Abstract
Purpose:
This paper compares the outcomes of the Ex-PRESS® Glaucoma Filtration Device (Alcon, Fort Worth, TX) implant observed in Japanese patients for 1 year with those of patients undergoing trabeculectomy.
Patients and methods:
The subjects comprised ten eyes of ten cases with open-angle glaucoma for which filtration surgery using Ex-PRESS (P-50) was performed by one operator from February 2008 and observed for at least 1 year (Ex-PRESS Group), and eleven eyes of eleven cases for which trabeculectomy was performed by the same operator (TE Group). For both groups, mitomycin C was used and a scleral flap was created after a fornix-based incision of the conjunctiva.
Results:
Hypotony and choroidal detachment were observed as early postoperative complications during a 1-week period in one-third of the cases in the TE Group, and failing vision in about 45%, while these were seen in fewer cases in the Ex-PRESS Group. No significant difference in intraocular pressure (IOP) was observed during the period, but IOP variations on the day following the surgery were obviously narrower in the Ex-PRESS Group than in the TE Group. Visual acuity was significantly poorer from 1 week to 3 months in the TE Group while it was stable in the Ex-PRESS Group. The Ex-PRESS Group had fewer cases of laser suture lysis and fewer administrations of glaucoma eyedrop, and no cases of progression in the stage of visual field defect.
Conclusion:
Filtration surgery using the Ex-PRESS is unlikely to cause early complications in Japanese patients. Similarly to the trabeculectomy, the intermediate-term control of IOP showed favorable results.
Introduction
The Ex-PRESS® Glaucoma Filtration Device (Alcon, Fort Worth, TX) is a miniature drainage device used in glaucoma surgery, and is already approved and widely used in Europe and the US. Initially, it was inserted from the limbus into the anterior chamber and placed underneath the conjunctiva, but this method is likely to cause overfiltration, exposure of the Ex-PRESS, and other complications.Citation1–Citation4 The currently adopted method places it under the scleral flap, and desirable long-term results are now reported.Citation5–Citation8
The Ex-PRESS has yet to be recognized as a medical device in Japan and we are unaware of any reported postoperative outcomes in Japanese patients. This paper examines the intermediate-term outcome of the filtration surgery for 1 year after surgery using the Ex-PRESS for Japanese patients by comparing it with that of trabeculectomy performed by the same operator.
Patients and methods
The subjects comprised ten cases of ten eyes suffering from open-angle glaucoma for which a filtration surgery using the Ex-PRESS was performed by one of the authors (TS) at the department of ophthalmology in Osaka Medical College Hospital in and after February 2008 and observed for at least 1 year (Ex-PRESS Group), as well as eleven cases of eleven eyes suffering from open-angle glaucoma for which a trabeculectomy was performed in almost the same period by the same operator and observed for at least 1 year (TE Group). All cases were consecutive and their background factors are as shown in . There was no significant difference in any of these factors between the groups, except that the glaucoma in the Ex-PRESS Group tended to be at later stages according to Aulhorn-Greve’s classification, by which the stages of the patients’ visual field defects were classified into the stages 0–1, 2, 3, 4, 5, and 6 (0–1: early stage, 2–5: middle stage, 6: advanced stage).Citation9 This study was carried out after obtaining approval from the Ethics Committee of Osaka Medical College and after explaining the procedure to the patients and gaining their consent.
Table 1 Background factors of groups
The following describes the surgical techniques. For both groups, a scleral flap 4 mm × 4 mm was created after a fornix-based incision of the conjunctiva. A side port was also created after application of 0.04% mitomycin C (MMC) for 3 to 5 minutes and washing it with intraocular irrigating solution. After that, for the Ex-PRESS Group, pre-incision was performed in parallel with the surface of the iris using a 25G needle from the limbus toward the anterior chamber. At the same time, a viscoelastic substance was injected. After that, the Ex-PRESS device (P-50) was inserted along the puncture wound by the 25G needle. For the TE Group, an iridectomy followed a resection of a sclerotic block including the trabecula. After that, the scleral flap was sutured with 10-0 nylon for both groups. For the Ex-PRESS Group, the process normally placed two sutures at the two hinder corners of the sclerotic block and, depending on a degree of filtration, a few (two to four) sutures were added between the fore and hinder corners. For the TE Group, six sutures were placed (two at the two back corners and others between the fore and back corners) in principle. The conjunctiva was tightly sutured using 10-0 nylon for both groups. In cases where a cataract surgery was additionally performed, phacoemulsification and aspiration combined with intraocular lens implantation from other wounds were conducted after application of MMC.
Intraocular pressure (IOP) was measured by Goldmann applanation tonometry, and visual acuity was also evaluated before and after surgery. Postoperative complications, care and treatment were investigated in the groups. Success was determined by IOP between 5 and 21 mmHg at 1, 3, 6, 9, and 12 months with or without medications, without requiring further surgery or total loss of vision. Laser suture lysis and needling of the bleb were not considered as failures of the procedure.
The groups were compared using the unpaired t-test or Mann–Whitney U-test for continuous variables. Differences of categorical data or complications in the two groups were evaluated with Fisher’s exact test. Success in both groups was compared using Kaplan–Meier survival analysis and the log-rank test. P values of < 0.05 were considered statistically significant.
Results
In the TE Group, one-third of the cases exhibited hypotony and choroidal detachment during the week after surgery (). In nearly 40% of the cases, visual acuity had fallen by two or more levels. In the Ex-PRESS Group, these complications were all exhibited in a smaller number of cases.
Table 2 Early postoperative complications (1 week after surgery)
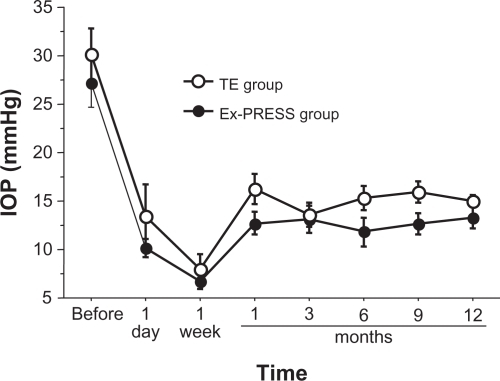
Twelve months after surgery, the IOP stood at 13.9 ± 4.0 mmHg (expressed as mean value ± standard error) in the Ex-PRESS Group and 14.9 ± 2.0 mmHg in the TE Group (). Overall, IOP was slightly lower in the Ex-PRESS Group, but there was no significant difference between the groups at any time. However, it is noteworthy that in the TE Group there were clearly substantial variations on the day after the surgery, whereas they were limited in the Ex-PRESS Group.
Figure 1 Time-course trends in intraocular pressure (IOP) of the Ex-PRESS Group and the conventional trabeculectomy (TE) Group.
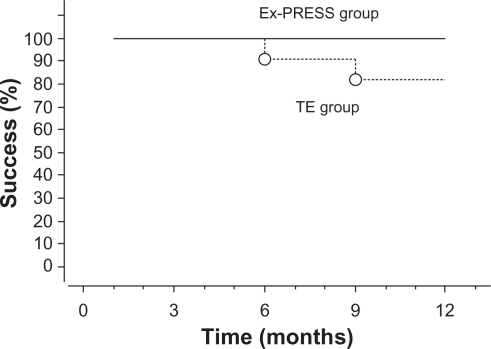
shows the Kaplan–Meier survival analysis for each group. According to the definition of success in this study, success rate was 100% for Ex-PRESS Group and 81.8% for TE Group at 1 year postoperatively, but there is not a significant difference between the groups (P = 0.167, log-rank test).
Figure 2 Kaplan–Meier survival analysis after implantation of the Ex-PRESS device under a scleral flap (Ex-PRESS Group, solid line) or conventional trabeculectomy (TE Group, dashed line). The success rate was 100% (Ex-PRESS Group) and 81.8% (TE Group) at 1 year postoperatively (P = 0.167, log-rank test).
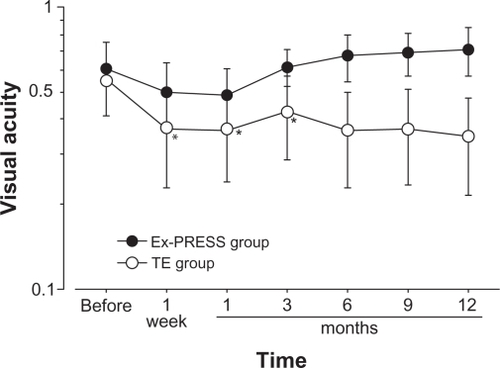
illustrates the trends in visual acuity of the two groups. For the purpose of assessing the impact of the glaucoma surgery on visual acuity, the cases with cataract–glaucoma combined surgery were excluded. In the TE Group, the figures at 1 week to 3 months after surgery reflected a significant decline from the level before surgery (). Since there were no cases with obvious progression of cataract or glaucoma during this period, complications of the surgeries were probably responsible for the reduction of visual acuity. In contrast, visual acuity was stable and no significant decline was observed in the Ex-PRESS Group.
Figure 3 Time-course trends in visual acuity of the Ex-PRESS Group (•) and the conventional trabeculectomy (TE) Group (○) excluding cases with additional cataract surgery.
The number of cases with laser suture lysis was smaller and there were fewer administrations of glaucoma eyedrops in the Ex-PRESS Group (). Progression of visual field defect was observed in one-third of the cases in the TE Group, while no such progression was seen in the Ex-PRESS Group ().
Table 3 Postoperative care and treatment (1 year after surgery)
Table 4 Late postoperative complications (1 year after surgery)
Discussion
This paper is evidently the first report of postoperative results in Asians undergoing filtration surgery using Ex-PRESS. As in previous reports with Western subjects,Citation5–Citation8 this study confirms limited cases of early postoperative complications. One possible explanation of this outcome is that the small internal 50-μm diameter of Ex-PRESS is unlikely to cause hypotony, shallow anterior chambers, or choroidal detachment due to overfiltration. Another is that absence of iridectomy induces hyphema unlikely and results in minor postoperative inflammation. In association with early postoperative complications, it is notable that the IOP variations among individual eyes on the day following the surgery were clearly narrower than with conventional trabeculectomy and that there were obviously a small number of cases with a substantial fall in visual acuity among those when Ex-PRESS was used. In the traditional trabeculectomy, it was difficult to predict filtration volume. As a result, hypotony and choroidal detachment occurred more often in the traditional trab-eculectomy, inducing significant reduction in visual acuity or progression of visual field defect (36%, as the rate of progression was rather high in TE Group, but it might probably be because the stages of those patients were rather advanced). The filtration surgery using the Ex-PRESS, however, is highly desirable in terms of safety since the filtration volume through the device is not so varied as the traditional trabeculectomy at least in the early stage after surgery.
Laser suture lysis was required in only few cases in the filtration surgery using the Ex-PRESS as a postoperative treatment, because it required a limited number of sutures for sewing scleral valves since, as discussed above, excessive filtration volume is unlikely. However, further studies may be required on the number of sutures for the scleral flap.
The effect of lowering IOP in the Ex-PRESS surgery was not significantly different from that of conventional tra-beculectomy over 12 months. However, there tended to be a higher success rate and fewer postoperative administrations of glaucoma eyedrops than with trabeculectomy. Taking together, the approach using the Ex-PRESS may be slightly superior in lowering IOP. Previous reports on the analysis of Western subjects states that the Ex-PRESS Group showed better results,Citation7 while another paper reports comparable results between the two groups.Citation6 Future studies need to be conducted with more Japanese subjects. The present study used the Ex-PRESS P-50 model with a 50-μm internal diameter for all cases. The effect of the P-200 model, with a larger internal diameter of 200 μm, could be open to future studies.
Disclosure
The authors report no conflicts of interest in this work.
References
- WamsleySMosterMRRaiSAlvimHSFontanarosaJResults of the use of the Ex-PRESS miniature glaucoma implant in technically challenging, advanced glaucoma cases: a clinical pilot studyAm J Ophthalmol200413861049105115629303
- TavolatoMBabighianSGalanASpontaneous extrusion of a stainless steel glaucoma drainage implant (Ex-PRESS)Eur J Ophthalmol200616575375517061230
- StewartRMDiamondJGAshmoreEDAyyalaRSComplications following Ex-PRESS glaucoma shunt implantationAm J Ophthalmol2005140234034116086969
- RivierDRoySMermoudAEx-PRESS R-50 miniature glaucoma implant insertion under the conjunctiva combined with cataract extractionJ Cataract Refract Surg200733111946195217964403
- DahanECarmichaelTRImplantation of a miniature glaucoma device under a scleral flapJ Glaucoma20051429810215741808
- MarisPJJrIshidaKNetlandPAComparison of trabeculectomy with Ex-PRESS miniature glaucoma device implanted under scleral flapJ Glaucoma2007161141917224744
- De JongLAThe Ex-PRESS glaucoma shunt versus trabeculectomy in open-angle glaucoma: a prospective randomized studyAdv Ther200926333634519337705
- TraversoCEDeFeoFMessas-KaplanALong term effect on IOP of a stainless steel glaucoma drainage implant (Ex-PRESS) in combined surgery with phacoemulsificationBr J Ophthalmol200589442542915774918
- GreveELLangerhorstCTvan den BergTTJPPerimetry and other visual function tests in glaucomaCairnsJEGlaucoma13777London, UKGrune and Stratton1986