Abstract
The paper describes the first reported case of multifocal choroiditis following simultaneous hepatitis-A, typhoid, and yellow fever vaccinations. A 33-year-old male developed sudden onset of flashing lights and floaters in his right eye 3 weeks following hepatitis A, typhoid, and yellow fever vaccinations. Fundus examination and angiography confirmed the presence of multiple peripheral chorioretinal lesions. These lesions demonstrated characteristic morphologic changes over a period of 8 weeks which were consistent with a diagnosis of self-resolving multifocal choroiditis. Vaccine-induced intraocular inflammation has been described infrequently. We demonstrate the first case of self-resolving multifocal choroiditis following simultaneous administration of hepatitis A, yellow fever, and typhoid immunizations.
Case report
A previously healthy 33-year-old male was referred to our retina service for sudden onset of intermittent floaters and flashing lights in his right eye which developed 3 weeks following inactivated hepatitis A, yellow fever, and typhoid vaccinations. These vaccines were given prophylactically in preparation for a 2-week trip to Panama at the Ohio State University Wexner Medical Center Travel and Immunization Clinic. The patient had previously received one dose of the hepatitis A vaccine 12 years prior (he did not complete the series) and had never before been exposed to typhoid or yellow fever immunizations.
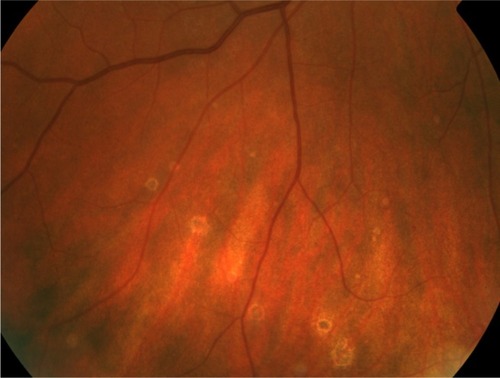
On examination, visual acuity was 20/20 in both eyes. Pupil responses, visual fields to confrontation, and intraocular pressures (14 mmHg) were normal bilaterally. Slit lamp examination revealed 1+ anterior vitreous inflammation bilaterally. Fundus examination of the right eye revealed a few scattered peripheral nonpigmented chorioretinal lesions. The macula and optic nerve appeared normal, and the left fundus was unremarkable. Fluorescein angiography of the right eye demonstrated scattered peripheral hyperfluorescent lesions correlating with those seen in the fundus, and there was no evidence of disc leakage (). A comprehensive review of systems was negative for fever, rash, oral ulcers, arthralgias, headache, or vertigo. There was no history of autoimmune disease or recent viral illness. There was no family history of autoimmune disease. The patient was diagnosed as having acute multifocal choroiditis and observed. After 2 weeks, the patient continued to describe occasional floaters. His ocular examination revealed continued low grade anterior vitreous inflammation and the peripheral retinal lesions began to demonstrate early hyperpigmentation (). Because of the nonprogressive examination findings and given the excellent visual acuity, it was decided to continue close observation. At 8 weeks, the patient’s symptoms had resolved, the vitreous was clear of cellular inflammation, and the fundus revealed punched out areas of retinal pigment epithelium atrophy.
Figure 1 Late frame fluorescein angiographic photograph of the right eye demonstrating well demarcated hyperfluorescent lesions.
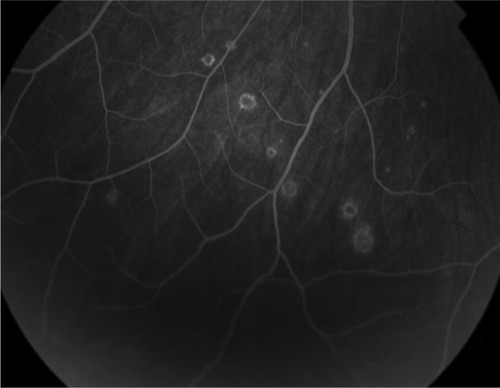
Figure 2 Color fundus photograph of the right eye demonstrating well circumscribed chorioretinal lesions with hyperpigmentation.
Discussion
Vaccines potentiate both humoral and cellular immune responses by exposing lymphocytes to pathogen-specific antigens which triggers an inflammatory T cell-mediated reaction and initiates the steps of adaptive immunity and development of cellular memory. Autoimmune phenomena have been infrequently observed following vaccination, and possible mechanisms proposed to explain some of these occurrences include the roles of excessive lymphocyte activation, cytokine expression, and molecular mimicry.Citation1
Cross-reactivity of an activated immune response against uveal antigens may occur when peptide fragments presented to T cells show close conformational resemblance to uveal self-peptides. Melanin-associated molecules present in choroid have been shown experimentally to be capable of inducing ocular inflammation.Citation2
Another possible method of immune system activation following vaccination relates to the use of vaccine adjuvants. Adjuvants are routinely combined with vaccines to potentiate their immunogenic activity and these have been used in animal models to create uveitis.Citation2 Aluminum-containing adjuvants are used widely in vaccine formulations licensed for use in the US, including hepatitis A. Crucial to the adjuvant activity of aluminum is the influx of inflammatory factors, including dendritic cells, to the site of injection. These cells can recognize and process foreign antigens, as well as provide the costimulatory molecules necessary for activating plasma cell production of target antibodies.Citation3 Rarely, erythema, subcutaneous nodules, contact hypersensitivity, and granulomatous inflammation have been observed with the use of aluminum adjuvants.Citation4 The currently used preparation of typhoid and yellow fever vaccines are free of adjuvants.
There are a few case reports in the literature describing posterior uveitis syndromes occurring shortly after vaccination. Specifically, multiple evanescent white dot syndrome was reported 10 days following simultaneous hepatitis A and yellow fever vaccines, and acute posterior multifocal placoid pigment epitheliopathy was described in association with hepatitis B and varicella vaccinations.Citation5–Citation7 A review of 32 cases of uveitis following hepatitis B vaccination included a few reports of positive rechallenge response in patients who developed recurrent uveitis following separate doses of the hepatitis B vaccine.Citation8 Most of the reported cases of uveitis demonstrated self-resolution, although recently a case of ampiginous choroiditis was described following human papilloma virus vaccination which required treatment with oral prednisone and resulted in macular scarring.Citation9
Multifocal choroiditis is an inflammatory disease characterized by multiple, small, yellow fundus lesions, and vitreous inflammation. Presenting symptoms include blurry vision, floaters, and photopsias. Although the etiology of multifocal choroiditis remains unknown, there have been suggestions of autoimmune and viral associations. The primary location of pathology involves the retinal pigment epithelium. The choriocapillaris and choroid are richly invested with certain potential antigen-presenting cells and the retinal pigment epithelium can be induced to express major histocompatibility complex Class II molecules, suggesting it may be able to interact with T lymphocytes. There is experimental evidence that high densities of T lymphocytes, B lymphocytes, and macrophages can infiltrate the choroid and stimulate synthesis of cytokines capable of altering the subsequent immune response.Citation10 During the late stage of the disease, the spots adopt a rim of hyperpigmentation and often assume the classic punched-out appearance of retinal pigment epithelium atrophy with bands of subretinal fibrosis at their margins. To our knowledge, this is the first reported case of multifocal choroiditis following vaccination.
Although this case does not prove causation and the relationship remains presumptive, it does suggest that some vaccinations can act as a trigger for immunologic initiation that could subsequently lead to the development of noninfectious uveitis.
Disclosure
The authors report no conflicts of interest in this work.
References
- JampolLMBeckerKGWhite spot syndromes of the retina: a hypothesis based on the common genetic hypothesis of autoimmune/inflammatory diseaseAm J Ophthalmol200513537637912614757
- BorekhuyseRMKuhlmannEDWinkensHJExperimental autoimmune anterior uveitis (EAAU). Induction by immunization with purified uveal and skin melaninsExp Eye Res1993565755838500566
- KoolMFierensKLambrechtBNAlum adjuvant: some of the tricks of the oldest adjuvantJ Med Microbiol20126192793422174375
- GuptaRKAluminum compounds as vaccine adjuvantsAdv Drug Deliv Rev19983215517210837642
- StangosAZaninettiMPetropoulosIBaglivoEPournarasCMultiple evanescent white dot syndrome following simultaneous hepatitis A and yellow fever vaccinationOcular Immunol Inflamm200614301304
- FineLFineACunninghamETMultiple evanescent white dot syndrome following hepatitis A vaccinationArch Ophthalmol20011191856185711735803
- FineHFKimEFlynnTEGomesNLChangSAcute posterior multifocal placoid pigment epitheliopathy following varicella vaccinationBr J Ophthalmol20109428228318728052
- FraunfelderFWSuhlerEBFraunfelderFTHepatitis B vaccine and uveitis: an emerging hypothesis suggested by review of 32 case reportsCutan Ocul Toxicol201029262919947819
- KhalifaYMMonahanPMAcharyaNRAmpiginous choroiditis following quadrivalent human papilloma virus vaccinationBr J Ophthalmol20104913713920385534
- StreileinJWMaNNgTFZamiriPImmunobiology and privilege of neuronal retina and pigment epithelium transplantsVision Res20024248749511853765