Abstract
Purpose
To investigate changes in the area of the foveal avascular zone (FAZ) in patients with retinal vascular disease.
Patients and methods
This retrospective, consecutive study examined 53 eyes of 53 patients with macular edema due to branch retinal vein occlusion in 25 patients (47.2%) and nonproliferative diabetic retinopathy in 28 patients (52.8%). The macular edema was treated with an intravitreal injection of 0.05 mL equal to 1.25 mg bevacizumab. Before and 6–8 weeks after the injection, best corrected visual acuity, slit lamp biomicroscopy of the anterior segment and fundus, optical coherence tomography, and fluorescein angiography were conducted. The FAZ was manually circumscribed on early-phase angiography images and the area of the FAZ was measured.
Results
The preoperative overall mean FAZ area was 0.327 ± 0.126 mm2 (median 0.310 mm2). At the control consultation, the overall mean area was significantly larger (0.422 ± 0.259 mm2; median 0.380 mm2; P < 0.001). In the nonproliferative diabetic retinopathy subpopulation, the mean area was 0.361 ± 0.129 mm2 (median 0.330 mm2) before bevacizumab application and 0.434 mm2 at the follow-up visit (mean increase 0.071 mm2/19.7%). In the branch retinal vein occlusion group, the baseline FAZ area was 0.290 ± 0.115 mm2 and 0.407 ± 0.350 mm2 at follow-up (median 0.330 mm2; mean increase 0.117 mm2/40.3%). No cases of severe operation-associated complications were observed.
Conclusion
The results confirm the safety of intravitreal bevacizumab injection in patients with macular edema due to nonproliferative diabetic retinopathy and branch retinal vein occlusion. The enlargement of the FAZ could be equivalent to an increase in retinal ischemia. These results may be transient; a potential vascular risk, however, when applying antivascular endothelial growth factor therapy in eyes with preexistent vascular disease must be considered.
Introduction
Management of macular edema following branch retinal vein occlusion (BRVO) and nonproliferative diabetic retinopathy (NPDR) is challenging. Except photocoagulation, which used to be the initial therapy of choice, the pharmacologic inhibition of vascular endothelial growth factor (VEGF) shows promise.Citation1,Citation2 In the meantime, ranibizumab has become the therapy of choice for BRVO with macular edema and a visual acuity of 20/40 and less.
VEGF is a multifunctional cytokine. It is not only crucial for cell proliferation, cell migration, proteolysis, cell survival, and maintenance of the choriocapillaris, it also facilitates survival and development of retinal neurons following ischemia and it is necessary for preservation of normal vessels.Citation3–Citation7 Its role in angiogenesis and organogenesis is vital; the loss of one single VEGF allele results in embryonic death.Citation8 One of its major inducers is hypoxia.Citation9 Therefore, it plays an important role in ocular diseases in which retinal malperfusion is developing, eg, diabetic macular disease or BRVO.Citation10 Furthermore, VEGF stimulates endothelial mitogenesis, promotes endothelial survival, and controls vascular permeability. It is 50,000 times more potent in inducing vascular leakage than histamine, causing macular edema when released in the vitreous cavity of monkeys.Citation11,Citation12 Development of macular edema causes impairment of visual acuity in these pathological conditions.
There is great evidence from large prospective randomized trials for the efficacy of anti-VEGF therapy in diabetic macular edema (DME), macular edema following BRVO, and age-related macular degeneration.Citation13–Citation22 A novel agent, aflibercept (Eylea®, Regeneron Pharmaceuticals, Inc, Tarrytown, NY, USA), now augments the pharmacological anti-VEGF armamentarium.Citation23 This soluble decoy receptor shows a higher affinity and faster association to VEGF-A than ranibizumab or bevacizumab.Citation24
This study presents two groups of patients who were diagnosed with macular disease secondary to DME or BRVO and consequently treated with a single dose of intravitreal bevacizumab. Both groups demonstrated a significantly enlarged foveal avascular zone (FAZ) at the 6–8-week follow-up.
Material and methods
In this retrospective consecutive study, more than 200 patients with NPDR or BRVO who visited the Department of Ophthalmology of Technical University of Munich (Munich, Germany) between June 2008 and December 2009 were screened, and 53 patients were included. These 53 individuals suffered from macular edema due to NPDR or BRVO and also had a well-circumscribed FAZ, both visible on fluorescein angiography. The study was approved by the local institutional review board (Ethics Commission, Faculty of Medicine, Technical University of Munich) and informed consent was obtained from every patient for the intravitreal injection. The subjects were also provided information about the off-label use of the drug.
The mean age of the patients was 67.4 years; 31 female (58.5%) and 22 male (41.5%) patients were included. The macular edema was caused by NPDR in 28 patients (52.8%) and by BRVO within the last 6 months in 25 patients (47.2%). The exclusion criteria were macular disease secondary to causes other than DME or BRVO, any ongoing ocular or periocular inflammation, any kind of ocular surgeries on the studied eye within the last 6 months, or any previous treatment of the macular edema (eg, any intravitreal injection for macular edema in the last 6 months or laser treatment at any time in the past for macular edema).
Examinations at baseline included best corrected visual acuity with a Snellen chart at a distance of 20 feet, slit lamp biomicroscopy of the anterior segment and fundus (Slit Lamp BM 900®; Haag-Streit AG, Koeniz, Switzerland), optical coherence tomography (Spectralis®; Heidelberg Engineering, Heidelberg, Germany), and fluorescein angiography (Heidelberg Retina Angiograph II; Heidelberg Engineering).
The intravitreal injection of 0.05 mL with 1.25 mg bevacizumab was performed in accordance with the guidelines for intravitreal injections published by the Macula Committee of the German Ophthalmological Society and the Professional Association of Ophthalmologists of Germany.Citation25 Before injection administration, the eye was washed with povidone-iodine (5%) and the eyelashes and lid region were then wiped, also with povidone-iodine (5%). The drape (as used for intraocular intervention) was applied, a lid speculum was inserted. After dislocation of the conjunctivae, the injection was performed at a distance of 3.5 mm from the limbus. Consecutively, each patient received an injection of 1.25 mg bevacizumab (Avastin®; F Hoffmann-La Roche, Basel, Switzerland). Antibiotic eye drops were then applied. At day one and day three after the injection, a slit lamp examination was performed to rule out intraocular inflammation or elevated intraocular pressure.
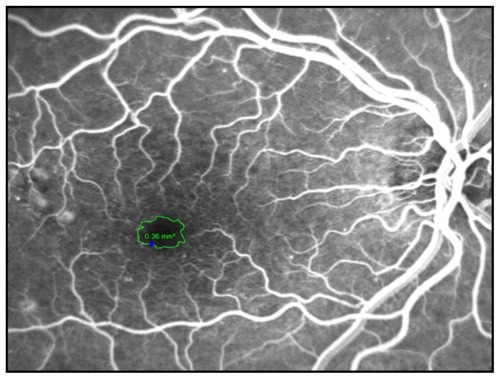
In order to visualize the FAZ, the angiography was performed with scanning laser technology, and only patients with good quality early-phase fluorescein angiograms without any bleeds or exudates hindering visualization of the macular region were included for evaluation. The FAZ was manually circumscribed by two experienced retina consultants in these early-phase fluorescein angiograms, once by each of them (). Heidelberg Eye Explorer software (version 1.7.0.0; Heidelberg Engineering) yielded the area (in mm2). The mean value was used for further calculations and patients with differing values of more than 0.05 mm2 were excluded.
Figure 1 The foveal avascular zone was manually circumscribed on an early-phase fluorescein angiogram and the software measured the area (in mm2).
Patients returned to the outpatient clinic for routine postinjection follow-up. Best corrected visual acuity, slit lamp biomicroscopy of the anterior segment and fundus, optical coherence tomography, and fluorescein angiography were conducted again at 6–8 weeks postinjection. The area of FAZ was assessed again in the above described manner. Statistical analysis was performed using SPSS version 13 (SPSS Inc, Chicago, IL, USA) with the Wilcoxon matched-pairs test and t-test.
Results
All patients tolerated the injection well. There were no cases of operation-associated complications such as retinal detachment, endophthalmitis, or persistent elevated intraocular pressure. Two patients reported ocular discomfort for a few days, and seven patients (13.2%) showed a mild hyposphagma at the injection site that disappeared without further treatment within 10 days. The mean FAZ was significantly larger at the control visit after 6–8 weeks compared to the previous values for all patients (Wilcoxon: P < 0.001). Preoperative parameters showed a mean area of 0.327 ± 0.126 mm2 (median 0.310 mm2). After the first visit, the mean area increased to 0.422 ± 0.259 mm2 (median 0.380 mm2) (; ).
Figure 2 Box plots summarize the increase in foveal avascular zone area (mm2) at FU1 compared to pre OP measurements for all patients (overall) and the patients with DME and BRVO.
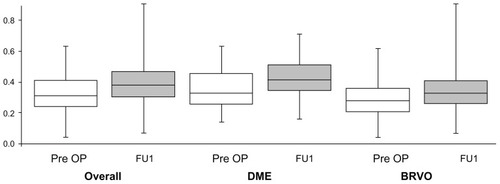
Table 1 Foveal avascular zone area measurements
An analysis to differentiate between the underlying diagnoses was also performed. In the NPDR group (n = 28), the baseline mean FAZ area was 0.361 ± 0.129 mm2 (median 0.330 mm2). At the follow-up, the mean area increased by 0.071 mm2 (or 19.7%) to 0.434 mm2 (; ).
The subjects with BRVO (n = 25) showed a slightly smaller FAZ area at baseline compared to the diabetic group (0.290 ± 0.115 mm2 versus 0.361 ± 0.129 mm2). At the follow-up, the mean area increased by 0.117 mm2 (or 40.3%) to 0.407 ± 0.350 mm2 (median 0.330 mm2; ; ).
Discussion
In February 2004, the US Food and Drug Administration approved bevacizumab as the first angiogenesis inhibitor for first-line treatment of cancer; and favorable results led to extended use in non-small-cell lung cancer, kidney cancer, and glioblastoma. As a nonselective inhibitor of all isoforms of the VEGF, this humanized antibody also suppresses vital physiological functions like its vasodilatory effect or the stimulated expression of plasminogen activators, resulting in arterial thromboembolic events.Citation26–Citation31 Ultrastructural analyses showed the reduction of choriocapillaris endothelial cell fenestrations and emerging thrombosis.Citation32–Citation34 Evidence for vasoconstriction of retinal vessels was published, altogether raising concerns about retinal vascular events.Citation35–Citation37
This retrospective study found a significant increase in the area of the FAZ 6–8 weeks after a single intravitreal injection of 1.25 mg bevacizumab. There were no significant complications after intravitreal bevacizumab, including endophthalmitis, retinal detachment, cataract formation, increased intraocular pressure, or retinal artery occlusion. The presented results are in accordance with previous observations.Citation38 Several multicenter clinical trials also did not detect any elevated incidence of severe side effects in anti-VEGF therapy; and reports on increased intraocular pressure and ischemia are seldom, with no adverse event rate exceeding 0.21%.Citation39–Citation45 Mansour et al determined the overall risk of ocular vascular events following VEGF antagonist injection as 0.108% in a general population and 2.61% in diabetic patients, and refer to the patients’ perioperative stress and the natural history of their conditions.Citation46
There are several publications that attempt to measure retinal ischemia on fluorescence angiography as the size of the FAZ. Neubauer et al used a high-resolution ultra wide-field scanning ophthalmoscopy system for counting retinal fields of nonperfusion in a group of 19 nonresponders to photocoagulation.Citation47 The number of avascular fields dropped significantly, but the diameter of the FAZ remained quasi unchanged, as it did in a prospective, consecutive, noncomparative case series with 126 diabetic pretreated patients at a 12-month follow-up.Citation14 Another group measured an area of capillary nonperfusion in the context of intravitreal bevacizumab for macular edema following BRVO; they found an unchanged mean area of nonperfusion.Citation48 One reason for this could be the slightly different period of time between intervention and the second data acquisition. Nevertheless, the current study yielded different results.
A statistically significant enlargement of the FAZ 6 to 8 weeks after one intravitreal injection of 1.25 mg bevacizumab in patients with macular edema both secondary to NPDR and BRVO was found. This effect may be transient. Papadopoulou et al found a vasoconstrictor impact of ranibizumab on retinal arteries after application of ranibizumab, suggesting that closure of the smallest vessels approaching the FAZ could enlarge this area on fluorescein angiography.Citation35 A recent report defined the FAZ as a factor of macular ischemia and found a negative effect of an enlarged FAZ on short-term visual outcomes after intravitreal bevacizumab for DME.Citation49
Some limitations are inherent in the current study. First, the design was retrospective, the sample size was small (both groups totaled 53 eyes), and there was no control group. As the natural course of the disease also leads to increasing vascular stress and enlargement of the FAZ, it is not known without doubt that the results are secondary to the use of bevacizumab. Second, this one-time follow-up of the patients does not describe the development of the FAZ over time and the results may be transient, especially since the effects of intravitreal bevacizumab have been reported to vanish within weeks after a single application.Citation50 Third, the period from BRVO or the onset of diabetes to the application of bevacizumab was not defined. It is likely that different durations of ischemia yield a varying response to anti-VEGF treatment.
Conclusion
The results show that intravitreal injection of anti-VEGF drugs may induce an increase in the area of the FAZ, a morphological retinal change visualized by fluorescein angiography. In the light of retinal ischemia, this may cause further problems. Altogether, the findings emphasize only one single aspect of intravitreal anti-VEGF treatment in patients with preexistent vascular disease; they underline the necessity to consider the potential vascular risk when applying anti-VEGF therapy in eyes with preexistent vascular disease, which is common in patients with DME or BRVO. A standardized method to assess the FAZ and further investigations are necessary to describe the relationship between intravitreal bevacizumab, microvascular changes in the FAZ, and long-term visual acuity results.
Disclosure
The authors report no conflicts of interest in this work.
References
- Early Treatment Diabetic Retinopathy Study Research GroupEarly photocoagulation for diabetic retinopathy. ETDRS report number 9Ophthalmology199198Suppl 57667852062512
- The Branch Vein Occlusion Study GroupArgon laser photocoagulation for macular edema in branch vein occlusionAm J Ophthalmol19849832712826383055
- ThakkerGDHajjarDPMullerWARosengartTKThe role of phosphatidylinositol 3-kinase in vascular endothelial growth factor signalingJ Biol Chem199927415100021000710187776
- TiltonRGChangKCLeJeuneWSStephanCCBrockTAWilliamsonJRRole for nitric oxide in the hyperpermeability and hemodynamic changes induced by intravenous VEGFInvest Ophthalmol Vis Sci199940368969610067972
- BernatchezPNRollinSSokerSSiroisMGRelative effects of VEGF-A and VEGF-C on endothelial cell proliferation, migration and PAF synthesis: role of neuropilin-1J Cell Biochem200285362963911968003
- MarnerosAGFanJYokoyamaYVascular endothelial growth factor expression in the retinal pigment epithelium is essential for choriocapillaris development and visual functionAm J Pathol200516751451145916251428
- Saint-GeniezMMaldonadoAED’AmorePAVEGF expression and receptor activation in the choroid during development and in the adultInvest Ophthalmol Vis Sci20064773135314216799060
- HaighJJRole of VEGF in organogenesisOrganogenesis20084424725619337405
- FerraraNVascular endothelial growth factor: basic science and clinical progressEndocr Rev200425458161115294883
- FunatsuHYamashitaHNomaHMimuraTYamashitaTHoriSIncreased levels of vascular endothelial growth factor and interleukin-6 in the aqueous humor of diabetics with macular edemaAm J Ophthalmol20021331707711755841
- OzakiHHayashiHVinoresSAMoromizatoYCampochiaroPAOshimaKIntravitreal sustained release of VEGF causes retinal neovascularization in rabbits and breakdown of the blood–retinal barrier in rabbits and primatesExp Eye Res19976445055179227268
- DvorakHFBrownLFDetmarMDvorakAMVascular permeability factor/vascular endothelial growth factor, microvascular hyperpermeability, and angiogenesisAm J Pathol19951465102910397538264
- ChangTSBresslerNMFineJTDolanCMWardJKlesertTRImproved vision-related function after ranibizumab treatment of neovascular age-related macular degeneration: results of a randomized clinical trialArch Ophthalmol2007125111460146917998507
- KookDWolfAKreutzerTLong-term effect of intravitreal bevacizumab (Avastin) in patients with chronic diffuse diabetic macular edemaRetina20082881053106018779710
- PragerFMichelsSKriechbaumKIntravitreal bevacizumab (Avastin) for macular oedema secondary to retinal vein occlusion: 12-month results of a prospective clinical trialBr J Ophthalmol200993445245619074916
- KondoMKondoNItoYIntravitreal injection of bevacizumab for macular edema secondary to branch retinal vein occlusion: results after 12 months and multiple regression analysisRetina20092991242124819672216
- NguyenQDBrownDMMarcusDMRanibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDEOphthalmology2012119478980122330964
- MitchellPBandelloFSchmidt-ErfurthUThe RESTORE study: ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edemaOphthalmology2011118461562521459215
- GregoriNZGaitanJRosenfeldPJLong-term safety and efficacy of intravitreal bevacizumab (Avastin) for the management of central retinal vein occlusionRetina20082891325133719430392
- GregoriNZRattanGHRosenfeldPJSafety and efficacy of intravitreal bevacizumab (Avastin) for the management of branch and hemiretinal vein occlusionRetina200929791392519584649
- CampochiaroPABrownDMAwhCCSustained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve-month outcomes of a phase III studyOphthalmology2011118102041204921715011
- HeierJSCampochiaroPAYauLRanibizumab for macular edema due to retinal vein occlusions: long-term follow-up in the HORIZON trialOphthalmology2012119480280922301066
- BoyerDHeierJBrownDMVascular endothelial growth factor Trap-Eye for macular edema secondary to central retinal vein occlusion: six-month results of the phase 3 COPERNICUS studyOphthalmology201211951024103222440275
- PapadopoulosNMartinJRuanQBinding and neutralization of vascular endothelial growth factor (VEGF) and related ligands by VEGF Trap, ranibizumab and bevacizumabAngiogenesis201215217118522302382
- JaissleGBSzurmanPBartz-SchmidtKURecommendation for the implementation of intravitreal injections – statement of the German Retina Society, the German Society of Ophthalmology (DOG) and the German Professional Association of Ophthalmologists (BVA)Klin Monbl Augenheilkd20052225390395 German15912456
- ScappaticciFASkillingsJRHoldenSNArterial thromboembolic events in patients with metastatic carcinoma treated with chemotherapy and bevacizumabJ Natl Cancer Inst200799161232123917686822
- CannistraSAMatulonisUAPensonRTPhase II study of bevacizumab in patients with platinum-resistant ovarian cancer or peritoneal serous cancerJ Clin Oncol200725335180518618024865
- EreminaVJeffersonJAKowalewskaJVEGF inhibition and renal thrombotic microangiopathyN Engl J Med2008358111129113618337603
- HurwitzHISaltzLBVan CutsemEVenous thromboembolic events with chemotherapy plus bevacizumab: a pooled analysis of patients in randomized phase II and III studiesJ Clin Oncol201129131757176421422411
- SchutzFAJeYAzziGRNguyenPLChoueiriTKBevacizumab increases the risk of arterial ischemia: a large study in cancer patients with a focus on different subgroup outcomesAnn Oncol20112261404141221115602
- PragerGWBreussJMSteurerSMihalyJBinderBRVascular endothelial growth factor (VEGF) induces rapid prourokinase (pro-uPA) activation on the surface of endothelial cellsBlood2004103395596214525763
- PetersSHeiduschkaPJulienSZiemssenFFietzHBartz-SchmidtKUUltrastructural findings in the primate eye after intravitreal injection of bevacizumabAm J Ophthalmol20071436995100217449002
- MeyerTRobles-CarrilloLRobsonTBevacizumab immune complexes activate platelets and induce thrombosis in FCGR2A transgenic miceJ Thromb Haemost20097117118118983497
- VidinovaCVidinovNThe effect of bevacizumab on the ultrastructure of choroidal neovascular membranes in patients with age-related macular degeneration (AMD)Klin Monbl Augenheilkd20092266491495 German19507100
- PapadopoulouDNMendrinosEMangiorisGDonatiGPournarasCJIntravitreal ranibizumab may induce retinal arteriolar vasoconstriction in patients with neovascular age-related macular degenerationOphthalmology200911691755176119560206
- SacuSPempBWeigertGResponse of retinal vessels and retrobulbar hemodynamics to intravitreal anti-VEGF treatment in eyes with branch retinal vein occlusionInvest Ophthalmol Vis Sci20115263046305021051706
- SolimanWVintenMSanderBOptical coherence tomography and vessel diameter changes after intravitreal bevacizumab in diabetic macular oedemaActa Ophthalmol200886436537118028237
- FeuchtNMatthiasHLohmannCPMaierMPegaptanib sodium treatment in neovascular age-related macular degeneration: clinical experience in GermanyClin Ophthalmol20082225325919668713
- FungAERosenfeldPJReichelEThe International Intravitreal Bevacizumab Safety Survey: using the internet to assess drug safety worldwideBr J Ophthalmol200690111344134916854824
- RosenfeldPJRichRMLalwaniGARanibizumab: phase III clinical trial resultsOphthalmol Clin North Am200619336137216935211
- BrownDMKaiserPKMichelsMRanibizumab versus verteporfin for neovascular age-related macular degenerationN Engl J Med2006355141432144417021319
- van der ReisMILa HeijECDe Jong-HesseYRingensPJHendrikseFSchoutenJSA systematic review of the adverse events of intravitreal anti-vascular endothelial growth factor injectionsRetina20113181449146921817960
- YokoyamaKChoshiTKimotoKShinodaKNakatsukaKRetinal circulatory disturbances following intracameral injection of bevacizumab for neovascular glaucomaActa Ophthalmol200886892792818494739
- KimKSChangHRSongSIschaemic change after intravitreal bevacizumab (Avastin) injection for macular oedema secondary to non-ischaemic central retinal vein occlusionActa Ophthalmol200886892592718494740
- HuangZLLinKHLeeYCSheuMMTsaiRKAcute vision loss after intravitreal injection of bevacizumab (Avastin) associated with ocular ischemic syndromeOphthalmologica20102242868919707032
- MansourAMShahinMKofoedPKParodiMBShamiMSchwartzSGInsight into 144 patients with ocular vascular events during VEGF antagonist injectionsClin Ophthalmol2012634336322419856
- NeubauerASKookDHaritoglouCBevacizumab and retinal ischemiaOphthalmology200711411209617980746
- TeruiTKondoMSugitaTChanges in areas of capillary nonperfusion after intravitreal injection of bevacizumab in eyes with branch retinal vein occlusionRetina20113161068107421451440
- ChungEJRohMIKwonOWKohHJEffects of macular ischemia on the outcome of intravitreal bevacizumab therapy for diabetic macular edemaRetina200828795796318698297
- MirshahiARoohipoorRLashayAMohammadiSFAbdoallahiAFaghihiHBevacizumab-augmented retinal laser photocoagulation in proliferative diabetic retinopathy: a randomized double-masked clinical trialEur J Ophthalmol200818226326918320520