Abstract
Purpose
To determine the effectiveness and possible side effects of using propranolol for the treatment of orbital and periorbital infantile hemangiomas.
Methods
Infants with periorbital or orbital hemangiomas who had not received either local or systemic corticosteroids were recruited. The changes in tumor size, color, and texture, and any side effects of the drug were recorded.
Results
Fifteen infants with a mean age of 8.13 ± 4.7 months were treated according to the set protocol. A change in the color and texture of the hemangioma occurred in the first week following treatment. Mean duration of treatment was 7.67 ± 3.96 months. The size of hemangiomas decreased from a mean of 2.4 ± 0.9 cm to a mean of 1.6 ± 1.0 cm 3 months after treatment (P = 0.001). One patient had to stop the drug because of peripheral vascular ischemia. Another case had the dose reduced to control a mild hyperglycemia. Serious side effects were not observed. A single case of tumor regrowth (8.3%) was recorded.
Conclusion
Treatment of 1–2 mg/kg/day propranolol proved to be effective and associated with minimal side effects. It is likely to replace steroids as the first-line of treatment of hemangiomas in infants.
Introduction
Infantile hemangioma (IH) is the most common pediatric tumor, occurring in 5%–10% of 1-year-old children, with up to 60% presenting in the head and neck region.Citation1 Large hemangiomas can cause amblyopia in up to 60% of cases due to astigmatism or occlusion of the visual axis.Citation2 Various modalities have been employed to induce regression in these lesions, such as laser therapy, cryotherapy, radiotherapy, injection of sclerosing agents, interferon-α, and vincristine,Citation3 but corticosteroids – whether systemic or intralesional – remain the mainstay of treatment of IH.Citation4,Citation5 Systemic side effects of corticosteroids have been observed following systemic as well as intralesional administration and include behavior changes, irritability, insomnia, cushingoid appearance, hypertension, growth deceleration, adrenal suppression, and increased susceptibility to infections.Citation6 Local side effects include eyelid hypopigmentation,Citation7 subcutaneous fat atrophy,Citation8 and eyelid necrosis.Citation9 Intralesional injections have also been reported to cause ophthalmic artery or central retinal artery occlusions.Citation10 In June 2008, Léauté-Labrèze et al reported an accidentally discovered profound regression of a rapidly growing facial hemangioma in a 9-week-old baby following nonselective β-blocker propranolol administration for a cardiac indication.Citation11 Over the last 2 years, most of the studies on this matter were retrospective case reports or case series with limited number of infants included as well as follow-up interval, and some of the cases had already received prior systemic or local corticosteroids at some point. Several important questions remained unanswered. Are these results reproducible? What is the efficacy of the drug? What is the optimal dose, method of initiation, and duration of therapy? What about recurrence and possible side effects? The purpose of the present study was, therefore, to prospectively evaluate the results of this old antihypertensive drug as a new first-line of treatment for IH.
Patients and methods
An interventional prospective case series was conducted between August 2009 and December 2010 after the approval of the local ethics committee and informed consent from the legal guardians of the participants were obtained. Inclusion criteria were infants newly diagnosed of having periorbital or orbital IH, who had not been previously treated with local or systemic corticosteroids. In one case of a deep-seated orbital hemangioma causing proptosis, a biopsy was obtained through an inferior transconjunctival orbitotomy to confirm the diagnosis before being included. Propranolol hydrochloride (PH) was given orally to these infants under the supervision of the pediatrician (RG) according to the hospital’s safety protocol originally designed for other indications of PH administration in infants. Before an infant was given PH, a detailed medical history was taken and a complete ophthalmic examination performed, followed by physical examination and any necessary investigations including blood picture, blood glucose, and electrolytes. Infants with any systemic diseases, especially respiratory or cardiac disease, elevated blood sugar, or other contraindications to β-adrenergic blockers, were not recruited. Patients were hospitalized and a starting dose of 0.16 mg/kg every 8 hours before meals was given under close observation. If the vital signs and glucose levels remained normal, the dose was gradually increased over 2 weeks to 0.67 mg/kg every 8 hours (2 mg/kg/day). The commercially available preparation Inderal® (AstraZeneca plc, London, UK) as a 10 mg tablet was used, crushed and dissolved in 10 cc of distilled water (1 mg/cc). After the final dose of 2 mg/kg/day had been reached (usually within 1–2 weeks), the patient was discharged and instructed to visit the outpatient clinic every 2 weeks initially, during the first 3 months, then every 1–2 months. During these visits, the pediatrician would ask direct questions about the possible adverse effects of PH, such as gastrointestinal or respiratory symptoms; monitor the heart rate, blood pressure, blood glucose, and serum electrolytes; and perform a thorough clinical examination including weighing the infant, and adjusting the dose of PH accordingly. Changes in the tumor in terms of color, texture, or size, and any side effects of the drug were recorded and documented by photograph. A volume estimate of the tumor was determined by taking two maximum orthogonal measurements of the lesion from the axial computed tomography (CT) scans prior to and 3 months after treatment with PH. Subdermal lesions were also measured clinically at each visit. The mean of the higher figure of the two orthogonal measurements was compared prior to, 3, and 6 months after treatment or at the end of therapy if earlier. The treatment was discontinued if the lesion had completely involuted clinically, if the parents decided that the lesion was no longer recognizable and did not want to carry on with taking the medication, or if no further decrease in size was achieved despite continuation of therapy for at least 3 months. PH treatment was tapered gradually over 2 weeks. Patients with large hemangiomas affecting the eyelid were subjected to amblyopia therapy as soon as the visual axis was cleared after prescribing glasses for any considerable refractive errors.
Data was analyzed using SPSS/Win statistical package (v 15; SPSS Inc, Chicago, IL). Numerical data were expressed as mean and standard deviation. For quantitative data, comparison of repeated measures was done using Wilcoxon signed-rank test. A P value <0.05 was considered significant.
Results
Fifteen infants (11 females and 4 males) fit the inclusion criteria and were included in this study; their mean age at presentation was 8.13 ± 4.7 months. With only one case exception, all hemangiomas were subdermal, ie, affecting the upper or lower eyelids or both, including the root of the nose and sometimes with a superficial element (strawberry nevus). In two cases there was an additional involvement of the tip of the nose and the lips with similar lesions. A single case had a deep orbital lesion.
The tumor responded to the drug and decreased in size in all of the cases (100%). A change in color from intense red to purple, associated with a palpable softening of the lesion, was observed as early as 1 week after PH administration ( and ). The visual axis, if initially obliterated, was cleared within a few weeks. The mean size of hemangiomas as measured by CT decreased from 2.4 ± 0.9 cm (range 4.0 × 4.0 cm to 1.0 × 0.5 cm) before treatment to a mean of 1.6 ± 1.0 cm (range 3.0 × 3.0 cm to 0.25 × 0.25 cm) 3 months after PH administration (P = 0.001), and continued to involute resulting in a satisfactory cosmetic result in all except one case which showed an initially huge hemangioma affecting the root of the nose and medial parts of the eyelids and orbit which continued to be disfiguring and surgical resection of the residual lesion was advocated (). On CT, the lesion appeared homogenous, showing intense enhancement with infusion during the pretreatment proliferative phase and later, with involution, it decreased in size and appeared heterogeneous, showing fibrofatty changes ( and ). The mean duration of treatment required was 7.67 ± 3.96 months and the mean follow-up period after propranolol had been stopped was 5.13 ± 3.27 months. No serious adverse effects were observed. An acceptable decrease in heart rate and blood pressure occurred in all patients within the first month (). These were considered secondary circulatory system drug effects rather than complications and did not require the cessation of therapy. Mild hyperglycemia (above 140 mg), confirmed on three occasions, was detected in one patient after 2 months of treatment and resolved by reducing the dose to 1 mg/kg/day. Peripheral vascular ischemic changes in the form of mottling, coldness, and hypoperfusion of the skin of the trunk and lower limbs occurred in another case that had no history of a vascular disease; PH was stopped and these changes resolved completely without sequel (). A single case (8.3%) showed signs of regrowth after 3 months of cessation of therapy: a 12-month-old female who presented with subdermal upper-lid hemangiomas was treated with PH for 11 months. The lesion considerably decreased in size and treatment was terminated upon request of her parents.
Figure 1 A large upper-lid hemangioma prior to and 4 months after treatment.

Figure 2 Multiple facial hemangiomata prior to and 6 months after treatment.

Figure 3 A right upper-lid hemangioma prior to and 3 months after propranolol hydrochloride administration with an evident decrease in size as shown by the axial computed tomography scan with enhancement.

Figure 4 A 2-week-old girl with a right deep orbital hemangioma causing proptosis prior to and 3 months after treatment; computed tomography scan with enhancement shows a change in the size and appearance of the lesion being initially homogenous in the proliferative phase, then becoming heterogenous denoting fibrofatty degeneration when starting involution.
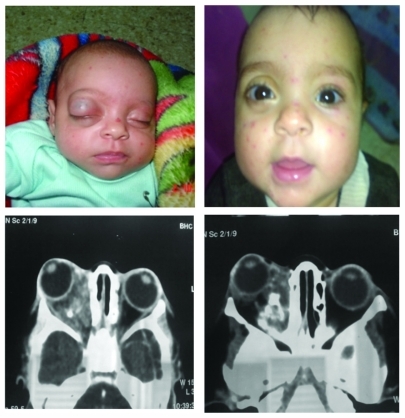
Figure 5 Thigh of a 2-month-old child showing peripheral vascular ischemic changes at 3 weeks from propranolol hydrochloride administration; mottling became more apparent after 4 weeks. These changes were reversible.

Table 1 Changes in size, heart rate, blood pressure, and blood glucose prior to and 3 months after treatment
Discussion
This is one of few prospective studies concerning the use of oral PH for the treatment of IH that was preceded by or accompanied with administration of corticosteroids. No treatment failure was observed in any patients in this study who were able to continue the administration of PH (14 patients). PH proved to be well tolerated, safe, and without considerable complications when used in infants.
All other current drug-based therapeutic options for IH, similar to steroids, have been known to cause serious complications in the pediatric population. Therapy with immunomodulators such as cyclophosphamide or vincristine has been associated with myelosuppression and hepatotoxic effect. Also, serious neurotoxic effects in the form of spastic diplegia in up to 20% of cases were reported when interferon-α2a was used in treatment of IH.Citation12
Recently, new molecular and cellular insights have helped in understanding the pathophysiology of IH. An intrinsic defect in endothelial cells caused by a genetic mutation of the endothelial cell or its progenitor has been suggested;Citation13 another theory involves the hypoxia-inducible factor 1a, a major regulator of cellular response to hypoxia.Citation13 Finally, release of placental cells into the circulation that might embolize to fetal vascular sites has been proposed.Citation14 In favor of this placental hypothesis are the recent reports of increased incidence of IH associated with chorionic villus sampling, but not with amniocentesis,Citation15 and the demonstration that both IH endothelium and placental vessels share the expression of several surface markers as glucose transporter 1, which is not found in other vascular tumors or malformations, nor normal skin.Citation14
The proliferation and involution of hemangiomas are controlled by complex interactions of molecular, cellular, and hormonal regulators. Takahashi et al hypothesized that during the third trimester of fetal development, masses of plump immature endothelial cells coexist with immature pericytes, which maintain their proliferative capacity for a limited period during postnatal life.Citation16 Angiogenic peptides, such as β-fibroblast growth factor, vascular endothelial growth factor, and proliferating cell nuclear antigen, induce proliferation of these immature cells, resulting in the development of the hemangioma. As the endothelial cells differentiate, an influx of mast cells, various myeloid cells, and tissue inhibitors of metalloproteinases occurs. Tissue inhibitors of metalloproteinases, along with interferon and transforming growth factor produced by the mast cells, terminate the endothelial cell proliferation and induce involution by apoptosis of endothelial cells.Citation17
In view of the new theories for pathogenesis, possible explanations for the therapeutic effect of such β-blockers as propranolol on IH may include vasoconstriction due to decreased release of nitric oxide, which results in the early visible change in color and is associated with a palpable softening of the hemangioma.Citation18 Decreased expression of proangiogenic factors like vascular endothelial growth factor and β-fibroblast growth factor may occur through the down regulation of the Raf-mitogen-activated protein kinase pathway,Citation19 matrix metallopeptidase 9 secretion, and human brain microvascular endothelial cells tubulogenesis,Citation20 which explains the progressive improvement of the hemangioma, possibly through the triggering of apoptosis of capillary endothelial cells, which results in further tumor involution.Citation21
Pediatricians recite a long list of possible side effects of β-blockers including fatigue, gastrointestinal upset, nightmares, anxiety, dizziness, and bronchospasm, as well as hyperlipidemia and hyperglycemia. Citation22 Thus, they are relatively contraindicated in children with asthma or diabetes. β-blockers may also predispose young children, especially infants, to hypoglycemia with even masking of the β-sympathetic-related symptoms,Citation23 but this has been reported mainly in circumstances of diminished feeding. This was avoided in the authors’ study by ensuring that children were well fed during drug therapy. The occurrence of a reversible peripheral vascular ischemic-like change that was not linked to any original disease and, therefore, had to be linked to the administration of PH is reported for the first time in this study.
Although partial regrowth of the tumor has been commonly reported with oral corticosteroids,Citation24 to the authors’ knowledge, previous studies have not mentioned the regrowth of the hemangioma after stopping PH except in a single study in which a recurrence of the hemangioma within 8 weeks of stopping the drug was reported in two patients when PH was given for a short duration and was tailed down rapidly.Citation25 In this study, however, a single case (8.3%) showed signs of regrowth of the hemangioma 3 months after PH administration had been stopped. The reason for this was possibly the cessation of therapy while the tumor still had proliferating cells. A longer follow-up period of a greater number of patients treated with PH is needed before reaching a conclusion in this matter.
Conclusion
A PH dose between 1–2 mg/kg/day for 6 to 12 months is both effective and safe for the treatment of IH. However, a collaborative approach with a pediatrician is required. A pretreatment work up and gradual loading and tapering with close monitoring on an outpatient basis during the initial phase of treatment is recommended. The use of PH would be extremely beneficial in multiple and miliary hemangiomatosis and in deep orbital lesions where surgical excision or steroid injections are hazardous. β-blockers may well replace corticosteroids as the first-line of treatment for IH with improved tolerability and side-effect profile. In the future, steroid use can be limited to cases of allergy, resistance, or contraindications to β-blockers.
Acknowledgment
The authors appreciate the consent of the guardians of those cases whose photos were used in this report so as not to mask their features to help show clearly the effect of treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
- PowellJUpdate on hemangiomas and vascular malformationsCurr Opin Pediatr199911545746310555599
- SchwartzSRBleiFCeislerESteeleMFurlanLKodsiSRisk factors for amblyopia in children with capillary hemangiomas of the eyelids and orbitJ AAPOS200610326236816814181
- FriedenIJHaggstromANDroletBAInfantile hemangiomas: current knowledge, future directions. Proceedings of a research workshop on infantile hemangiomas, April 7–9, 2005, Bethesda, Maryland, USAPediatr Dermatol200522538340616190987
- ChowdriNADarziMAFaziliZIqbalSIntralesional corticosteroid therapy for childhood cutaneous hemangiomasAnn Plast Surg199433146517944196
- OrawiecBStefanczykLCzajkowskiJBogorodzkiBGralekMPeriorbital capillary hemangiomas in children–treatment and monitoring of treatmentKlin Oczna1996983217220 Polish9019593
- GeorgeMESharmaVJacobsonJSimonSNopperAJAdverse effects of systemic glucocorticosteroid therapy in infants with hemangiomasArch Dermatol2004140896396915313812
- CogenMSElsasFJEyelid depigmentation following corticosteroid injection for infantile ocular adnexal hemangiomaJ Pediatr Ophthalmol Strabismus198926135382915311
- TownshendLMBuckleyEGLinear subcutaneous fat atrophy after a single corticosteroid injection for ocular adnexal hemangiomaAm J Ophthalmol199010911021032297019
- SutulaFCGloverATEyelid necrosis following intralesional corticosteroid injection for capillary hemangiomaOphthalmic Surg19871821031053574861
- KushnerBJLemkeBNBilateral retinal embolization associated with intralesional corticosteroid injection for capillary hemangioma of infancyJ Pediatr Ophthalmol Strabismus19933063973998120748
- Léauté-LabrèzeCDumas de la RoqueEHubicheTBoraleviFThamboJBTaiebAPropranolol for severe hemangiomas of infancyN Engl J Med2008358242649265118550886
- BarlowCFPriebeCJMullikenJBSpastic diplegia as a complication of interferon alfa-2a treatment of hemangiomas of infancyJ Pediatr19981323 Pt 15275309544915
- RitterMRButschekRAFriedlanderMFriedlanderSFPathogenesis of infantile haemangioma: new molecular and cellular insightsExpert Rev Mol Med200793211918045510
- NorthPEWanerMMizerackiAA unique microvascular phenotype shared by juvenile haemangiomas and human placentaArch Dermatol2001137555957011346333
- BurtonBKSchulzCJAngleBBurdLIAn increased incidence of hemangiomas in infants born following chorionic villous sampling (CVS)Prenat Diagn19951532092147784377
- TakahashiKMullikenJBKozakewichHPRogersRAFolkmanJEzekowitzRACellular markers that distinguish the phases of hemangioma during infancy and childhoodJ Clin Invest1994936235723647911127
- RitterMRReinischJFriedlanderSFFriedlanderMMyeloid cells in infantile hemangiomaAm J Pathol2006168262162816436675
- ShyuKGLiouJYWangBWFangWJChangHCarvedilol prevents cardiac hypertrophy and overexpression of hypoxia-inducible factor-1 and vascular endothelial growth factor in pressure-overloaded rat heartJ Biomed Sci200512240942015942707
- D’AngeloGLeeHWeinerRIcAMP-dependent protein kinase inhibits the mitogenic action of vascular endothelial growth factor and fibroblast growth factor in capillary endothelial cells by blocking Raf activationJ Cell Biochem19976733533669361190
- AnnabiBLachambreMPPlouffeKMoumdjianRBeliveauRPropranolol adrenergic blockade inhibits human brain endothelial cells tubulogenesis and matrix metalloproteinase-9 secretionPharmacol Res2009605438445 El-Essawy et al19467330
- Sommers SmithSKSmithDMBeta blockade induces apoptosis in cultured capillary endothelial cellsIn Vitro Cell Dev Biol Anim200238529830412418927
- WiysongeCBradleyHMayosiBBeta-blockers for hypertensionCochrane Database Syst Rev20071CD00200317253471
- ChavezHOzolinsDLosekJDHypoglycemia and propranolol in pediatric behavioral disordersPediatrics19991036 Pt 11290129210353945
- AbryFKehrliPSpeeg-SchatzCHemangioma of the eyelids and orbit in children: therapeutic follow-upJ Fr Ophthalmol2007302170176 French
- ChikKKLukCKChanHBTanHYUse of propranolol in infantile haemangioma among Chinese childrenHong Kong Med J201016534134620889997