
Abstract
Purpose
To analyze the real-life clinical outcome of a single dexamethasone implant (DEX) injection in the treatment of persistent diabetic macular edema (DME) after anti-vascular endothelial growth factor (anti-VEGF) agents in a sample of the Jordanian population.
Methods
An observational case study design that involved a retrospective chart review analysis in a tertiary hospital in Amman, Jordan. Patients who showed persistent DME after receiving at least six doses of anti-VEGF agents for DME treatment were included.
Results
The study population consisted of 72 participants (29 females, 43 males) having an average age of 66 years. All patients had best-corrected visual acuity (BCVA) less than 0.7 (6/9) and SD-OCT documented center-involved DME. The study results showed that the average baseline BCVA improved from 0.205±0.1 before DEX injection to 0.358±0.1 at 3 months post-injection (p<0.0001). The central mean thickness (CMT) showed significant improvement also (539.347±132.402 to 379.041±99.430, p<0.0001). There was a mean of 3 mmHg increase in intraocular pressure at 3 months post-injection (p<0.0001), however, only 4% of patients required medical treatment. Other inflammatory biomarkers in OCT, such as intraretinal hyper-reflective dots (HRD), showed significant improvement also (23.67±16 to 14.83±13, p<0.0001). No other significant safety concerns were noticed.
Conclusion
A single DEX injection showed significant clinical and anatomical improvement in DME cases that are persistent after anti-VEGF treatment in our sample, with an excellent safety profile. In case of supply shortage of intravitreal injections, which occurs frequently at our center, a single DEX injection may be utilized as an effective DME therapy. Further research is mandated to identify clinical response in a larger sample and more frequent injections.
Introduction
Diabetes mellitus (DM) is a major global health epidemic. In the United States alone, the lifetime probability of diabetes mellitus for individuals born in 2000 is 33% for males and 39% for females.Citation1 Diabetic macular edema (DME) is an important cause of impairment of vision among patients who have diabetes mellitus, and approximately 50% of the patients who have DME end up having multiple lines of visual acuity loss in less than 2 years of diagnosis.Citation2
The chronic stage of elevated serum glucose is a part of the breakdown of the retinal blood barrier.Citation3 Accumulation of hypoxia, oxygen-free radicals, and mediators of inflammation is likely to result in VEGF-A release, leading to the breakdown of tight junctions present in the blood vessels, ultimately resulting in extravasation of fluids and proteins in the retina and choroid.Citation4 Studies put forward that anti-vascular endothelial growth factor (anti-VEGF) agents like bevacizumab, pegaptanib, and ranibizumab and aflibercept are valuable treatment modalities for the treatment of DME.Citation5–Citation7 Increased utilization of corticosteroids has been observed in the treatment of DME as an alternative treatment for specific patients resistant to laser photocoagulation and intravitreal anti-VEGF treatment.Citation8
The factors of inflammation play a pivotal part in the pathophysiology of diabetic retinopathy along with DME, in suggestion with the chronic illnesses involved.Citation9 Corticosteroids inhibit leukocytosis and expression of prostaglandins and proinflammatory cytokines, enhance vascular tight junctions’ barrier function, and reduce VEGF levels. Therefore, intravitreal corticosteroids may play an essential role as an alternative treatment for DM.Citation6,Citation10
Dexamethasone intravitreal (DEX) implant (0.7 mg) (Ozurdex®, Allergan, Inc., Irvine, CA, USA) consists of micronized Dexamethasone in a biodegradable copolymer of polylactic-co-glycolic acid. It slowly releases steroids into the vitreous over about 6 months.Citation11 In 2014, based on the MEAD study results, the United States Food and Drug Administration (FDA) and most European countries approved DEX to treat DME.Citation12,Citation13
It was demonstrated by Dexamethasone intravitreal implant 0.7 mg (DEX 0.7) that it might improve both central macular thickness (CMT) and best-corrected visual acuity (BCVA) (Boyer et al 2014). Previous studies have focused on the effectiveness of multiple intravitreal dexamethasone (DEX) injections in patients with diabetic muscular edema (DME). The efficacy of Intravitreal injections of DEX combined with anti-vascular endothelial growth factor inhibitors (anti-VEGF) has been proven in several randomized clinical trials, which reported better outcomes than any other treatment plan.Citation14,Citation15 Although DME treatment with DEX involves several injections repeated at variable intervals, we used to have a shortage of supply of drugs for a certain period during the year, which leaves some patients taking only one DEX injection. Therefore, this study aimed to evaluate the effect of a single intravitreal dexamethasone implant (DEX) in patients with persistent DME after anti-vascular endothelial growth factor (anti-VEGF) therapy in a tertiary center in Amman–Jordan.
Materials and Methods
The present study is a retrospective chart review study that included patients with persistent DME that were shifted to treatment with DEX intravitreal injection after anti-VEGF between 2017 and 2019. The study was approved by the Institutional Board Review (IRB) at the Hashemite University. The IRB waived the patient consent form since this was a chart review study. The study protocol involved strict patient data confidentiality, and complies with Declaration of Helsinki. Following were the inclusion criteria: patients with DM, center-involved DME (CI-DME) with central mean subfield thickness (CMT) more than 300 µm on SD-OCT (Topcon, USA) and best-corrected visual acuity (BCVA) less than 6/9 or 0.7 with previous treatment of anti-VEGF for at least 6 consecutive injections, and dexamethasone implant given at least 4 weeks after the last anti-VEGF injection.
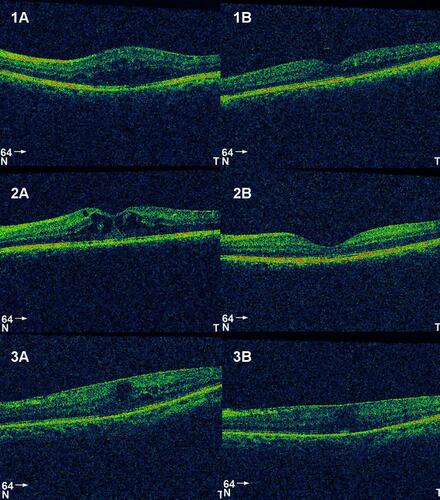
Full demographic data were collected for all patients. Functional and anatomical data before and after DEX injection were also recorded. Those included best-corrected visual acuity (BCVA), intraocular pressure (IOP), CMT, number of previous anti-VEGF injections, the presence of hyperreflective dots on OCT (HRD), type of DME, state of the lens, and use of antiglaucoma or need for glaucoma surgery. We classified DME into four different categories based on OCT: Cystoid Macular Edema (CME) where OCT shows a predominantly cystic pattern, Diffuse DME where OCT shows diffuse retinal thickening, epiretinal membrane (ERM) if OCT shows obvious ERM at the surface of the macula, vitreomacular traction (VMT) in cases where OCT shows anteroposterior traction secondary to abnormally attached vitreous ().
Figure 1 Different variants of DME before (A) and after treatment (B): 1. CME, 2. Diffuse DME, 3. DME with ERM.
The data collection was done in an Excel sheet (Microsoft Corp., 2020, CA, USA). SPSS package (IBM Corp., ver. 26, CA, USA) was employed for statistical analysis utilizing the Student’s t-test for paired data. ANOVA and regression linear modelling were used to assess factors predicting functional and anatomical outcomes. A p-value of 0.05 was used for the cut-off point of clinical significance.
Results
A total of 72 patients were included in the study. shows the demographic data of our sample. The results of the study showed that the average BCVA significantly improved 3 months after DEX injection (0.205±0.1 (log MAR 0.68) to 0.358±0.1 (log MAR 0.44), p<0.0001). An overall decrease in the CMT was observed also after the DEX injection (539.347±132.402 to 379.041±99.430, p<0.0001). The baseline intra-ocular pressure (IOP) before the DEX injection was observed to be 14.847±1.0 and after 3 months of injection increased to 17.805±1.0. Fortunately, only 4.2% of the patients were maintained on antiglaucoma treatment at 3 months. The number of HRD improved after DEX injection from 23.67±16 to 14.83±13 ().
Table 1 Demographic Data
Table 2 Average Results Obtained Pre- and Post-DEX Injection
All types of DME showed significant improvement of BCVA, CMT, and HRD after DEX injection, as shown in , . The presence of ERM was associated with the least changes in CMT and BCVA.
Table 3 Average Results Obtained Pre- and Post-DEX Injection According to the Type of Macular Edema
shows the outcomes classified according to the state of the lens. It shows that patients with cataracts did not have a statistically significant BCVA improvement (0.25 to 0.33, p-value=0.123), although CMT showed a significant reduction (534 to 363, p=0.001).
Table 4 Average Results Obtained Pre- and Post-DEX Injection According to the State of the Lens
Treatment with DEX injection showed a significant reduction in HRD in OCT regardless of the state of the lens and type of DME, except for mixed type DME, where the reduction was not statistically significant. Male gender, lower HbA1c, better BCVA, and a higher number of previous anti-VEGF injections were associated with better final BCVA.
Discussion
The role of chronic inflammation in diabetic macular edema (DME) has been shown by several studies.Citation16–Citation18 The use of anti-VEGF and laser for DME treatment has been associated with some resistance in some cases. Intravitreal steroids have been effectively used to treat DME that persists despite adequate treatment by other modalities of treatment.Citation19
In this study, we tried to investigate the real-life clinical benefit of a single DEX injection in patients with poor or partial response to anti-VEGF injections at our center. Several studies showed that the effect of DEX injection persists up to 3–4 months, and re-injection is usually done after that.Citation20,Citation21 Because of the high patient-volume, our protocol in our center involves a reassessment of patients after DEX injection at 1 week, 1, 3, 4, and 6 months. We repeat BCVA and OCT for the first time at 3 months post-Injection. In this study, we evaluated the clinical effect of DEX injection at 3 months when expected to be at its maximum.
Our results showed improvement of both BCVA and CMT after DEX injection in DME patients after the variable number of intravitreal anti-VEGF, and it was statistically significant. Our findings are consistent with other similar research articles. Esen et al published a series of 25 eyes after a single DEX injection. They showed improvement of mean BCVA from baseline (0.97 ± 0.26 logMAR) to month 3 (0.77 ± 0.34 logMAR, p=0.002). Moreover, CMT improved significantly from baseline (616 ± 132 µm) to 3 months post-injection (339 ± 88 µm).Citation20 The results show that DEX implant may be a viable choice in persistent DME after anti-VEGF injection, and treatment may result in a significant clinical and anatomical improvement. However, several reports indicated a short-lasting effect of DEX injection where it peaks at 1–3 months and starts to deteriorate at 4–6 months. Repeated injection is expected after 3 months. Rishi et al reported a 46% re-injection rate at a variable interval in his 28-eye retrospective series. Of the 17 re-injections, eight (27%) were given at a mean interval of 5 months (median: 4, range: 4–6 months), five (17%) were given after a mean interval of 9 months (median: 9, range: 8–18 months) and four (13%) were given after a mean interval of 18 months (median: 18, range: 18–28 months) following the primary injection.Citation22 Other studies reported variable re-injection rates after 4 months.Citation23,Citation24 In our study, we did not look for the rate of re-injection after 3 months.
Our cohort included patients with different status of the lens. We noticed that patients with preexisting cataract did not show a statistically significant functional improvement while showing a significant anatomical improvement. That was expected since DEX injection is known to cause cataract progression in phakic patients, as reported by several studies.Citation19,Citation25,Citation26 The safety profile of DEX injection in our study was high. None of our patients showed any significant complications after the procedure. There was a mean of 3 mmHg of elevation in intraocular pressure (IOP) at 3 months of follow-up. This elevation was statistically significant but, clinically, only 6 (8.3%) patients had IOP levels above 22 mmHg, and 3 (4.2%) of them were started on IOP-lowering medications. This was much lower than other studies such as MEAD, BEVORDEX, and RELDEX studies.Citation26–Citation28 This difference is mostly attributed to the number of injections since it has been shown that IOP elevation is more with repeated DEX injection.
One of the critical OCT inflammatory biomarkers studied previously in DME patients is hyper-reflective foci (HRD).Citation29,Citation30 It has been shown that the number of HRD decreased after treatment with either anti-VEGF or steroids.Citation31–Citation33 Our cohort showed a significant reduction in HRD in all patients regardless of the type of DME (23.67±16 to 14.83±13, p<0.0001). There was no statistical correlation between the number of HRD and either final BCVA or final CMT at 3 months.
This study has several limitations. First, its retrospective nature renders data collection incomplete or inaccurate sometimes. Second, the sample size is not large compared to the prevalence of DME in Jordan, which may underpower the results and its statistical significance. Third, it includes only patients with only one DEX injection, so we cannot conclude long-term efficacy and treatment frequency in our population, meriting further research to identify DME behaviour in Jordanian population in response to various treatment options. This study did not take into consideration the type of anti-VEGF used. However, up-to-our-knowledge the present study is the first to evaluate DME treatment by either steroids or anti-VEGF in Jordan. It has been conducted in a tertiary hospital where electronic medical records are employed, which improves our data collection accuracy.
Conclusion
The present study aimed to present the effect of a single DEX injection in the treatment of DME that persists after anti-VEGF treatment with a follow-up time of 3 months at our center. Patients in our study showed functional improvement as indicated by BCVA improvement, anatomical improvement as indicated by the reduction of CMT and HRD, and a high safety profile indicated by the low percentage of patients who were started on IOP lowering medications. In case of shortage of supply of medications, we still can manage patients with DME with a single DEX injection and get good functional and anatomical improvement. This treatment strategy is not the standard DEX treatment protocol which requires repeated injections in some patients, but it can be considered in certain centers where logistics may affect the availability of medications.
Disclosure
The authors report no conflicts of interest in this work.
References
- Narayan KMV, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA. 2003;290(14):1884–1890. doi:10.1001/jama.290.14.1884
- Bhagat N, Grigorian RA, Tutela A, Zarbin MA. Diabetic macular edema: pathogenesis and treatment. Surv Ophthalmol. 2009;54(1):1–32.
- Zhang X, Bao S, Lai D, Rapkins RW, Gillies MC. Intravitreal triamcinolone acetonide inhibits breakdown of the blood-retinal barrier through differential regulation of VEGF-A and its receptors in early diabetic rat retinas. Diabetes. 2008;57(4):1026–1033. doi:10.2337/db07-0982
- Zhang X, Zeng H, Bao S, Wang N, Gillies MC. Diabetic macular edema: new concepts in patho-physiology and treatment. Cell Biosci. 2014;4(1):1–14. doi:10.1186/2045-3701-4-27
- Karim R, Tang B. Use of antivascular endothelial growth factor for diabetic macular edema. Clin Ophthalmol. 2010;4:493. doi:10.2147/OPTH.S8980
- Funatsu H, Noma H, Mimura T, Eguchi S, Hori S. Association of vitreous inflammatory factors with diabetic macular edema. Ophthalmology. 2009;116(1):73–79. doi:10.1016/j.ophtha.2008.09.037
- Pacella E, La Torre G, Impallara D, et al. Efficacy and safety of the intravitreal treatment of diabetic macular edema with pegaptanib: a 12-month follow-up. Clin Ter. 2013;164(2):e121–6. doi:10.7417/CT.2013.1543
- Cunningham MA, Edelman JL, Kaushal S. Intravitreal steroids for macular edema: the past, the present, and the future. Surv Ophthalmol. 2008;53(2):139–149. doi:10.1016/j.survophthal.2007.12.005
- Aiello LP, Avery RL, Arrigg PG, et al. Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med. 1994;331(22):1480–1487. doi:10.1056/NEJM199412013312203
- Miyamoto K, Khosrof S, Bursell S-E, et al. Prevention of leukostasis and vascular leakage in streptozotocin-induced diabetic retinopathy via intercellular adhesion molecule-1 inhibition. Proc Natl Acad Sci. 1999;96(19):10836–10841. doi:10.1073/pnas.96.19.10836
- Chang-Lin J-E, Attar M, Acheampong AA, et al. Pharmacokinetics and pharmacodynamics of a sustained-release dexamethasone intravitreal implant. Invest Ophthalmol Vis Sci. 2011;52(1):80–86. doi:10.1167/iovs.10-5285
- Haghjou N, Soheilian M, Abdekhodaie MJ. Sustained release intraocular drug delivery devices for treatment of uveitis. J Ophthalmic Vis Res. 2011;6(4):317.
- Boyer DS, Yoon YH, Belfort JR, et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology. 2014;121(10):1904–1914. doi:10.1016/j.ophtha.2014.04.024
- Nalçacı S, Akkın C, Afrashi F. Dexamethasone implant in patients with diabetic macular edema resistant to anti-VEGF therapy. Turk J Ophthalmol. 2019;49(2):73–77. doi:10.4274/tjo.galenos.2018.84665
- Lally DR, Shah CP, Heier JS. Vascular endothelial growth factor and diabetic macular edema. Surv Ophthalmol. 2016;61(6):759–768. doi:10.1016/j.survophthal.2016.03.010
- Adamis AP, Berman AJ. Immunological mechanisms in the pathogenesis of diabetic retinopathy. In: Seminars in Immunopathology. Vol. 30. Springer; 2008:65–84.
- Joussen AM, Doehmen S, Le ML, et al. TNF-α mediated apoptosis plays an important role in the development of early diabetic retinopathy and long-term histopathological alterations. Mol Vis. 2009;15:1418.
- El-Asrar AMA. Role of inflammation in the pathogenesis of diabetic retinopathy. Middle East Afr J Ophthalmol. 2012;19(1):70. doi:10.4103/0974-9233.92118
- Pacella F, Romano MR, Turchetti P, et al. An eighteen-month follow-up study on the effects of intravitreal dexamethasone implant in diabetic macular edema refractory to anti-VEGF therapy. Int J Ophthalmol. 2016;9(10):1427.
- Esen E, Sizmaz S, Demircan N. Efficacy of dexamethasone intravitreal implant for the treatment of persistent diffuse diabetic macular edema. Int Ophthalmol. 2017;37(1):1–6. doi:10.1007/s10792-016-0219-2
- García-Layana A, Figueroa MS, Arias L, et al. Clinical decision-making when treating diabetic macular edema patients with dexamethasone intravitreal implants. Ophthalmologica. 2018;240(2):61–72. doi:10.1159/000486800
- Rishi P, Rishi E, Attiku Y, Dhami A, Iyer V. Real-world experience with pro re nata dosing of intravitreal dexamethasone implant for eyes with refractory diabetic macular edema. GMS Ophthalmol Cases. 2020;10:10. doi:10.3205/oc000148
- Castro-Navarro V, Cervera-Taulet E, Navarro-Palop C, Monferrer-Adsuara C, Hernández-Bel L, Montero-Hernández J. Intravitreal dexamethasone implant Ozurdex® in naïve and refractory patients with different subtypes of diabetic macular edema. BMC Ophthalmol. 2019;19(1):15. doi:10.1186/s12886-018-1022-9
- Mastropasqua R, Di Antonio L, Di Staso S, et al. Optical coherence tomography angiography in retinal vascular diseases and choroidal neovascularization. J Ophthalmol. 2015;2015:1–8. doi:10.1155/2015/343515
- Fassbender Adeniran JM, Jusufbegovic D, Schaal S. Common and rare ocular side-effects of the dexamethasone implant. Ocul Immunol Inflamm. 2017;25(6):834–840. doi:10.1080/09273948.2016.1184284
- Maturi RK, Pollack A, Uy HS, et al. Intraocular pressure in patients with diabetic macular edema treated with dexamethasone intravitreal implant in the 3-year MEAD study. Retina. 2016;36(6):1143–1152. doi:10.1097/IAE.0000000000001004
- Malclès A, Dot C, Voirin N, et al. Real-life study in diabetic macular edema treated with dexamethasone implant: the Reldex Study. Retina. 2017;37(4):753–760. doi:10.1097/IAE.0000000000001234
- Gillies MC, Lim LL, Campain A, et al. A randomized clinical trial of intravitreal bevacizumab versus intravitreal dexamethasone for diabetic macular edema: the BEVORDEX study. Ophthalmology. 2014;121(12):2473–2481. doi:10.1016/j.ophtha.2014.07.002
- Murakami T, Yoshimura N. Structural changes in individual retinal layers in diabetic macular edema. J Diabetes Res. 2013;2013:1–11. doi:10.1155/2013/920713
- Vujosevic S, Casciano M, Pilotto E, Boccassini B, Varano M, Midena E. Diabetic macular edema: fundus autofluorescence and functional correlations. Invest Ophthalmol Vis Sci. 2011;52(1):442. doi:10.1167/iovs.10-5588
- Kang J-W, Chung H, Chan Kim H. Correlation of optical coherence tomographic hyperreflective foci with visual outcomes in different patterns of diabetic macular edema. Retina. 2016;36(9):1630–1639. doi:10.1097/IAE.0000000000000995
- Vujosevic S, Torresin T, Bini S, et al. Imaging retinal inflammatory biomarkers after intravitreal steroid and anti-VEGF treatment in diabetic macular oedema. Acta Ophthalmol. 2017;95(5):464–471. doi:10.1111/aos.13294
- Vujosevic S, Berton M, Bini S, Casciano M, Cavarzeran F, Midena E. Hyperreflective spots and visual function after anti-vascular endothelia growth factor treatment in center-involving diabetic macular edema. Retina. 2016;36(7):1298–1308. doi:10.1097/IAE.000000000000912