Abstract
Selective intra-arterial chemotherapy (IAC) has been adopted by many ocular oncology centers to treat advanced intraocular retinoblastoma. In this report, we describe two patients with unilateral intraocular retinoblastoma and persistent vitreous seeding, who were treated with IAC after failed systemic chemotherapy. Despite multiple sessions and increasing dosage of drug delivery, vitreous seeding in these cases failed to respond to IAC, and ultimately both eyes were enucleated for tumor control. Based on the histopathologic findings in these two cases, IAC appears to have limitations in treating persistent vitreous seeding in eyes which have failed systemic chemotherapy. Possible causes for failure of IAC to treat persistent vitreous seeding include poor vitreous penetration, inactive state of tumor seeds within the avascular vitreous cavity, and chemotherapeutic drug resistance.
Introduction
Intra-arterial infusion of chemotherapy (IAC) has been recognized as a viable new method for treating advanced intraocular retinoblastoma.Citation1–Citation4 When compared to intravenous chemotherapy, potential advantages of selective IAC include the reduction of systemic effects such as myelosuppression, immunosuppression and the risk of secondary leukemia.Citation5 Compared to external beam radiation, IAC can be used to treat children below age 12 months without concerns regarding local side effects such as orbital hypoplasia and the risk of secondary head and neck cancers later in life.Citation6 Gobin et al have demonstrated globe salvage rates as high as 82% with IAC in primary cases with advanced intraocular tumors.Citation2 In this report, we describe two patients with unilateral intraocular retinoblastoma and persistent vitreous seeding, who were treated with IAC after failed systemic chemotherapy. Despite multiple sessions and increasing dosage of drug delivery, vitreous seeding in these cases failed to respond to IAC, and ultimately both eyes were enucleated for tumor control.
Case description
Case one
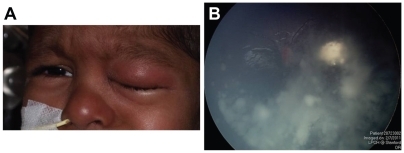
A one-month-old child born three weeks premature was diagnosed with a left retinal tumor during a screening examination. Fundus evaluation revealed a left macular tumor which was whitish in appearance with fine retinal vasculature (). Based on her other clinical findings (symphalangism, pelviectasis, paired ribs, facial dysmorphic features), she was diagnosed with unilateral retinoblastoma in the setting of 13q deletion syndrome. The left eye was classified as having a Group C tumor based on the macular location and the presence of localized seeding. She received three sessions of systemic chemotherapy using a three drug regimen (carboplatin, etoposide, vincristine), with excellent clinical regression of the tumor (). There was complete calcification of the tumor, and it was decided to carefully observe the patient rather than perform laser treatment due to its macular location. The patient was then lost to follow-up when her family took her to India for approximately 9 months. When she finally returned to our institution, a tumor recurrence along the temporal edge of the macular scar was noted. There was also diffuse vitreous seeding arising from this area of tumor recurrence (). The patient was treated with two additional courses of systemic chemotherapy (topotecan and cyclophosphamide) with excellent regression of the retinal tumor recurrence, but there was no response by the vitreous seeding (). The patient was then treated with two sessions of IAC; the first with 5 mg of melphalan and the second (1 month later) with 8 mg of melphalan. After the second session of IAC, the patient developed diffuse periocular edema (), which resolved within 1 week. Unfortunately, the vitreous seeding appeared to increase in severity (), and the left eye was enucleated to prevent tumor spread, approximately 2 1/2 years after initial diagnosis.
Figure 1 (A) One-month-old child with unilateral retinoblastoma and a left macular tumor. (B) Excellent regression of the tumor after three sessions of systemic chemotherapy, causing complete calcification of the macular lesion. (C) Tumor recurrence along temporal edge of the tumor, with associated vitreous seeding. (D) Excellent regression of the retinal tumor recurrence but no response by vitreous seeding after systemic chemotherapy.
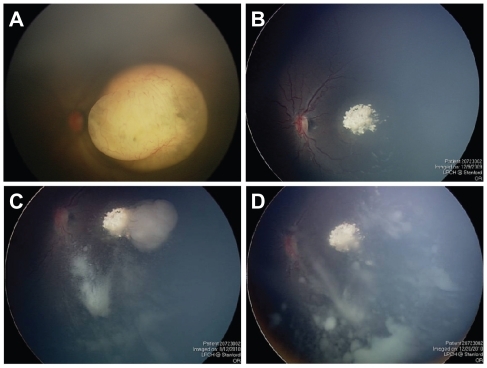
Figure 2 (A) Diffuse periocular edema following intra-arterial infusion of melphalan, which resolved without sequelae. (B) Fundus photograph showing progression of vitreous seeding despite two sessions of intra-arterial chemotherapy.
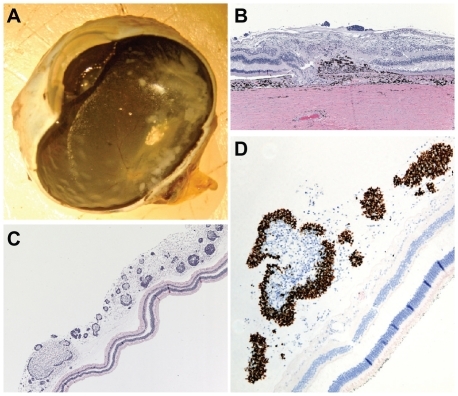
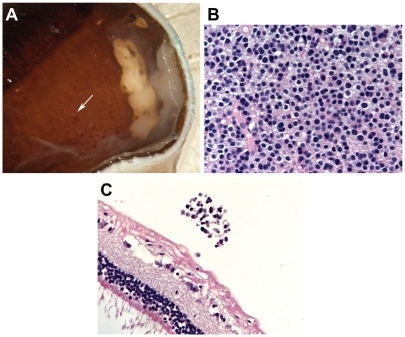
Gross examination of the sectioned enucleated eye showed extensive tumor seeding within the vitreous cavity (). Histopathologic examination showed complete regression and calcification of the macular tumor. (). The tumor was replaced by a scar comprising glial cells and retinal pigment epithelial proliferation. Bruch’s membrane was broken and a portion of the retina had shifted through this break into the choroid. Numerous tumor seeds were seen lying on the internal limiting membrane (), but the retina away from the macular scar was otherwise normal in appearance. The vitreous contained numerous tumor nodules of small, basophilic cells with a high nuclear to cytoplasmic ratio. The diffuse vitreous seeding demonstrated 80% positive staining with Ki67 (), an immunohistochemistry marker for cellular proliferation.Citation7 No histopathologic abnormalities were noted within the cornea, iris, choroid, sclera or optic nerve (data not shown).
Figure 3 (A) Gross photograph of enucleated eye showing a calcific scar of the regressed macular retinoblastoma and extensive vitreous seeding. (B) Section through the macula with the optic nerve to the right of the photograph. Macular scar in area without calcification; the scar consists of glial cell proliferation and retinal pigment epithelium hyperplasia. In addition, a portion of the retina has shifted into the choroid through a break in Bruch’s membrane (hematoxylin-eosin, original magnification 100×). (C) Temporal, equatorial retina with numerous tumor seeds (basophilic cells, see arrow) in the overlying vitreous (hematoxylin-eosin, original magnification 100×). (D) Vitreous seeds with markedly positive nuclear reaction to Ki67 (original magnification 200×).
Case two
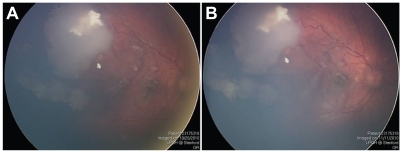
A four-year-old boy was referred with persistent unilateral retinoblastoma involving the right eye after systemic chemotherapy. The patient had received five total courses of systemic chemotherapy at another institution; the first three courses with vincristine, etoposide, and carboplatin, and the final two courses with topotecan and cyclophosphamide. The patient had no family history of retinoblastoma and his past medical history was otherwise negative. The patient’s vision measured 20/30 OD and 20/15 OS. Fundus examination revealed a partially regressed supero-temporal tumor, with multiple vitreous seeds overlying the macula (). He was treated with three sessions of IAC; the first with 5 mg of melphalan, the second with 8 mg of melphalan, and the third with 4 mg of melphalan and 30 mg of carboplatin. After the first IAC infusion, his white blood cell count decreased from 5600 to 3700 but he did not require admission. Visual acuity after the IAC infusions ranged between 20/30–20/50 in the right eye. Examination under anesthesia after the third session of IAC showed a slight increase in the vitreous seeding, and no response by the main tumor mass (). Five months following the initial IAC infusion, enucleation was performed due to concerns regarding the persistently active tumor.
Figure 4 (A) Fundus photograph of the right eye showing partially regressed superotemporal tumor and vitreous seeds overlying the macula. (B) Same view of right fundus showing no regression of the vitreous seeds despite three sessions of intra-arterial chemotherapy.
Gross evaluation of the sectioned enucleated eye revealed a 5 × 5 mm mass superotemporally on the retina with calcifications (). The mass was differentiated, containing cells with small bland nuclei and relatively abundant eosinophilic cytoplasm (). No fleurettes, rosettes or mitotic figures were seen. Scattered areas of glial cells were seen adjacent to the tumor and within the tumor. Occasional vitreous seeds were found in the vitreous near the retina. The retina otherwise appeared normal in all quadrants. The immunohistochemical stain for Ki-67, a cellular proliferation marker, revealed no positive reactions in either the main tumor or the vitreous seeds, consistent with their differentiated appearance ().
Figure 5 (A) Gross photograph of enucleated eye showing main superotemporal tumor and vitreous seeds overlying the macula (arrow). (B) The main tumor consisting of well-differentiated cells with abundant cytoplasm (hematoxylin-eosin, original magnification 400×). (C) A vitreous seed containing differentiated cells, with negative staining with Ki67 (hematoxylin-eosin, original magnification 400×).
Comment
Selective intra-arterial chemotherapy (IAC) has been adopted by many ocular oncology centers to treat advanced intraocular retinoblastoma.Citation1–Citation4 In some centers, IAC has become the primary modality for treating advanced tumors, while in other institutions IAC is used mainly as salvage therapy after failed systemic chemotherapy and/or radiation.Citation2,Citation3 The ocular effects of directly infusing the ophthalmic artery with chemotherapy agents are still being studied. Local transient side effects have been reported including peri-orbital swelling and erythema, temporary eyelash loss and more rarely, retinal arterial occlusion.Citation8–Citation10 Brodie and colleagues have demonstrated through electrophysiologic testing that some eyes after IAC have preserved and even improved ERG readings.Citation11 However, Vajzovic et al reported retinopathy and vitreous hemorrhage in three of their first eleven eyes treated at the University of Miami.Citation3,Citation9 There has also been a recent report of choroidal artery occlusion and retinal emboli formation following IAC.Citation10
We report two children with intraocular retinoblastoma who underwent enucleation following failed systemic chemotherapy and multiple infusions with IAC. In the original series of nine patients reported by Abramson, the two eyes enucleated after IAC did not show evidence of ocular toxicity. Citation1 A histopathologic report from Vajzovic and colleagues showed no evidence of toxicity to the retina, optic nerve, choroid or vascular structures.Citation12 Graeber and colleagues recently reported pathologic findings in ten eyes that were enucleated for tumor growth after IAC.Citation13 They also did not identify any specific evidence of ocular toxicity attributed to IAC, although nine of the ten eyes had received prior multimodal treatment such as external beam radiotherapy and laser therapy. In our two cases, there was no previous history of any local therapy being delivered to the globes. The two eyes were treated with doses of melphalan as high as 8 mg, utilizing an infusion technique identical to the one described by Abramson and colleagues.Citation1 There was no evidence of ocular toxicity on histopathologic examination, as evidenced by the lack of degeneration of the retina and optic nerve in areas uninvolved by tumor. Although electrophysiologic testing was not performed, the older patient in our case series demonstrated fairly well-preserved visual acuity after all three of his IAC infusions. Based on the limited evidence to date, it does not appear that IAC causes anatomic damage to the globe in the absence of a retinal occlusive event.
In both of our cases, vitreous seeding did not respond to treatment with IAC, despite escalating doses of melphalan (cases one and two) and even multiple drug combinations (case two). We used doses of melphalan as high as 8 mg per treatment in our two cases, which is slightly higher than the 7.5 mg dose reported by both Gobin et and Vajzovic.Citation2,Citation12 Both patients developed temporary side effects following IAC (periocular edema, neutropenia), but the vitreous seeding persisted and even continued to progress. It is noteworthy that all three of the eyes reported by Vajzovic et al which were removed for poor response after systemic chemotherapy and salvage IAC also had vitreous seeding.Citation12 Based on a limited number of cases to date, IAC appears to have limitations in treating persistent vitreous seeding in eyes which have failed systemic chemotherapy. Possible causes for failure of IAC to treat persistent vitreous seeding include poor vitreous penetration, inactive state of tumor seeds within the avascular vitreous cavity, and chemotherapeutic drug resistance. The decision to use IAC for any eye with retinoblastoma must be individualized based on several factors including unilateral or bilateral tumor involvement, the availability of other treatment options, and whether the eye has significant visual potential. For a patient with unilateral retinoblastoma and recalcitrant vitreous seeding after systemic chemotherapy, multiple sessions of IAC with escalating doses of melphalan may not be advisable given that enucleation is typically curative in these cases.
Disclosure
The authors have no financial or other conflict of interest which may arise from the publication of this manuscript.
References
- AbramsonDHDunkelIJBrodieSEKimJWGobinYPA phase I/II study of direct intraarterial (ophthalmic artery) chemotherapy with melphalan for intraocular retinoblastoma initial resultsO–hthalmology2008115813981404
- GobinYPDunkelIJMarrBPBrodieSEAbramsonDHIntra-arterial chemotherapy for the management of retinoblastoma: Four-year experienceArch Ophthalmol2011129673273721320950
- PetersonECElhammadyMSQuintero-WolfeSMurrayTGAziz-SultanMASelective ophthalmic artery infusion of chemotherapy for advanced intraocular retinoblastoma: initial experience with 17 tumorsJ Neurosurg201111461603160821294621
- ShieldsCLRamasubramanianARosenwasserRShieldsJASuperselective catheterization of the ophthalmic artery for intraarterial chemotherapy for retinoblastomaRetina20092981207120919734768
- GombosDSHungerfordJAbramsonDHSecondary acute myelogenous leukemia in patients with retinoblastoma: Is chemotherapy a factor?Ophthalmology200711471378138317613328
- AbramsonDHFrankCMSecond nonocular tumors in survivors of bilateral retinoblastoma: a possible age effect on radiation-related riskOphthalmology199810545735799544627
- GerdesJSchwabULemkeHSteinHProduction of a mouse monoclonal antibody reactive with a human nuclear antigen associated with cell proliferationInt J Cancer198331113206339421
- MarrBGobinPYDunkelIJBrodieSEAbramsonDHSpontaneously resolving periocular erythema and ciliary madarosis following intraarterial chemotherapy for retinoblastomaMiddle East Afr J Ophthalmol201017320720920844675
- VajzovicLMMurrayTGAziz-SultanMASupraselective intraarterial chemotherapy: Evaluation of treatment-related complications in advanced retinoblastomaClin Ophthalmol2011517117621383945
- MunierFLBeck-PopovicMBalmerAGaillardMCBoveyEBinaghiSOccurrence of sectoral choroidal occlusive vasculopathy and retinal arteriolar embolization after superselective ophthalmic artery chemotherapy for advanced intraocular retinoblastomaRetina201131356657321273941
- BrodieSEPierre GobinYDunkelIJKimJWAbramsonDHPersistence of retinal function after selective ophthalmic artery chemotherapy infusion for retinoblastomaDoc Ophthalmol20091191132219169884
- VajzovicLMMurrayTGAziz-SultanMAClinicopathologic review of enucleated eyes after intra-arterial chemotherapy with melphalan for advanced retinoblastomaArch Ophthalmol2010128121619162321149791
- GraeberCPGobinYPMarrBPHistopathologic findings of eyes enucleated after treatment with chemosurgery for retinoblastomaOpen Ophthalmol J201151521399766