Abstract
Purpose
Coffee and tea are very common nonalcoholic beverages. However, their intake, particularly that of coffee, has been suggested to increase intraocular pressure (IOP) in patients with open angle glaucoma/ocular hypertension. The causative agent has been suggested to be their caffeine content. The objective of this study was to determine if this represents a direct caffeine effect. This study was therefore done using pure caffeine applied directly to the eyes.
Methods
The study was conducted with five human volunteers with open angle glaucoma/ ocular hypertension. IOP was measured using a Perkins applanation tonometer. Eye drops of 1% caffeine were prepared in-home. Following the initial (basal) measurement of the IOP, 50 μL of the eye drop preparation was instilled in the eye at 0-, 4-, and 6-hour intervals. IOPs were measured 30 minutes after each instillation. A second study was also undertaken following the first. In this study, the same patients instilled the eye drops three times per day for 1 week at home and then returned to the clinic on day 7. They were then again treated with caffeine eye drops as above and IOPs measured.
Results
In the 1-day study, the mean basal IOP was 23.6 ± 2.80 mmHg. Thirty minutes after instillation of the drops as described, the pressures were 23.2 ± 1.93, 22.2 ± 1.99, and 22.6 ± 2.31. The basal reading was taken at 10 am and another reading was then taken at 10.30 am. Additional eye drops were instilled at 2 and 8 pm and readings taken 30 minutes after each instillation. In the 1 week study, the basal value was 22.6 ± 2.32. After instillation of the drops as above the values were 23 ± 2.16, 22.4 ± 2.27, and 23 ± 1.94.
Conclusion
Administration of caffeine into the eyes of patients did not have any effect on IOP and it remained relatively unchanged. This was true in the 1-day study as well as in the 1-week study. A cumulative effect was not visible. The results therefore demonstrate that caffeine has no significant effect on IOP in patients with glaucoma. Any effects reported in coffee drinkers may therefore be related to other constituents in coffee, known to be generated pyrolytically from endogenous constituents of coffee beans by roasting at relatively high temperature, combined with the osmotic effects imposed by adequate fluid intake, known to be common in glaucoma patients.
Introduction
Caffeine (1,3,7-trimethylxanthine) is a significant ingredient in several common beverages such as coffee, tea, and colas, as well as in various other food items such as cakes and candies. A regular cup of coffee (236 mL) contains 135–150 mg of caffeine.Citation1 On average, daily consumption from normal coffee drinking alone is over 200 mg per day, although amounts up to 400 mg per day have been reported from certain European countries.Citation2,Citation3 Such amounts of caffeine are known to exert several physiological effects such as stimulation of the central nervous system (CNS), cardiac excitation, relaxation of bronchial and vascular smooth muscles, and promotion of diuresis and intestinal motility.Citation4,Citation5
Although most of these caffeine effects are ultimately related to its effect of increasing levels of cytosolic calcium ions, the specific mechanisms involved and the magnitude of the physiological effects differ from one tissue to another. Stimulation of the CNS, for example, is attributed to a competitive blockade of the adenosine receptors situated at the presynaptic nerve terminals.Citation6–Citation9 This is due to the structural similarities between adenosine and caffeine, both purine derivatives. Since the binding of adenosine to its receptor regulates the voltage-gated calcium channels, blockade of these receptors results in an increased influx of calcium from the extracellular milieu into the cell cytosol, causing an increase in the synaptic release of neurotransmitters, including acetylcholine, norepinephrine, dopamine, and others involved in neural transduction and cardiovascular stimulation.Citation9–Citation11
The stimulation of cardiac muscle contraction by caffeineCitation12–Citation14 has been attributed to its binding with ryanodine-sensitive Ca++ channels in the sarcoplasmic reticulumCitation15–Citation18 and consequent release of the sequestered Ca++ into the cytosol. In turn, the increased cytosolic Ca++ stimulates muscle contraction via interaction with the actomyosin complex.
The vasodilatory effect of Ca++ is exerted through Ca++-dependent activation of nitric oxide synthase, resulting in the elevation of nitric oxide and cyclic guanosine monophosphate levels.Citation19 Caffeine also has several metabolic effectsCitation20–Citation23 exerted through an inhibition of cyclic adenosine monophosphate (c-AMP) phosphodiesteraseCitation24 leading to an enhancement of c-AMP levels in the cells.
In summary, most of the neural and extraneural effects of caffeine are exerted through its action on intracellular levels of free calcium and inhibition of phosphodiesterase. However, several recent biochemical studies demonstrate that it is also an effective scavenger of reactive oxygen species, including the hydroxyl radical OH•.Citation25–Citation33 The product of such a reaction is the formation of the 8-oxo derivative of caffeine, known as N-trimethyl urate. However, direct generation of OH• in vivo is a rarity. Usually it takes place by the interaction of hydrogen peroxide and superoxide, which by themselves are potent oxidants, detoxified normally by superoxide dismutase, catalase, and glutathione peroxidase. The generation of OH• is hence greatly minimized in most tissues, except in the cases of the eye and the skin where its generation remains consistent via several photochemical reactions.Citation29
Studies on the pathophysiological effects of caffeine in the eye are still very limited. However, coffee drinking has been suggested to cause a transient elevation of intraocular pressure (IOP) in patients with glaucoma. The magnitude of such pressure elevation ranges from 1 to 2 mmHg, an hour after drinking coffee.Citation34–Citation37 The significance of this relatively small elevation in the face of a normal IOP of 14–22 mmHg remains unsure, especially in view of a number of studies that have found no such effect.Citation38–Citation40 In fact, it is well known that such increases can take place just by drinking equivalent amounts of water, ranging from 250 to 1000 mL.Citation41–Citation47 That normal coffee drinking is not associated with an effect on IOP has been shown also by a large cohort study.Citation48 Further, it should be pointed out that coffee is not analogous to caffeine,Citation49 the former being a complex mixture of compounds containing several other physiologically active compounds such as furfurals and acrolein.
Information about the effect of caffeine per se on IOP in patients with glaucoma/ocular hypertension is not yet available, except for one study where oral administration of caffeine was found to be ineffective in raising IOP.Citation50 However, such studies are still lacking in glaucoma patients, who are known to have significant alterations in aqueous dynamics and IOP. The effect of a continued supply of caffeine to the aqueous humor also remains to be studied to determine whether there are any cumulative effects.
A study of the effects of direct topical application of caffeine on IOP in patients with glaucoma was thus desirable, especially in view of the many recent observations strongly suggesting that the compound has significant positive health effects such as the prevention of diseases such as Alzheimer’s and Parkinson’s-like diseases,Citation51–Citation58 and inhibition of the onset of diabetes.Citation59,Citation60 This study was therefore undertaken to determine the effect of caffeine on IOP in patients with glaucoma/ ocular hypertension, using direct topical administration of pure caffeine via eye drops, eliminating the possibility of indirect metabolic effects.
Contrary to expectations based on earlier observations of coffee drinking in relation to IOP in glaucoma patients, the results of this study indicate that direct application of caffeine to the eye does not exert any effect on IOP. This applied both in studies done within hours of caffeine instillation in the eye and when patients were treated consecutively 3 times a day for 6 days followed by another treatment on day 7. The authors’ studies suggest no reason for caution in the use of caffeine in patients with open angle glaucoma, as similar small increases in IOP can be generated by water-drinking as seen in a provocative test for glaucoma. This is attributable to changes in body fluid osmotic dynamics.
Materials and methods
A 1% caffeine eye drop preparation was made by dissolving 100 mg of caffeine (Sigma Aldrich catalogue number 58082; Sigma Aldrich, St Louis, MO) in 10 mL of sterile teardrop solution (0.3% hydroxyl-propyl methyl cellulose) (Sigma Aldrich) at room temperature. The solution was then divided, using sterile techniques, into 1 mL portions in eye drop vials and refrigerated. IOP was determined using a Perkins applanation tonometer (Clement Clarke Perkins MK-II; Clement Clarke International, Harlow, UK) after application of procaine/fluorescein eye drops (Smarth Life Sciences Nalagarh, Solan, Himachal Pradesh, India).
The five volunteers selected for the study were diagnosed to have primary open angle glaucoma/ocular hypertension. The age of the patients varied from 40 to 65 years. The group mean IOP was 23.6 ± 2.8 mmHg. They had not had any ocular surgical procedures such as cataract extraction or laser photocoagulation treatment for retinopathy.
Basal intraocular pressures were taken at 10.00 am and labeled “A.” Immediately following, the caffeine eye drop preparation was instilled (50 μL) and the eye closed for proper mixing of the drop in the conjunctival cul-de-sac. An IOP measurement was then taken at 10.30 am (labeled “B”). Additional eye drops were then instilled in the respective eyes at 2 and 8 pm and IOP measured again 30 minutes after each instillation, that is, at 2.30 (C) and 8.30 pm (D), respectively. Thus, the total number of IOP measurements on each eye was four, including the initial basal reading. Blood pressures were taken at the beginning and at the end of the investigation, with no substantial change revealed. Subsequently, the patients were asked to instill the eye drops three times daily at the above times for 6 days and then return to the clinic on day 7. The above schedule of drop instillation and IOP measurements was then repeated. The patients were then withdrawn from the study and started on antiglaucoma medications.
Results
The initial mean IOP level in the volunteers prior to caffeine drop instillation was 23.6 ± 2.8 mmHg. The levels 30 minutes after each subsequent treatment were 23.2 ± 1.93, 22.2 ± 1.99, and 22.6 ± 2.31 mmHg, respectively. As summarized in , no significant effect from the caffeine drops was noticeable. Repeated drop instillation did not show any enhancement of IOP. Blood pressure levels also remained unaffected. The results of the initial 1-day study were statistically analyzed and are summarized in .
Figure 1 The bars represent the intraocular pressure of patients given caffeine eye drops as described for (the 1-day study).
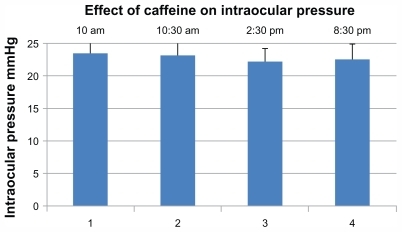
Table 1 Effect of caffeine eye drops on intraocular pressure: 1-day treatment study
To examine the possibility of any long-term effect of caffeine administration, the above study was extended by asking the patients to use the caffeine drops 3 times a day for 6 additional days, as per schedule used during the initial 1-day study, and return to the clinical on day 7 for further pressure measurements. On their return, the patients did not report any unwanted effects except for a general feeling of well-being. Measurement of IOP and caffeine administration was repeated on return as above. The results of this second investigation were statistically analyzed and are summarized in (see also , a bar diagram for easier comprehension). “A” represents the basal readings obtained without any further treatment with the caffeine eye drops. “B,” “C,” and “D” represent the data after caffeine administration as described above for the 1-day investigation. Contrary to expectations, no increase or decrease of IOP was noticed even in this study. The individual basal readings, as well as those determined 30 minutes after administering the drops, remained essentially unchanged. The reading in the group before administration of any drops was 22.6 ± 2.32 mmHg. This was similar to that obtained in the 1-day experiment, which was 23.6 ± 2.8. Subsequent readings at the above time points were 23, 22.4, and 23 mmHg, respectively, indicating no change in IOP after caffeine drop treatment.
Figure 2 The bars represent the intraocular pressure on patients given caffeine eye drops as described under , (the 1 week study).
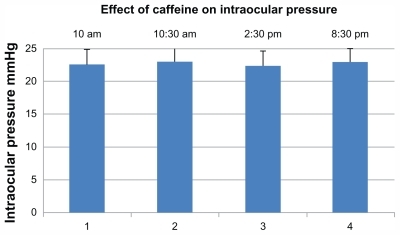
Table 2 Effect of caffeine eye drops on intraocular pressure: 1-week study
Discussion
Caffeine is widely present in various beverages and food items. Medically, it is frequently used as a CNS stimulant and for treating asthma and apnea, the latter primarily in preterm infants.Citation4 The US Food and Drug Administration lists this compound as generally safe for human consumption, the median lethal dose being high (10–15 g in a single dose), which is equivalent to 80–100 cups of coffee. Achieving lethality is difficult. Additionally, regular use of this compound, mostly from coffee or other common beverages, has been reported to provide several very significant health benefits such as reduced incidence of Alzheimer’s and Parkinson’s diseases,Citation51–Citation56 senile dementia, and prevention of neural degeneration in general which is associated with loss of cognitive performance.Citation57,Citation58 Recent reports also suggest that caffeine decreases the risk of development of type 2 diabetes,Citation59,Citation60 loss of liver function and cirrhosis,Citation61,Citation62 and development of certain cancers.Citation63–Citation68
Previous reports suggesting an association between regular use of caffeine and development of hypertension have been significantly toned down in view of recent epidemiological findings.Citation69 The association between hypertension and coffee intake could not be established in a study based on at least 155,000 nurses.Citation70 A Harvard study of 128,000 people concluded that coffee consumption is not associated with coronary heart disease unless it is used in combination with cigarette smoking and excessive use of alcohol. These and many other positive reports, including caffeine’s biochemical properties of scavenging reactive oxygen species, strongly suggest the desirability of further studies regarding its effect on the pathophysiology of ocular diseases. Based on earlier suggestions of possible transient increase in blood pressure caused by caffeine in persons who are not habitual users,Citation4 it was speculated that the caffeine present in coffee might also increase IOP, as a hemodynamic effect. A transient increase of 1–2 mmHg pressure following coffee drinking has indeed been found to be the case in some reportsCitation34–Citation36 but not in others.Citation37–Citation40 The pathophysiological significance of such a small change, if true, remains to be established.
Coffee is not analogous to caffeine.Citation49 Therefore, attributing the effects of coffee drinking on IOP elevation solely to coffee’s caffeine content may be misleading, because coffee contains several other physiologically active substances derived from the coffee beans endogenously, as well as those produced during its processing by roasting and the preparation of the drink itself. Roasted coffee beans are known to contain several bioactive ingredients such as furfural and its derivatives, formaldehyde, and acrolein,Citation71,Citation72 just to mention a few that are all known to be toxic to the eye.Citation73 Their concentrations also differ. It is therefore difficult to exclude the possibility that variation in the levels of these constituents in different coffee brands and preparations might have been responsible for the differences in results reported on IOP in coffee-drinking patients. This limitation applies even in studies where tea, with lower amounts of caffeine (<3 mg), was used as a control. Its composition is very different to that of coffee beans. It was therefore necessary to investigate the effect of caffeine on IOP in glaucoma patients by topical application of the chemically pure compound. Additional studies were also considered important because several recent studies suggest that caffeine appears beneficial to ocular tissues by protecting them against OH• radical-induced oxidative stress. In addition, caffeine can support the tissues metabolically by inhibiting c-AMP phosphodiesterase and thereby maintaining c-AMP levels.Citation74–Citation76 Caffeine’s effect in boosting body ergonomics and memory is now well accepted.
The observed ineffectiveness of caffeine in elevating IOP is not due to any lower doses than can be derived from drinking coffee. The amount used was much higher than that achievable by coffee drinking. The peak plasma level of caffeine following coffee drinking, 1 hour after consumption, varies from 3 to 12 mg/L.Citation77 Being freely diffusible, this level will be similar in intraocular fluids including the aqueous humor. The initial amount of caffeine instilled in the eyes in these experiments was 0.5 mg present in 50 μL of the drop preparation. On closing the eye after instillation, most of it leaked out through the palpebral fissure and nasolacrimal pathway, so about 8–10 μL was retained in the conjunctival sac. Hence, at maximum, a bolus of 0.1 mg of caffeine remains available to equilibrate with the aqueous, with the instant theoretical level of 0.5 mg/mL, (4.5 mM), taking the aqueous volume to be <0.2 mL. Topical instillation of such caffeine drops elevates the aqueous level significantly, as predicted above and as has been shown previously in experiments with rats.Citation78
In summary, therefore, studies with pure caffeine convincingly demonstrate that caffeine does not have any significant effect on IOP in patients with glaucoma/ocular hypertension, as is the case in humans without glaucoma/ ocular hypertension given oral doses of caffeine.Citation50
Disclosure
The authors report no conflicts of interest in this work.
References
- BaroneJJRobertHRCaffeine consumptionFood Chem Toxicol1996341191298603790
- wiseGeekHow much caffeine is consumed by the average person? [Web page on the Internet.]Sparks, NVwiseGeek nd. Available from: http://www.wisegeek.com/how-much-caffeine-is-consumed-by-the-average-person.htmAccessed September 13, 2011
- Energy FiendCaffeine: consumption by country [web page on the Internet]Energy Fiend nd [updated August 18, 2011]. Available from: http://www.energyfiend.com/caffeine-what-the-world-drinksAccessed September 13, 2011
- SerafinWEHardmanJGLimbirdLEMolinoffPBRuddonRWGoodman GillmanAGoodman and Gillman’s Pharmacological Basis of Therapeutics9th editionNew YorkMcGraw Hill1996673679
- ArnaudMJThe pharmacology of caffeineProg Drug Res1987312733133326033
- WilsonDFEffect of caffeine on neuromuscular transmission in ratsAm J Physiol197322548628654355178
- DalyJWBurnsRFSnyderSHAdenosine receptor in the central nervous system; Relationship to the central actions of methylxanthinesLife Sci19812819208320976114369
- DunwiddieTVInteractions between the effects of adenosine and calcium on synaptic responses in rat hippocampus in vitroJ Physiol19843505455596086898
- MorganMDVestalREMethylxanthine effects on caudate dopamine release as measured by in vivo electrochemistryLife Sci198945202520392601563
- PedataFGiovanelliLDe SamoPPepeuBEffect of adenosine derivatives and caffeine on acetylcholine release from the brain synaptosomes: Interaction with muscarinic autoregulatory mechanismsJ Neurochem1986465159315983958718
- SolinasMFerreSYouZBKarcz-KubichaMPopoliPGoldbergSRCaffeine induces dopamine and glutamate release in the shell of the nucleus accumbensJ Neurosci200222156321632412151508
- DegubareffTSleatorWJrEffects of caffeine on t mammalian atrial muscle and its interaction with adenosine and calciumJ Pharmacol Exp Ther196514820221414301011
- BlinksJOOlsonCBJewellBRBravenyPInfluence of caffeine and other methyl xanthines in the mechanical properties of isolated mammalian heart muscleCirc Res19723043673924401230
- DobemeyerJJSteinRALeierRAGreenbergRSchaalSFThe arrythmogenic effects of caffeine in human beingsN Engl J Med1983308148148166835272
- OgawaYEbashiSCa-Releasing action of βγ-methylene adenosine triphosphate on fragmented sarcoplasmic reticulumJ Biochem1976805114911571002681
- RousseauELadineJLiuQYMeissnerGActivation of Ca2+ release channel of skeletal muscle sarcoplasmic reticulum by caffeine and related compoundsArch Biochem Biophys1988267175862848455
- BhatMBZhaoJZangWCaffeine-induced release of intracellular Ca2+ from Chinese hamster ovary cells expressing skeletal muscle ryanodine receptor. Effects on full length carboxyl-terminal portion of Ca2+ release channelsJ Gen Physiol199711067497629382901
- CoronadoRMorrissetteJSukharevaMVaughanDMStructure and function of ryanodine receptorsAm J Physiol19942266 Pt 1C1485C15048023884
- EcheverriDMontesFRCabreraMGalanAPrietoACaffeine’s vascular mechanisms of actionInt J Vasc Med2010201083406021188209
- AchesonKHZahorska-MickiewiczBPittetPAnantharamanKJequierECaffeine and coffee: their influence on metabolic rate and substrate utilization in normal weight and obese individualsAm J Clin Nutr19803359899977369170
- BauerJMaierKLinderkampOHentschelREffects of caffeine on oxygen consumption and metabolic rate in very low birth weight infants with idiopathic apneaPediatrics2001107466066311335740
- BelzaAToubroSAstrupAThe effect of caffeine, green tea and tyrosine on thermogenesis and energy intakeEur J Clin Nutr2009631576417882140
- YeoSEJentjensRLWallisGAJeukendrupAECaffeine increases exogenous carbohydrate oxidation during exerciseJ Appl Physiol200599384485015831802
- BeavoJARogersNLCroffordOBHardmanJGSutherlandWWNewmanEVEffect of xanthine derivatives on lipolysis and on adenosine 3′,5′-monophosphate phosphodiesterase activityMol Pharmacol1970665976034322367
- ShiXDalalNSJainACAntioxidant behavior of caffeine: efficient scavenging of hydroxyl radicalsFood Chem Toxicol1991291161847890
- StadlerRHFayLBAntioxidative reactions of caffeine: formation of 8-oxocaffeine (1,3,7 trimethyl uric acid) in coffee subjected to oxidative stressJ Agric Food Chem19954313321338
- DevasagayamTPKamatJPMohanHKesavanPCCaffeine as an antioxidant: inhibition of lipid peroxidation induced by reactive oxygen speciesBiochim Biophys Acta. Bio membranes1996128216370
- StadlerRHRichozJTureskyRJWeltiDHFayLBOxidation of caffeine and related methylxanthines in ascorbate and polyphenol- driven Fenton-type oxidationsFree Radic Res19962432252408728124
- VarmaSDKumarSRichardsRDLight-induced damage to ocular lens cation pump: prevention by vitamin CProc Natl Acad Sci U S A197976735043506291017
- ChungWGChaYNOxidation of caffeine to theobromine and theophylline is catalyzed primarily by flavin-containing monooxygenase in liver microsomesBiochem Biophys Res Commun199723536856889207220
- DalmazioISantosLSLopesRPEberlinMNAugustiRAdvanced oxidation of caffeine in water: On-line and real-time monitoring by electrospray ionization mass spectrometryEnviron Sci Technol200539165982598816173554
- TeloJPVieiraAJMechanism of free radical oxidation of caffeine in aqueous solutionJ Chem Soc Perkin Trans1997217551757
- VarmaSDKovtunSHegdeKRole of ultraviolet irradiation and oxidative stress in cataract formation: medical prevention by nutritional antioxidants and metabolic agonistsEye Contact Lens201137423324521670697
- HigginbothamEJKilimanjaroHAWilenskyJTBatenhorstRLHermannDThe effect of caffeine on intraocular pressure in glaucoma patientsOphthalmology19899656246262636858
- AvisarRAvisaEWeinbergerDEffect of coffee consumption on intraocular pressureAnn Pharmacother200236699299512022898
- LeydheckerWGlaukom, ein Handbuch [Handbook of Glaucoma]BerlinSpringer-Verlag1960
- PeczonJDGrantWMSedatives, stimulants, and intraocular pressure in glaucomaArch Ophthalmol19647217818814162940
- ChandrasekaranSRochtchinaEMitchellPEffect of caffeine on intraocular pressure: The Blue Mountains Eye StudyJ Glaucoma200514650450716276285
- Jim and Looker [Internet pseudonyms]Caffeine and ocular pressure? MedKB.com [forum on the Internet]MedKB112003 Available from: http://www.medkb.com/Uwe/Forum.aspx/glaucoma/97/Caffiene-and-occular-pressureAccessed September 13, 2011
- WilenskyJTGlaucoma Eye Facts [website on the Internet]Chicago, ILUniversity of Illinois, Department of Ophthalmology and Visual SciencesNovember 102010 Available from: http://www.uic.edu/com/eye/LearningAboutVision/EyeFacts/Glaucoma.shtmlAccessed September 13, 2011
- LeydheckerWThe water-drinking testBritish J Ophthalmol1950348457479
- BuckinghamTYoungRThe rise and fall of intra-ocular pressure; the influence of physiological factorsOphthalmic Physiol Opt19866195993714283
- DranceSMStudies with applanation water testsArch Ophthalmol1963693943
- MouraMARodriguesLOWaisbergYDe AlmeidaHGSilami-GarciaEEffects of submaximal exercise with water ingestion on intraocular pressure in healthy human malesBraz J Med Biol Res200235112112511743624
- ArmalyMFSayeghREWater-drinking test. II. The effect of age on tonometric and tonographic measuresArch Ophthalmol19708321761815411529
- AlimuddinMNormal intra-ocular pressureBr J Ophthalmol195640636637213355942
- AgarwalLPSharmaCKTwo provocative tests for glaucomaBr J Ophthalmol195537633033513059267
- KangJHWilletWCRosnerBAHankinsonSEPasqualeLRCaffeine consumption and the risk of primary open-angle glaucoma: a prospective cohort studyInvest Ophthalmol Vis Sci20084951924193118263806
- IllyEThe complexity of coffeeScientific American20022866869112030095
- AdamsBABrubakerRFCaffeine has no clinically significant effect on aqueous humor flow in the normal human eyeOphthalmology1990978103010312402413
- MaiaLde MendonçaADoes caffeine intake protect from Alzheimer’s disease?Eur J Neurol20029437738212099922
- LindsayJLaurinDVerreaultRRisk factors for Alzheimer’s Disease: a prospective analysis from the Canadian Study of Health and AgingAm J Epidemiol2002156544545312196314
- Institute of Holistic NutritionCaffeine anyone? Available at:http://www.sciencedaily.com/releases/2009/01/090114200005.htm
- RitchieKCarriereIde MendoncaAThe neuroprotective effects of caffeine: a prospective population study (the Three City Study)Neurology200769653654517679672
- RossGWAbbottRDPetrovichHAssociation of coffee and caffeine intake with the risk of Parkinson diseaseJAMA2000283202674267910819950
- BenedettiMDBowerJHMaraganoreDMSmoking, alcohol, and coffee consumption preceding Parkinson’s diseaseNeurology20005591350135811087780
- JarvisMJDoes caffeine intake enhance absolute levels of cognitive performance?Psychopharmacology20051101–245527870897
- Johnson-KozlowMKritz-SilversteinDBarrett-ConnorEMortonDCoffee consumption and cognitive function among older adultsAm J Epidemiol2002156984285012397002
- Salazar-MartinezEWillettWCAscherioACoffee consumption and risk for type 2 diabetes mellitusAnn Intern Med200414011814706966
- HuxleyRLeeCMBarziFCoffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysisArch Intern Med2009169222053206320008687
- KlatskyALMortonCUdaltsovaNFriedmanGDCoffee, cirrhosis, and transaminase enzymesArch Intern Med2006166111190119516772246
- CaddenISPartoviNYoshidaEMReview article: possible beneficial effects of coffee on liver disease and functionAliment Pharmacol200726118
- InoueMYoshimiISobueTTsuganeSJPHC Study GroupInfluence of coffee drinking on subsequent risk of hepatocellular carcinoma: a prospective study in JapanJ Natl Cancer Inst200597429330015713964
- RodriguezTAltieriAChatenoudLRisk factors for oral and pharyngeal cancer in young adultsOral Oncol200440220721314693246
- TavaniABertuzziMTalaminiRCoffee and tea intake and risk of oral, pharyngeal and esophageal cancerOral Oncol200339769570012907209
- SongYJKristalARWicklundKGCushing-HaugenKLRossingMACoffee, tea, colas, and risk of epithelial ovarian cancerCancer Epidemiol Biomarkers Prev200817371271618349292
- GanmaaDWillettWCLiTYCoffee, tea, caffeine and risk of breast cancer: a 22-year follow-upInt J Cancer200812292071207618183588
- FlatowJWilsonKcan coffee lower the risk of prostate cancer [Transcript.]National Public RadioDecember 112009 Available at: http://www.npr.org/templates/story/story.php?storyId=121343438Accessed September 21, 2011
- CromieWCoffee gets cleared of blood pressure riskHarvard Gazette, Nov 2005102006 Available at: http://www.news.harvard.edu/gazette/2005/11.10/06-coffee.html
- Lopez-GarciaEvan DamRMWillettWCCoffee consumption and coronary heart disease in men and women: a prospective cohort studyCirculation2006113172045205316636169
- RizziGPFormation of sulfur-containing volatiles under coffee roastingParliamentTHHoCTSchieberleCaffeinated Beverages: Health Benefits, Physiological Effects, and ChemistryACS Symposium Series754Washington, DCAmerican Chemical Society2000210215
- QuartaBAneseMFurfurals removal from roasted coffee powder by vacuum treatmentFood Chem2011130610614
- GrantWMToxicology of the Eye2nd edSpringfield Illinois: Charles C Thomas1974590502
- VarmaSDHegdeKRPrevention of oxidative damage to lens by caffeineJ Ocul Pharmacol Ther2010261737720148663
- VarmaSDHegdeKRKynurenine-induced photo oxidative damage to lens in vitro: protective effect of caffeineMol Cell Biochem20103401–2495420204679
- WangLLuLPathway-specific effect of caffeine on protection against UV irradiation-induced apoptosis in corneal epithelial cellsInvest Ophthalmol Vis Sci200748265266017251462
- BaseltRDisposition of Toxic Drugs and Chemicals in man9th edSeal Beach, CABiomedical Publications2011
- VarmaSDKovtunSHegdeKEffectiveness of topical caffeine in cataract prevention: studies with galactose cataractMol Vis2010162626263321179241