Abstract
Background:
This study analyzes the characteristics of donor and recipient tissue preparation between the Hessburg-Barron and Hanna punch and trephine systems by using elliptical curve fitting models, light microscopy, and anterior segment optical coherence tomography (AS-OCT).
Methods:
Eight millimeter Hessburg-Barron and Hanna vacuum trephines and punches were used on six cadaver globes and six corneal-scleral rims, respectively. Eccentricity data were generated using measurements from photographs of the corneal buttons and were used to generate an elliptical curve fit to calculate properties of the corneal button. The trephination angle and punch angle were measured by digital protractor software from light microscopy and AS-OCT images to evaluate the consistency with which each device cuts the cornea.
Results:
The Hanna trephine showed a trend towards producing a more circular recipient button than the Barron trephine (ratio of major axis to minor axis), ie, 1.059 ± 0.041 versus 1.110 ± 0.027 (P = 0.147) and the Hanna punch showed a trend towards producing a more circular donor cut than the Barron punch, ie, 1.021 ± 0.022 versus 1.046 ± 0.039 (P = 0.445). The Hanna trephine was demonstrated to have a more consistent trephination angle than the Barron trephine when assessing light microscopy images, ie, ±14.39° (95% confidence interval [CI] 111.9–157.7) versus ±19.38° (95% CI 101.9–150.2, P = 0.492) and OCT images, ie, ±8.08° (95% CI 106.2–123.3) versus ±11.16° (95% CI 109.3–132.6, P = 0.306). The angle created by the Hanna punch had less variability than the Barron punch from both the light microscopy, ie, ±4.81° (95% CI 101.6–113.9) versus ±11.28° (95% CI 84.5–120.6, P = 0.295) and AS-OCT imaging, ie, ±9.96° (95% CI 95.7–116.4) versus ±14.02° (95% CI 91.8–123.7, P = 0.825). Statistical significance was not achieved.
Conclusion:
The Hanna trephine and punch may be more accurate and consistent in cutting corneal buttons than the Hessburg-Barron trephine and punch when evaluated using elliptical curve fitting models, light microscopy, and AS-OCT.
Introduction
Penetrating keratoplasty is a widely used procedure for the treatment of corneal disease. However, predicting refractive outcome with penetrating keratoplasty is challenging due to the high and irregular astigmatism.Citation1 Mean postoperative astigmatism is 2.5–5.0 diopters, and is thought to be due to imprecise trephination or a size difference of undercut or overcut tissue.Citation2 Disparity between donor and recipient tissue margins is one of the greatest contributors to postoperative astigmatism.Citation3 Other factors that alter postoperative corneal curvature include trephine technique and suture technique.Citation1 Previous studies have evaluated discrepancies in size between epithelial and endothelial openings, corneal button shape, and the angle formed by the trephinated surface of the button by data collected from 35 mm camera photography.Citation4 This current study describes the characteristics of donor and recipient tissue preparation using the Hessburg-Barron (Katena Products Inc, Denville, NJ) and Hanna (Moria Surgical, Antony, France) punch and trephine systems by elliptical curve fitting models, light microscopy, and anterior segment optical coherence tomography (AS-OCT).
Materials and methods
Eight millimeter Hessburg-Barron and Hanna vacuum trephines and punches were used on six cadaver globes and six corneal-scleral rims, respectively. Tissue was donated from the Utah Lions Eye Bank, Salt Lake City, UT. The globes were thawed to room temperature and secured in a Styrofoam mannequin orbit. Balanced Saline Solution (Alcon, Fort Worth, TX) using a 27-gauge needle and 3 cc syringe was injected into the posterior chamber to create an intraocular pressure of 40 ± 3 mmHg. A new trephine was used for each globe, which was trephinated or punched by the same operator. The vacuum trephine was centered on the cornea and trephination proceeded until egress of anterior chamber fluid. The circumferential cut was completed with corneal scissors under a surgical microscope. Eccentricity measurements were performed on the trephinated and punched buttons. AS-OCT (Visante, Zeiss, Jena, Germany) imaging followed by light microscopy evaluation with hematoxylin and eosin staining was performed on the buttons and corneal-scleral rims.
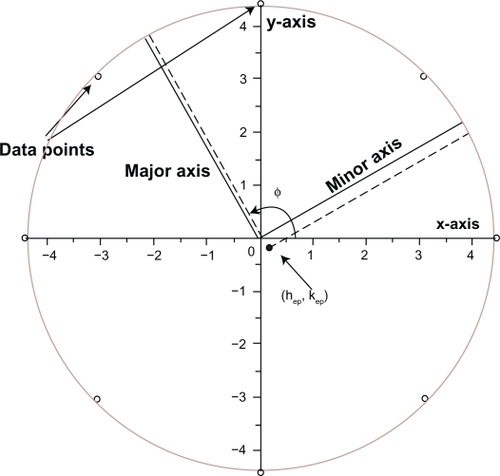
Data were generated using measurements taken from photos of the corneal buttons. Measurements were made of the length of corneal button at four axes, ie, 0–180°, 45–225°, 90–270°, and 135–315°. Data were centered at (0, 0) on a Cartesian coordinate system, and eight data points were generated for the bounds of the corneal button. These data points were used to generate an elliptical curve fit using mathematics based on the work of Fitzgibbon et al.Citation5 This method produces an ellipse-specific, direct solution to a least squares fit, which minimizes the sum of the squares of the distance between the data points and the generated ellipse. The ratio of the length of the major and minor axes was calculated from the equation of the ellipse. This ratio mathematically characterized the amount of deviation from a perfect circle for each corneal button (). In the case of a circle, the ratio of the axes is equal to 1 and any deviation from 1 represents an elliptical cut.
Figure 1 Example of raw data points and measurements of the major and minor axes. The corneal button was centered at (0, 0), represented as (hep, kep) in the Fitzgibbon equations,Citation5 on a Cartesian coordinate system, and eight data points were generated for the perimeter of the corneal button. These data points were used to generate an elliptical curve fit, and ratios of the major and minor axes were calculated.
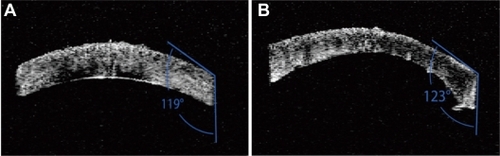
The trephination and punch angle made between the corneal surface and the cut created by the trephine or punch was measured by digital protractor software (AutoCAD 2008, Autodesk, San Rafael, CA) to evaluate the consistency with which each device cuts the cornea (). The digital protractor measurements were made from the light microscopy and AS-OCT images; two light microscopy images and two AS-OCT images per corneal button were used for measurement. Ninety-five percent confidence intervals (CI) and standard deviations were calculated from the data to evaluate the precision of the trephination and punch angles between devices. To standardize the measurement technique between corneal buttons with regular and irregular stromal edges, the vertex of the protractor was placed on the edge of epithelium, and the vertical ray transected the edge of the endothelium.
Figure 2 Example of punch angles measured by the digital protractor software on corneal donor buttons by (A) Hanna punch and (B) Barron punch.
Results
In all three recipient corneas cut by the Barron trephine, the trephine perforated the anterior chamber unequally, and nine clock hours of attached tissue had to be removed with corneal scissors. The Hanna trephine, on the other hand, evenly cut the corneas. Almost all clock hours of the anterior chamber were simultaneously penetrated, leaving one clock hour of tissue to remove with scissors.
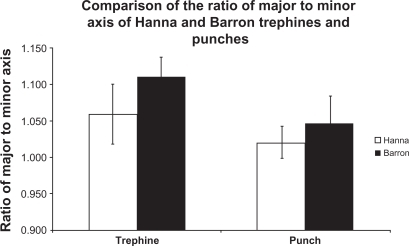
On examination of the trephinated and punched tissue, the ratio of major axis length to minor axis length was considered because it provides a more intuitive comparison than ellipticity, which varies nonlinearly from 1 to infinity. The Hanna trephine had a trend towards producing a more circular recipient button than the Barron trephine (1.059 ± 0.041 versus 1.110 ± 0.027, P = 0.147) and the Hanna punch had a trend towards producing a more circular donor cut than the Barron punch (1.021 ± 0.022 versus 1.046 ± 0.039, P = 0.445, ).
Figure 3 Comparison of the ratio of major to minor axis. (A) Comparison of Hanna trephine and Barron trephine (n = 3). (B) Comparison of Hanna punch and Barron punch (n = 3).
The Hanna trephine demonstrated a trend towards a more consistent trephination angle than the Barron trephine when assessing light microscopy images, ie, ±14.39° (95% CI 111.9–157.7) versus ±19.38° (95% CI 101.9–150.2), P = 0.492, ). Similar results were found between the Hanna and Barron trephine when the OCT images were evaluated, ie, ±8.08° (95% CI 106.2–123.3) versus ±11.16° (95% CI 109.3–132.6, P = 0.306). The punch angle created by the Hanna punch was shown to have less variability than the Barron punch from both light microscopy and AS-OCT imaging, ie, ±4.81° (95% CI 101.6–113.9), versus ±11.28° (95% CI 84.5–120.6, P = 0.295) and ±9.96° (95% CI 95.7–116.4) versus ±14.02° (95% CI 91.8–123.7, P = 0.825, respectively). Although the Hanna trephine and punch were demonstrated to have a more consistent trephination or punch angle than the Barron devices, due to the limited sample size, these differences in consistency were not found to be statistically significant.
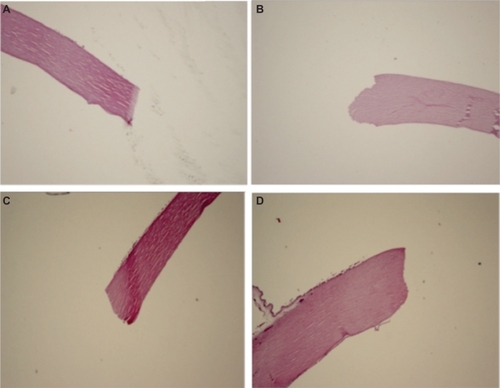
Figure 4 Light microscopy of corneal recipient rims created by (A) Hanna trephine and (B) Barron trephine. Corneal donor buttons cut by (C) Hanna punch and (D) Barron punch as seen by light microscopy. Note the uniform trephination cut on the rim made by the Hanna trephine compared with the irregular cut made by the Barron trephine.
Discussion
In a previous study comparing suction-fixated guided trephines with posterior punch techniques, the suction-fixated guided trephine resulted in significantly greater fibrillar disorder and stromal widening but less endothelial cell loss compared with the posterior punch trephine.Citation6 The authors proposed that the disordered fibrils allow for stronger scar formation during healing.Citation6 There are a wide variety of trephine types, but suction trephination systems are considered technically reliable and easy to use. In theory, they are the safest trephines because of independent stabilization and enhanced blade control.
Wilbanks et al investigated 124 eyes from 98 penetrating keratoplasty patients retrospectively and showed improvement in best-corrected visual outcome with the Hanna trephine compared with the Barron technique, but no difference in postoperative keratometric or refractive astigmatism.Citation6 This study also found a trend toward greater graft rejection in the Barron group, which was proposed to be due to sites of surgical imperfections.Citation6 Another study by van Rij and Waring looked at 12 trephination techniques with five different trephines in 60 human cadaver eyes.Citation4 They showed that the most uniform openings were created with the Hanna followed by a freestanding disposable trephine blade without a handle.Citation4 In this study, 35 mm camera photography was used to evaluate the difference in size between epithelial and endothelial openings, ovalness of the sides, and the angle formed by the trephinated surface of the button.Citation4 Our study supports and augments these findings by demonstrating the uniform cuts of the Hanna with AS-OCT () and light microscopy.
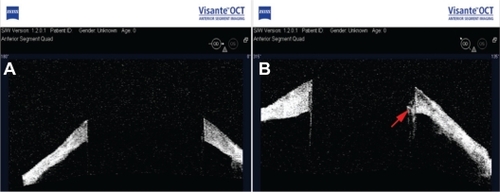
Figure 5 Anterior segment optical coherence tomography of a corneal recipient rim created by (A) Hanna trephine and (B) Barron trephine. Note the regularity of the trephinated surfaces and angles on the recipient rim made by the Hanna trephine. Remnant of corneal tissue (arrow).
Light microscopy and anterior segment OCT have not previously been used to evaluate tissue preparation by Hanna and Hessburg-Barron punch and trephine systems. These modalities have some advantages over using traditional photography. Microscopic analysis and staining allows for detailed examination of the cut surfaces and discrimination between corneal tissue layers. AS-OCT permits cross-sectional analysis of intact corneal buttons across many tissue planes. Data generated from these two imaging methods support prior results by showing a trend for greater precision with the Hanna trephine and punch systems.
Calculating the eccentricity, lengths of the major and minor axes and angles of the tissue buttons revealed a trend for the Hanna to produce more circular and less eccentric buttons than the Barron trephine. The accuracy and precision of the corneal button shape and trephination angle made by the Hanna trephine may be attributed to its greater success in completely entering the anterior chamber compared with the Barron trephine. The Hanna’s decreased need for scissors to complete the cut in our study may be one explanation for this system’s accuracy and precision. These differences between the Hanna and Barron may also represent possible underlying differences in the blades, stability of the tissue, and creation of a vacuum.
This study is limited by the small number of cadaver globes and corneal-scleral rims used, which prevented statistical significance from being achieved. Tissue factors such as corneal thickness, corneal edema, and pre-existing astigmatism were not evaluated, which may have some impact in the formation of a circular corneal donor button. However, these tissue factors can be controlled and monitored in an eye bank setting and will be included in the experimental design of a future study.
In conclusion, the Hanna trephine and punch may be more accurate and consistent in cutting corneal donor buttons than the Hessburg-Barron trephine and punch when evaluated with elliptical curve fitting models, light microscopy, and anterior segment OCT. The greater accuracy and precision of the Hanna devices support the improved visual outcomes and lower rates of graft rejection that has been described in patients who have received penetrating keratoplasty.Citation6
Acknowledgements
Funding for this work was received from the Research to Prevent Blindness Foundation, New York, NY.
Disclosure
The authors report no conflicts of interest in this work.
References
- WiffenSJMaguireLJBourneWMKeratometric results of penetrating keratoplasty with the Hessburg-Barron and Hanna trephine systems using a standard double-running suture techniqueCornea1997163063139143803
- RadnerWSkorpikCHLoeweRMudrichCRadnerGMallingerREffect of trephination technique on the ultrastructure of corneal transplants: Guided trephine system vs posterior punch techniqueBr J Ophthalmol1999831172117710502581
- SpadeaLBiancoGMastrofiniMCBalestrazziEPenetrating keratoplasty with donor and recipient corneas of the same diameterOphthalmic Surg Lasers1996274254308782254
- Van RijGWaringGOConfiguration of corneal trephine opening using 5 different trephines in human donor eyesArch Ophthalmol1988106122812333415548
- FitzgibbonAPiluMFisherRBDirect least squares fitting of ellipsesIEEE Trans Pattern Anal Mach Intell199921476480
- WilbanksGACohenSChipmanMRootmanDSClinical outcomes following penetrating keratoplasty using the Barron-Hessburg and Hanna corneal trephination systemsCornea1996155895988899271