
Abstract
Purpose
To evaluate the efficacy and safety of a closed-chamber air bubble capsulotomy technique to prevent the Argentinean flag sign (AFS) in patients with white and intumescent cataracts.
Setting
Sohag University, Faculty of Medicine, Ophthalmology Department, Sohag, Egypt.
Design
Prospective interventional noncomparative case series.
Methods
Eighty-two eyes of 80 patients with white and intumescent cataracts were included. Eyes with any ocular pathology other than cataract or eyes subjected to previous intraocular surgery were excluded. Needle capsulorhexis was performed under a large air bubble tamponade without capsular staining. Efficacy of the technique was assessed intraoperatively by successful completion of capsulorhexis. Safety of the technique was assessed by the occurrence of intraoperative or postoperative complications.
Results
Complete capsulorhexis by the closed-chamber air bubble technique was successful in 75 eyes (91.5%), while capsulorhexis extension occurred in seven eyes. In four eyes with extension, the procedure was shifted to the standard technique of CCC (circular curvilinear capsulorhexis), using a viscoelastic device. A shift to extracapsular cataract extraction (ECCE) surgery occurred in the remaining three eyes, as the extension was so far-gone. No intraoperative or postoperative complications were observed.
Conclusion
The closed anterior chamber air bubble technique for capsulorhexis is a novel, safe, and effective technique to prevent AFS in white and intumescent cataracts. It is also time-saving and cost-effective, with less likelihood of capsulorhexis extension. The technique is considered a valuable addition to previously described techniques.
Introduction
Achieving an intact capsulorhexis is a key step in successful and safe phacoemulsification. White and intumescent cataracts are challenging cases for almost all surgeons, because of the high risk of radial extension of the capsulorhexis.Citation1,Citation2 In such eyes, during creation of the capsulorhexis, the pressure created by hyper-hydration of the lens fibers can cause spontaneous tears that extend to the periphery. This is referred to as the Argentinean flag sign (AFS). Once this occurs, the cataract surgery may become extremely difficult, owing to poor construction of the capsulorhexis and possible rupture of the posterior capsule.Citation3
Several techniques have been described for more predictable, safer capsulorhexis creation, including two-stage capsulorhexis, the use of trypan blue dye, aspiration of the lens cortex using a 30-gauge needle, enhancement of anterior capsular visualization using an endoilluminator, creation of the capsulorhexis using micro-capsulorhexis forceps through a single side-port incision of 0.8 mm under a high-density viscoelastic, and femtosecond laser-assisted capsulotomy.Citation4–Citation9
In spite of the use of various methods, capsulorhexis extension may occur. Here, we evaluate a novel technique of needle capsulorhexis under a large air bubble tamponade in a mature cataract without staining.
The aim of this study was to evaluate the intraoperative difficulties, efficacy, and safety of using a large air bubble tamponade to perform circular curvilinear capsulorhexis (CCC) while preserving the anterior chamber (AC) and maintaining capsular flap visualization. We also aimed to add a new technique to the list of established techniques for the prevention of AFS and offer alternative options for cataract surgeons.
Patients And Methods
This prospective study was conducted on 82 eyes of 80 consecutive patients with mature, intumescent, white cataracts, who attended outpatient clinics of the Ophthalmology Department, Sohag University from September 2017 to August 2018.
The study adhered to the tenets of the Declaration of Helsinki. Institutional review board approval was obtained from the Ethical Committee of Sohag Faculty of Medicine. All patients with mature, intumescent, or white cataracts were included in the study.
Exclusion Criteria
Eyes with immature cataracts, subluxated lenses, glaucoma, uveitis, previous intraocular surgery, preoperative high intraocular pressure, a calcified anterior capsule, or history of trauma were excluded. The following data were collected: age, gender, intraoperative or postoperative complications.
Preoperative Preparation
Written informed consent was obtained from all patients, after which a full ophthalmological examination was performed preoperatively. Acetazolamide 500 mg was administered orally on the morning of the operation. Cyclopentolate 1%, tropicamide 1%, and phenylephrine 10%, were administered for mydriasis, and nonsteroidal anti-inflammatory eye drops were administered to maintain pupillary dilatation and avoid intraoperative miosis. These eye drops were administered 1 hr before surgery.
Benoxinate hydrochloride was used as topical anesthesia. All eyes were operated on, under the effect of retrobulbar anesthesia. All surgeries were performed by a single surgeon (AHS).
Surgical Technique
A bent cystotome with a 70° angle was made by a 26-gauge needle. The closed globe was stabilized by toothed forceps. A 26-gauge cystotome was introduced at a 10 o’clock position by direct entry of the tip through the clear corneal periphery, without making the usual side-port incision. Aqueous aspiration was performed with caution to avoid anterior capsule injury, after which the cystotome was removed from the AC. After evacuation of some of the aqueous humor and air filling through the same puncture, the cystotome was reintroduced to the AC. The AC was then enlarged by the injection of a large air bubble through the bent cystotome, which facilitated flattening of the anterior capsule ().
Fine movements of the globe in different directions were performed to reach the reflection rings of a light microscope at different tissue levels. Fine movements are usually needed to maintain visualization of the running edge of the flap of the capsulorhexis (). A punching incision was performed in the central area of the anterior capsule under the effect of air tamponade, and a flap was thereby created. The edge of this flap was flipped and reflected upon the underlying capsule ().
The reflected flap was manipulated by the cystotome tip near the torn edge. The edge was rotated () with repeated repositioning of the cystotome to be adjacent to the tear until continuous curvilinear anterior capsulorhexis was achieved. Visualization of the anterior capsule was achieved by light reflection at the torn edge of the capsule (, ). Light reflections were generated at different tissue levels under the large air bubble.
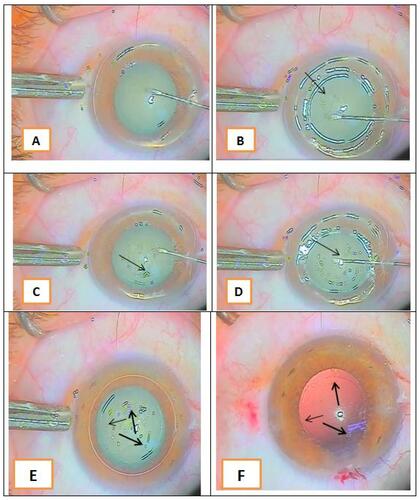
shows reflection rings; one at the peripheral iris plane, one at the aqueous meniscus, one at the edge of the pupil, and another at the plane of the capsulorhexis.
Figure 1 (A) Starting capsulorhexis; (B) multiple light reflection rings at different tissue levels (arrow shows the capsulorhexis edge); (C) progression of capsulorhexis guided by light reflection at the torn capsular edge (arrow shows the capsulorhexis edge); (D) closing of capsulorhexis (arrow shows the capsulorhexis margin to the end of the circle); (E) arrows showing the completed circular capsulorhexis; and (F) arrows showing the complete capsulorhexis against a red reflection after phacoemulsification.
The supplementary video clearly reveals multiple light reflection rings with obscuration, and the appearance of these reflection rings during fine movements of the globe.
Results
A total of 82 eyes of 80 patients met the inclusion criteria. There were 43 eyes of males and 37 eyes of females. Thirty-eight were right eyes. The mean age of patients was 62.30 ± 8.23 years (range 43–86 years). Capsulorhexis was completed in 75 eyes (91.5%), while capsulorhexis extension occurred in seven eyes (8.5%). In four eyes with extended rhexis, a shift was made to the usual technique of CCC using a viscoelastic device. In the remaining three eyes with extension, a shift to extracapsular cataract extraction (ECCE) surgery was made as the extension was so far-gone. No intraoperative or postoperative complications were reported.
Discussion
Anterior capsulorhexis in white cataracts remains a challenge, with the risk of rhexis extension. Different techniques have been described by surgeons to successfully complete the capsulorhexis and prevent AFS in white and intumescent cataracts. Each technique has its drawbacks and may not be suitable for all surgeons. The use of viscoelastics,Citation10 or a cannula attached to the infusion bottle raised high enough to give adequate depth to the AC is a common surgical practice.Citation11
Leakage may occur from the side-port with the use of viscoelastics. In addition, reinjection may be necessary as the AC becomes more shallow and peripheral movement of the flap becomes more likely. Such use of viscoelastics can also cause the flap edge to become wavy, thereby necessitating continuous bending of the capsule. On the other hand, Oksuz et al.Citation12 reported aspiration of the liquefied cortical material with a cannula while maintaining a formed anterior chamber by irrigating fluids, which is time-consuming. When a 27- or 30-gauge needle is used to remove the liquefied cortex, it is possible that an insufficient volume may be removed; thus, a spontaneous capsular tear may still occur.
Here, we described a closed-chamber air bubble technique without capsular staining, as an addition to previously described capsulorhexis saving techniques. The technique described in the present study offers an alternative option for ophthalmologists, depending on the available facilities and level of experience. The success rate of this technique in achieving complete capsulorhexis was (91.5%). The seven eyes with capsulorhexis extension were cases in which the technique was implemented at an early stage.
The main advantage of the large air bubble is the tamponade effect, which counteracts the high intralenticular pressure in the white cataractous lens; it also prevents the leakage of the liquefied lens material to the AC during anterior capsulorhexis.
The maintenance of a closed AC prevents the drawbacks of sudden decompression of the lens, which may lead to rhexis extension and unsuccessful phacoemulsification. In this study, sudden decompression of the AC did not occur because the it remained firmly closed through the use of a needle. Even if air escaped, it would have been a very small amount that could have been managed by reinjection of air with the same syringe, which would have been already filled with air, without exiting the AC.
In addition, our technique offers crucial advantages of no additional cost. No special device is used, neither are any instruments required, except those already used in conventional phacoemulsification surgery. Moreover, the technique is not overly time-consuming, as the steps of capsular staining, injection and reinjection of viscoelastic material, and the aspiration of liquefied cortical material are not performed. We did not use capsular staining, as visualization was enhanced by optical reflection at the torn edge of the anterior capsule.
Conclusion
The closed-AC air bubble technique for capsulorhexis is a novel, safe, and effective technique in the treatment of white and intumescent cataracts. It is also time-saving and cost-effective, with a reduced risk of capsulorhexis extension. It is considered a valuable addition to previously described techniques.
Ethical Approval
All procedures involving human participants were performed in accordance with the ethical standards of the National Research Committee, the 1964 Helsinki Declaration and its later amendments, or comparable ethical standards. Written informed consent was obtained from the patients after explanation of the treatment plan.
Disclosure
The authors report no conflicts of interest in this work.
References
- Jacob S, Agarwal A, Agarwal A, et al. Trypan blue as an adjunct for safe phacoemulsification in eyes with white cataract. J Cataract Refract Surg. 2002;28:1819–1825. doi:10.1016/s0886-3350(01)01316-5
- Chakrabarti A, Singh S. Phacoemulsification in eyes with white cataract. J Cataract Refract Surg. 2000;26:1041–1047. doi:10.1016/s0886-3350(00)00525-3
- Christopher C. Phaco capsulotomy: a technique to prevent the argentinean flag sign. Clin Ophthalmol. 2017;11:1937–1940. doi:10.2147/OPTH.S138676
- Melles GR, de Waard PW, Pameyer JH, Houdijn Beekhuis W. Trypan blue capsule staining to visualize the capsulorhexis in cataract surgery. J Cataract Refract Surg. 1999;25:7–9. doi:10.1016/s0886-3350(99)80004-2
- Mansour AM. Anterior capsulorhexis in hypermature cataracts. J Cataract Refract Surg. 1993;19:116–117. doi:10.1016/s0886-3350(13)80299-4
- Figueiredo CG, Figueiredo J, Figueiredo GB. Brazilian technique for prevention of the argentinean flag sign in white cataract. J Cataract Refract Surg. 2012;38:1531–1536. doi:10.1016/j.jcrs.2012.07.002
- Rao SK, Padmanabhan P. Capsulorhexis in white cataracts. J Cataract Refract Surg. 2000;26:477–478. doi:10.1016/s0886-3350(00)00354-0
- Robinson MS, Olson RJ. Simple approach to prevent capsule tear-out during capsulorhexis creation in hypermature cataracts. J Cataract Refract Surg. 2015;41:1353–1355. doi:10.1016/j.jcrs.2015.06.002
- Titiyal JS, Kaur M, Singh A, Arora T, Sharma N. Comparative evaluation of femtosecond laser-assisted cataract surgery and conventional phacoemulsification in white cataract. Clin Ophthalmol. 2016;10:1357–1364. doi:10.2147/OPTH.S108243
- Polat A. Needle capsulorhexis: the importance of using an anterior chamber maintainer. J Cataract Refract Surg. 2003;29:1248–1249. doi:10.1016/s0886-3350(03)00475-9
- Sethi HS, Dada T, Rai HK, Sethi P. Closed chamber globe stabilization and needle capsulorhexis using irrigation hand piece of bimanual irrigation and aspiration system. BMC Ophthalmol. 2005;5:21. doi:10.1186/1471-2415-5-21
- Oksuz H, Daglioglu MC, Coskun M, et al. Vacuum-assisted continuous circular capsulorhexis using bimanual irrigation and aspiration system of phaco machine in immature cataract. J Ophthalmol. 2013;2013:921646. doi:10.1155/2013/670242