Abstract
Purpose
To introduce a novel, noninvasive technique to determine the depth and extent of anterior corneal stroma changes induced by collagen cross-linking (CXL) using quantitative analysis of high-resolution anterior-segment optical coherence tomography (OCT) post-operative images.
Setting
Private clinical ophthalmology practice.
Patients and methods
Two groups of corneal cross-sectional images obtained with the OptoVue RTVue anterior-segment OCT system were studied: group A (control) consisted of unoperated, healthy corneas, with the exception of possible refractive errors. The second group consisted of keratoconic corneas with CXL that were previously operated on. The two groups were investigated for possible quantitative evidence of changes induced by the CXL, and specifically, the depth, horizontal extent, as well as the cross-sectional area of intrastromal hyper-reflective areas (defined in our study as the area consisting of pixels with luminosity greater than the mean +2 × standard deviation of the entire stromal cross section) within the corneal stroma.
Results
In all images of the second group (keratoconus patients treated with CXL) there was evidence of intrastromal hyper-reflective areas. The hyper-reflective areas ranged from 0.2% to 8.8% of the cross-sectional area (mean ± standard deviation; 3.46% ± 1.92%). The extent of the horizontal hyper-reflective area ranged from 4.42% to 99.2% (56.2% ± 23.35%) of the cornea image, while the axial extent (the vertical extent in the image) ranged from 40.00% to 86.67% (70.98% ± 7.85%). There was significant statistical difference (P < 0.02) in these values compared to the control group, in which, by application of the same criteria, the same hyper-reflective area (owing to signal noise) ranged from 0.00% to 2.51% (0.74% ± 0.63%).
Conclusion
Herein, we introduce a novel, noninvasive, quantitative technique utilizing anterior segment OCT images to quantitatively assess the depth and cross-sectional area of CXL in the corneal stroma based on digital image analysis. Mean cross-sectional area showing evidence of CXL was 3.46% ± 1.92% of a 6 mm long segment.
Introduction
Keratoconus (KCN) is a degenerative bilateral, progressive, noninflammatory disorder characterized by ectasia, thinning, and increased curvature of the cornea, and is associated with loss of visual acuity, particularly in relation to high-order aberrations.Citation1–Citation4
Corneal collagen cross-linking (CXL) with riboflavin and ultraviolet-A irradiation is a common technique for tissue stabilization.Citation5,Citation6 Several studies have shown that CXL is an effective intervention to halt the progression of keratoconus and corneal ectasia.Citation7
Anterior-segment optical coherence tomography (AS-OCT) is a promising imaging mode providing high-resolution cross-sectional images across a meridian of choices that can be employed in KCN diagnosis.Citation8,Citation9 The most advanced AS-OCT systems invariably employ Fourier spectral-domain signal processing. As of today, there are a number of different spectral domain OCT systems commercially available.Citation10,Citation11
The ability to provide real-time cross sectional mapping, in conjunction with the very principle of operation, namely photon back scattering, provides the understudied application of quantitative assessment of the extent of stromal changes due to CXL.
OCT and CXL demarcation line observations
To date, the efficacy of CXL treatment can be monitored only indirectly by postoperative follow-up observations, such as with a Scheimpflug camera,Citation12 or with corneal confocal microscopy.Citation13
In addition, a corneal stromal demarcation line indicating the transition zone between cross-linked anterior corneal stroma and untreated posterior corneal stroma can be detected in slit-lamp examination as early as 2 weeks after treatment.Citation14 In our clinical assessment, the presence of this finding over the anterior two-thirds of the stroma confirms that sufficient CXL treatment has occurred.
Following our presentation and the introduction in the peer-reviewed literature of the use of OCT imaging in order to evaluate the CXL-induced demarcation line, OCT has seen some recent interest as a tool for investigating CXL effects, such as corneal thickness before and after CXL for KCN, and demarcation line depth following CXL.Citation15–Citation22
The principle lies in the fact that although these lines do not appear to affect vision, as they correspond to changes in stromal density, they appear as brighter (hyper-reflective) areas on cross-sectional corneal OCT scans. However, the depth and extent of stromal changes induced by CXL has been difficult to evaluate quantitatively in the clinic.
The motivation for our study was to advance this aforementioned theory by examining not only the demarcation line depth between the suspected CXL and the deeper cornea with corneal OCT, but also to attempt to quantitatively assess the extent of this area on a large number of patients over a large postoperation interval. Our novel technique is based on digital signal processing on cross-sectional OCT images of corneas, and evaluates quantitatively and, in our opinion, free of examiner bias, the extent of CXL changes in the corneal stroma.
Methods
This prospective interventional case series study received approval by the Ethics Committee of our Institution and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from each subject at the time of the CXL intervention or at the first clinical visit. The study was conducted in our clinical practice on patients during their regular clinical visits (control group) and scheduled postoperative procedure visits (KCN group).
Patient inclusion criteria
The control group (50 patients, 100 eyes) consisted of patients with eyes with unoperated corneas (ie, normal eyes with no ocular pathology other than refractive error). Mean patient age was 35.2 ± 9.1 years (range 19–48), equally divided between males and females. Before OCT corneal mapping, a complete ocular examination and tomographic topography was performed to screen for corneal abnormalities.
The second group (47 patients, 94 eyes) consisted of KCN patients previously operated with CXL by employing the Athens Protocol, which combined same-day phototherapeutic keratectomy epithelial removal and partial topographically-guided photorefractive keratectomy normalization of the cornea ectasia, followed by high-fluence, short-duration riboflavin induced CXL.Citation21
The mean patient age in this group was 28.1 ± 7.1 years (range 16–45 years). There is a bias towards males in this group (33 males, 14 females), which is consistent with our clinical experience of the male–female incidence of keratoconic patients, and with previous reports.Citation2 Of the 94 eyes included in the study, 47 were oculus sinister and 47 were oculus dexter. Mean postoperative time since CXL operation was 17.65 ± 20.83 months, with a range of 1 to 72 months.
Most patients enrolled in the group had bilateral CXL operation, and thus both eyes were included in the study, while in some patients only one eye was included in the study. For some patients, images from more than one visit were included in the study (separated by at least 3 months).
Materials
The OptoVue RTVue (OptoVue Inc, Fremont, CA, USA) AS-OCT system was employed in the study. Using the L-Cam lens, a 6 mm long Hi-Res Cross Line Scan, centered at the pupil center along the vertical meridian, was recorded. The meridional cross-sectional images were processed with the RTVue software (version 5.1.0, processing algorithm A5, 1, 0, 90). The software averages up to 32 successive acquisitions. In our study, we included images consisting of at least five averages.
Our novel investigation technique
All images from both groups were investigated for possible quantitative evidence of changes induced by CXL. Evidence of such was considered as the existence of the intrastromal hyper-reflective demarcation line. To search for such a line, images were loaded into commercially available software, Adobe Photoshop CS5 Version 12.04 (Adobe Systems Inc, San Jose, CA, USA).
For every meridional cross-sectional image, the pixels associated with the stromal cross-section were selected with the marquee tool. The area separated by 10 pixels from the anterior and the exterior corneal surfaces were deselected, as they are typically of higher luminosity (). The extent (pixel count) of the selected stromal image area was determined with the histogram tool report. The dialog box for this tool also provides the mean ± standard deviation of the luminosity for the selected area.
Figure 1 (A) Typical cornea cross-sectional meridian image of a patient with KCN. (B) The selected hyper-reflective intrastromal area is indicated in red.
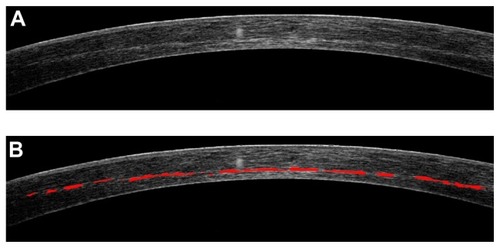
The hyper-reflective demarcation area was quantitatively defined in this study as the population of pixels (pixel count) having luminosity greater than the value defines as luminosity mean +2 × standard deviations, as obtained in the previous step.
Subsequently, after using the histogram tool report again, the extent (pixel count) of the hyper-reflective intrastromal area was recorded, as well as its horizontal extent (pixels across the y axis), and this was compared to the horizontal extent of the captured image, which was set to a standard of 860 pixels across the y-axis.
Similarly, the axial extent (depth of demarcation line) was assessed and compared to the depth of the corneal section (vertical line in the image; that is, pixels in the x-axis) to which it corresponded.
Descriptive statistics (average, minimum, maximum, standard deviation, bias, and range), comparative statistics, and linear regression were performed in Microsoft Excel 2010 (Microsoft Corp, Redmond, WA, USA) and OriginLab version 8 (OriginLab Corp, Northampton, MA, USA). Analysis of variance between groups was performed using the OriginLab statistics tool.
Results
Areal extent (depth and diameter) of demarcation
Cross-sectional meridian area measurements had an average of 59,183 pixels (±5778), ranging from 80,729 to 39,951 (maximum to minimum). This corresponds to an area of 2.88 mm2. Mean luminosity values were, on a grayscale of 0 to 255, 63 ± 13, ranging from 89 to 25 (maximum to minimum).
As shown in , the intrastromal hyper-reflective area found with this technique for group A (control) had a mean area of 427.25 ± 373.81 pixels (range, maximum to minimum, 1518-0), corresponding to a mean of 0.74% ± 0.63% (range, 2.50%–0.00%), corresponding to 0.02 mm2. This contrasts with group B (KCN), in which the mean hyper-reflective area had a mean of 2018.21 ± 1104.70 (range, 4927–121), corresponding to a mean of 3.46% ± 1.92% (range, 8.80%–0.18%), or 0.098 mm2 of the corneal cross-sectional area. Of the 94 cases examined, 72 had more than 2.50% hyper-reflective areas, whereas six were close to and 16 were below this mark. The two groups were found to be statistically different (comparison of hyper-reflective area pixel count; P < 0.02). The over time development of the extent of the area of demarcation; that is, the CXL area over post-operative time, is plotted in .
Figure 2 Demarcation line area as a function of time elapsed since the CXL operation.
Abbreviation: CXL, cross-linking.
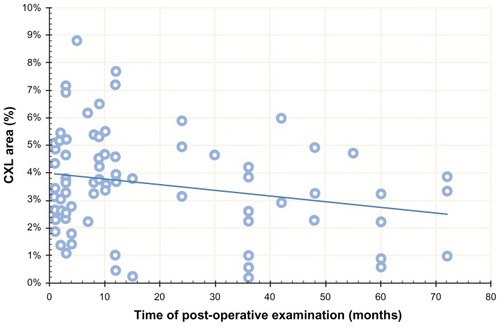
Table 1 Hyper-reflective area corresponding to meridional corneal cross section, as measured in the two groups
Horizontal extent of demarcation
The horizontal extent of demarcation was assessed for the KCN group and was compared to the standard 860 pixel width extent of the corneal cross-section. As shown in , on average the extent of the hyper-reflective area (CXL width) was 483.35 ± 200.82 pixels (range, 853–38), corresponding to an average of 56.20% of the cross-section width, ranging from 99.19% to 4.42%. Of the subgroup of 78 corneas with more than a 2.50% hyper-reflective area, the minimum was 12.45%.
Table 2 Horizontal and axial extent of hyper-reflective area in group B (KCN)
Axial extent (depth) of demarcation
The axial extent of demarcation corresponds to what we describe as the depth of the CXL effect. The quantitative assessment is subject to the corneal thickness, which varies significantly among images. In each image studied, the corneal thickness was measured in pixels (vertical line total in ), and was found to correspond to an average of 61.93 ± 8.18 pixels (max to min, 80–38). Considering that 6 mm across the image corresponded to 860 pixels, the 61.93 pixels corneal thickness translates to 432 μm of thickness.
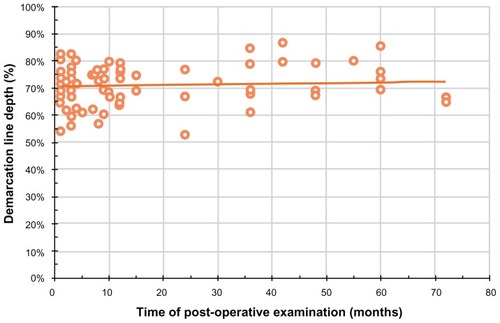
Having measured the corneal thickness of each individual section, the distance in pixels (vertical line CXL) from the anterior corneal surface was measured. On average, it was found to be 43.81 ± 6.96 pixels (range, 65–30), corresponding to 305.6 μm or 70.98% of the total corneal thickness. The over time (postoperative) development of the depth of the area of demarcation, that is CXL area over time, is presented in .
Figure 3 Demarcation line depth as a function of time elapsed since the CXL operation.
Abbreviation: CXL, cross-linking.
Discussion
By examining high-resolution corneal OCT images, we encountered statistically different findings between the treated group (KCN; group B) and the control group (A).
It appears that there is a statistically significant difference between the control group and the KCN group regarding the presence of a demarcation line, as quantitatively measured by the extent of the area of the hyper-reflective demarcation line, indicating a localized change in stromal (treated) density over the underlying (untreated) stroma.
In 72 of 94 cases, the demarcation line area corresponded to more than 2.50% of the total corneal cross-sectional area, with a mean ± standard deviation of 3.46% ± 1.92%. In the entire control group A, by applying the same luminosity criteria, the similar area had a mean of 0.74% ± 0.63%. We believe that these pixel counts represent merely signal noise rather than reflect actual changes in stromal density. Thus, we can ascertain that the demarcation line viewed by OCT can be a good indication of the extent of collagen density changes induced by CXL.
Over time, these density changes become less apparent. The trend line shown in has a negative slope (reduced by 0.02% per month), indicating that the demarcation line area fades away by postoperative month 12, in agreement with our clinical findings.Citation15
The depth of the demarcation line, found to be on average of 305 μm, is consistent with the accepted notion that in order to avoid ultraviolet-A irradiation damage to the corneal endothelium,Citation23 the CXL parameters are set in a way that effective treatment occurs only in the first 300 μm of the corneal stroma.Citation12
The depth of the demarcation line appears, on the other hand, to be stable over time, even after 3 years following operation, at approximately 70% of the corneal depth. However, a deeper demarcation line depth (relative to the corneal depth) is associated with thinner corneal thickness, as measured postoperatively. In the selected 12 thinner corneas, the depth of the demarcation line was found to be 83% of the total corneal thickness.
One clinical example of ineffective CXL action is demonstrated in , in which a case of a cornea treated in another institution with epithelium-on CXL technique demonstrated minimal signs of hyper-reflective areas.Citation24 This case, which was not part of the case study, was presented to our practice with progressive ectasia following the CXL operation in another practice. Examples of corneal cross-sectional images examined in the study showing various degrees of demarcation line extent are presented in .
Figure 4 Example of epithelium-on CXL cornea with minimal appearance of the demarcation line.
Abbreviation: CXL, cross-linking.
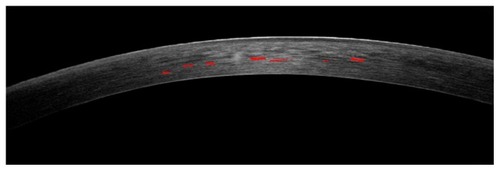
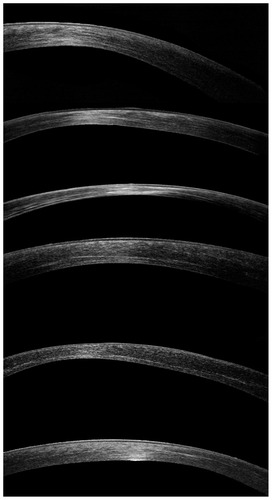
Figure 5 Example of corneal cross-sectional images examined in the study showing various degrees of demarcation line extent.
Conclusion
AS-OCT appears to demonstrate reproducible early (1 month) and long-term (up to 3 years) CXL cornea findings. The hyper-reflective lines may represent induced cornea density changes or subtle intrastromal cornea scarring. This novel quantitative and qualitative technique may constitute a possible benchmark for a noninvasive measurement to evaluate and titrate the amount, extent, and depth of intrastromal effects of the CXL treatment in KCN and possibly ectasia eyes.
Disclosure
The authors report no conflicts of interest in this work.
References
- KrachmerJHFederRSBelinMWKeratoconus and related noninflammatory corneal thinning disordersSurv Ophthalmol19842842933226230745
- BelinMWAsotaIMAmbrosioRJrKhachikianSSWhat’s in a name: keratoconus, pellucid marginal degeneration, and related thinning disordersAm J Ophthalmol2011152215716221708379
- AmbrósioRJrCaldasDLda SilvaRSPimentelLNde FreitasVBImpact of the wavefront analysis in refraction of keratoconus patientsRev Bras Oftalmol2010695294300 Portuguese
- KosakiRMaedaNBesshoKMagnitude and orientation of Zernike terms in patients with keratoconusInvest Ophthalmol Vis Sci20074873062306817591874
- GkikaMLabirisGKozobolisVCorneal collagen cross-linking using riboflavin and ultraviolet-A irradiation: a review of clinical and experimental studiesInt Ophthalmol201131430931921847678
- DahlBJSpottsETruongJQCorneal collagen cross-linking: an introduction and literature reviewOptometry2012831334222153823
- JankovMRIiJovanovicVDelevicSCoskunsevenECorneal collagen cross-linking outcomes: reviewOpen Ophthalmol J20115192021448301
- LiYMeislerDMTangMKeratoconus diagnosis with optical coherence tomography pachymetry mappingOphthalmology2008115122159216618977536
- LiYTanOBrassRWeissJLHuangDCorneal epithelial thickness mapping by fourier-domain optical coherence tomography in normal and keratoconic eyesOphthalmology2012119122425243322917888
- KiernanDFMielerWFHariprasadSMSpectral-domain optical coherence tomography: a comparison of modern high-resolution retinal imaging systemsAm J Ophthalmol20101491183120103039
- GrewalDSBrarGSJainRGrewalSPComparison of Scheimpflug imaging and spectral domain anterior segment optical coherence tomography for detection of narrow anterior chamber anglesEye (Lond)201125560361121336254
- KránitzKKovácsIMiháltzKCorneal changes in progressive keratoconus after cross-linking assessed by Scheimpflug cameraJ Refract Surg201228964564922947293
- FilippelloMStagniEBuccolieroDBonfiglioVAvitabileTTransepithelial cross-linking in keratoconus patients: confocal analysisOptom Vis Sci20128910e1e722940781
- SeilerTHafeziFCorneal cross-linking-induced stromal demarcation lineCornea20062591057105917133053
- KanellopoulosAJNovel cornea OCT findings in early and long-term follow-up of collagen crosslinking for keratoconusProceedings of the American Academy of OphthalmologyOctober 24–27, 2009San Francisco, CA, USA
- KanellopoulosAJComparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconusJ Refract Surg2009259S812S81819772257
- KanellopoulosAJThe management of cornea blindness from severe corneal scarring, with the Athens Protocol (transepithelial topography-guided PRK therapeutic remodeling, combined with same-day, collagen cross-linking)Clin Ophthalmol20126879022347790
- MencucciRPaladiniIVirgiliGGiacomelliGMenchiniUCorneal thickness measurements using time-domain anterior segment OCT, ultrasound, and Scheimpflug tomographer pachymetry before and after corneal cross-linking for keratoconusJ Refract Surg201228856256622785060
- DoorsMTahzibNGEgginkFABerendschotTTWebersCANuijtsRMUse of anterior segment optical coherence tomography to study corneal changes after collagen cross-linkingAm J Ophthalmol2009148684485119781685
- YamJCChanCWChengACCorneal collagen cross-linking demarcation line depth assessed by Visante OCT after CXL for keratoconus and corneal ectasiaJ Refract Surg201228747548122767165
- OrtizSPérez-MerinoPAlejandreNGambraEJimenez-AlfaroIMarcosSQuantitative OCT-based corneal topography in keratoconus with intracorneal ring segmentsBiomed Opt Express20123581482422567577
- KanellopoulosAJLong term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconusClin Ophthalmol201269710122275813
- BaggaBPahujaSMurthySSangwanVSEndothelial failure after collagen cross-linking with riboflavin and UV-A: case report with literature reviewCornea201231101197120022960648
- StojanovicAChenXJinNSafety and efficacy of epithelium-on corneal collagen cross-linking using a multifactorial approach to achieve proper stromal riboflavin saturationJ Ophthalmol2012201249843522900147