. Management of zonular dialysis in phacoemulsification and IOL implantation using the capsular tension ring. Ophthalmic Surg Lasers. 1997;28(4):273–281.
- Moreno-Montanes J, Sainz C, Maldonado MJ. Intraoperative and postoperative complications of Cionni endocapsular ring implantation. J Cataract Refract Surg. 2003;29(3):492–497. doi:10.1016/S0886-3350(02)01604-8
- Cionni RJ, Osher RH. Management of profound zonular dialysis or weakness with a new endocapsular ring designed for scleral fixation. J Cataract Refract Surg. 1998;24(10):1299–1306. doi:10.1016/S0886-3350(98)80218-6
- Rai G, Sahai A, Kumar PR. Outcome of Capsular Tension Ring (CTR) implant in complicated cataracts. J Clin Diagn Res. 2015;9(12):NC05–NC07. doi:10.7860/JCDR/2015/10425.6999
- Lu LW, Fine IH. Phacoemulsification in Difficult and Challenging Cases. Thieme; 1999.
- Mohebbi M, Bashiri SA, Mohammadi SF, et al. Outcome of single-piece intraocular lens sulcus implantation following posterior capsular rupture during phacoemulsification. J Ophthalmic Vis Res. 2017;12(3):275–280. doi:10.4103/jovr.jovr_181_15
- Raciti MW, Majmudar PA. Phakic IOLs: sulcus versus iris-claw versus angle-supported: complications and outcomes. Curr Ophthalmol Rep. 2013;1(1):45–49. doi:10.1007/s40135-012-0001-1