Abstract
Purpose
The study reported here investigated the efficacy, tolerability, and safety of the preservative-free prostaglandin analog tafluprost 0.0015% in treatment-naive patients.
Patients and methods
Data were collected in two non-interventional, prospective, multicenter, observational, open-label studies of identical design that were conducted in Germany and the Czech Republic. All subjects received preservative-free tafluprost 0.0015% once daily. Intraocular pressure (IOP) levels were recorded for each eye at untreated baseline and 3 months after initiation of medical treatment. The primary outcome was change in mean IOP from baseline to month 3. In the primary open-angle glaucoma (POAG) and ocular hypertension (OH) patient subgroups, analyses were stratified by the level of baseline IOP: ≥20 to 23 mmHg versus ≥24 mmHg. In addition, responder rates and the achievement of pre-specified IOP levels at month 3 were evaluated. Local tolerance of preservative-free tafluprost was evaluated by the patients at final visit. Overall satisfaction with the medical treatment was evaluated by both patients and physicians. All adverse events were recorded.
Results
A total of 579 treatment-naive patients with POAG (n = 349), OH (n = 105), normal tension glaucoma (n = 71), exfoliative glaucoma (n = 27), or other glaucomas (n = 27) were included in this observational study. Mean IOP level at baseline for all patients was 23.6 ± 4.0 mmHg. Mean IOP at month 3 was 16.8 ± 2.9 mmHg (−28.8% vs baseline). At month 3, significant reductions in mean IOP (P < 0.001) were seen in all patients and all subgroups. Preservative-free tafluprost lowered mean IOP significantly in patients with POAG and OH with IOP levels ≥ 20 to 23 mmHg from 21.9 ± 1.1 mmHg at baseline to 16.5 ± 2.2 mmHg, and in the subgroup with IOP levels ≥ 24 mmHg from 26.2 ± 2.4 mmHg to 17.9 ± 2.4 mmHg. In the subgroups of patients with POAG and OH, an IOP response ≥20%, ≥30%, and ≥40% was achieved by 83.4%, 44.1%, and 12.8%, respectively. Overall, patients with higher baseline IOP values showed a better response than patients with lower baseline IOP levels. Preservative-free tafluprost was well tolerated and safe. After 3 months, 97.9% of all patients remained on therapy.
Conclusion
In this real-world observational study, treatment with once-daily preservative-free tafluprost proved efficacious, well tolerated, and safe in treatment-naive patients.
Introduction
Lowering intraocular pressure (IOP) using anti-glaucoma medications is considered the first-line effective treatment for glaucoma.Citation1–Citation5 Worldwide, prostaglandin analogs (PGAs) have become the major therapeutic class for the medical treatment of glaucoma because of their efficacy and generally well-tolerated systemic safety profile.Citation6 Tafluprost (marketed as Taflotan, Tapros, and Saflutan and manufactured by Santen Oy, Tampere, Finland) is highly selective for the prostanoid prostaglandin F receptor.Citation7–Citation9 PGAs including tafluprost have a strong, sustained, and stable IOP-lowering effect with few systemic side effects. In clinical studies, preservative-free tafluprost lowered IOP effectively and was generally well tolerated.Citation10–Citation13 Further, among all widely used PGAs, tafluprost has been the first preparation to be available in a preservative-free formulation.
Benzalkonium chloride (BAK), which is widely used in glaucoma preparations as a preservative, is pro-apoptotic, pro-inflammatory, causes damage to the tear film by disrupting the lipid-layer, and has a negative impact on the number of conjunctival goblet cells.Citation14–Citation18 Other clinical studies have demonstrated major differences with respect to subjective symptoms, local tolerability, and objective clinical signs after the use of glaucoma medications containing preservatives and those that are preservative free.Citation19–Citation21 These subjective symptoms and clinical signs may have a negative impact on adherence and persistence of glaucoma patients.Citation22,Citation23 It should also be considered that there is a high prevalence of ocular surface disease in patients treated for glaucoma and ocular hypertension (OH).Citation24–Citation26 Finally, the long-term treatment of glaucoma patients with eye drops containing preservatives may have a negative impact on the outcome of filtration sugery.Citation15,Citation27
The purpose of this study was to assess the efficacy, tolerability, and safety of preservative-free tafluprost in treatment- naive patients in a routine clinical setting. Prospective, randomized, double-masked clinical trials have provided strong evidence of the efficacy and safety of preservative-free tafluprost;Citation10–Citation13 however, they may not completely reflect the conditions found in routine clinical settings due to their restrictive design and inclusion and exclusion criteria. In these clinical trials, usually both treatment-naive patients and those who had had prior medical treatment were included. It remains of interest to prospectively assess the efficacy, tolerability, and safety of preservative-free tafluprost used in monotherapy in a large cohort of treatment-naive patients with different diagnoses and a broad range of baseline IOP levels.
Materials and methods
Study design
This was a prospective, noninterventional, observational, open-label, nonrandomized, multicenter study conducted between July 2009 and March 2011 in Germany and the Czech Republic. A total of 266 centers in Germany and 65 centers in the Czech Republic participated, providing data on 579 treatment-naive patients. The initiation of medical treatment was based on the decision of the physician only. Laws of both countries do not require informed consent for this type of noninterventional observational study.
Treatment-naive patients with glaucoma or OH were followed for 3 months after initiation of medical therapy with the preservative-free formulation of tafluprost 0.0015% once daily. The primary objective of this study was to evaluate the change in mean IOP between baseline and final visit. The secondary objective was to determine the change in IOP in different subgroups of treatment-naive patients (primary open-angle glaucoma [POAG], OH, normal tension glaucoma [NTG], exfoliative glaucoma [PEX], and other glaucomas [ie, secondary glaucoma, pigment dispersion, glaucoma with narrow angle component, or not specified]). Further, we evaluated the impact of baseline IOP levels on the IOP-lowering effect of preservative-free tafluprost 0.0015% in patients with POAG and OH. For this analysis, patients with POAG and OH were stratified by baseline IOP levels (≥20 to 23 mmHg and ≥24 mmHg). The cut off level of 24 mmHg was thought to be clinically relevant to roughly distinguish between patients with high versus moderately elevated IOP levels. Tolerability of preservative-free tafluprost and overall satisfaction with preservative-free tafluprost was evaluated at month 3. Adverse events and terminations of medical treatment were recorded.
Patients
The study included patients with different types of unilateral or bilateral glaucoma (POAG, NTG, PEX, and other glaucomas) and OH who required initiation of medical hypotensive treatment and who had never been treated for OH or glaucoma. The initiation of medical treatment was based on the decision of the physician only. Patients with contraindications and known sensitivities to any component of preservative-free tafluprost were excluded from participation according to the summary of product characteristics for preservative-free tafluprost.Citation28
Treatment and assessments
Using standardized data collection forms, investigators provided anonymous patient data. As already indicated, initiation of medical treatment with preservative-free tafluprost was at the physician’s discretion. Due to the observational character of the study, no instructions were made to the study participants concerning the time of IOP measurements during the day and when to administer the medication during the day (evening or morning dose). Demographic information collected included age, sex, and type of glaucoma. IOP readings were taken at untreated baseline and at the patient’s final visit, 3 months after the initiation of medical therapy, using Goldman applanation tonometry in each eye with the patient in a sitting position at the slit lamp. Glaucomatous damage was identified by ophthalmoscopy, automatic perimetry, and/or optic nerve head/fundus imaging techniques. At month 3, subjects were asked to evaluate the tolerability of preservative-free tafluprost referring to a five-point scale (“very good,” “good,” “satisfactory,” “less satisfactory,” and “not acceptable”). Overall patient and doctor satisfaction with the medication was evaluated using a four-point scale (“very satisfied,” “satisfied,” “less satisfied,” and “not satisfied”). All adverse events reported by patients and/or observed by physicians and all terminations of medical treatment were recorded.
Statistical analysis
Efficacy analyses used only IOP measurements of one study eye per subject. If both eyes of a subject were eligible, the eye with the higher IOP at baseline was considered the study eye. If the baseline IOP was the same in both eyes, the right eye was considered the study eye. Paired t-tests were conducted to compare mean IOP values at baseline with IOP values 3 months after initiation of treatment with tafluprost 0.0015%. The significance in percentages of patients achieving pre-specified percentage IOP reductions and target IOP levels between the POAG and OH subgroups (stratified by baseline IOP ≥ 20 to 23 mmHg and ≥24 mmHg) was assessed using chi-square tests. The two-sided significance level was set at 0.05.
Results
Patient demographics
In total, 579 treatment-naive patients were included in this observational study between July 2009 and March 2011. Most patients were female (n = 327; 56.5%) and the mean age was 58.1 years. POAG was the most common diagnosis (n = 349; 60.3%), followed by OH (n = 105; 18.1%), NTG (n = 71; 12.3%), PEX (n = 27; 4.7%), and other glaucomas (n = 27; 4.7%) ().
Table 1 Patient demographics
Effect on mean IOP
Overall, mean IOP (±standard deviation [SD]) was 23.6 ± 4.0 mmHg at baseline. Three months after initiation of medical therapy, IOP decreased significantly to 16.8 ± 2.9 mmHg. This IOP decrease is equivalent to 6.8 mmHg, or 28.8%, versus untreated baseline. A significant decrease in mean IOP was also achieved for all different subgroups by diagnosis: in patients with POAG (n = 349), mean IOP (±SD) was significantly lowered from 24.6 ± 2.9 mmHg at baseline to 17.3 ± 2.4 mmHg at final visit; in patients with OH (n = 105), from 24.4 ± 2.6 mmHg to 17.5 ± 2.4 mmHg; in patients with NTG (n = 71), from 16.6 ± 1.9 mmHg to 13.3 ± 2.4 mmHg; in patients with PEX (n = 27), from 25.8 ± 3.5 mmHg to 17.5 ± 2.4 mmHg; and in patients with other glaucomas (n = 27), from 23.7 ± 5.4 mmHg to 16.7 ± 4.4 mmHg. Further details are shown in .
Table 2 Change in mean intraocular pressure (IOP) from baseline to final visit 12 weeks after initiation of medical therapy with preservative-free tafluprost
Percentage IOP reduction and achievement of target IOP levels
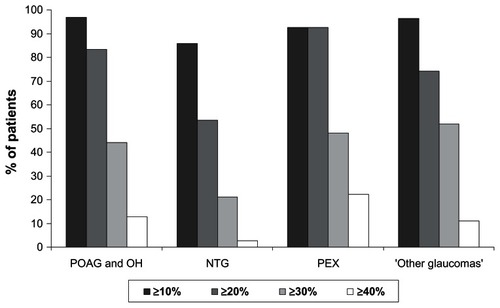
In patients with POAG or OH, an IOP reduction ≥ 20% versus untreated baseline IOP levels was achieved by 83.4% of patients and an IOP reduction ≥ 30% and ≥40% by 44.1% and 12.8% of patients, respectively. In the subgroup of patients with PEX, 92.6% achieved an IOP reduction ≥ 20% and 48.1% and 22.2% of patients achieved an IOP reduction ≥ 30% and ≥40%, respectively. Percentage IOP reduction was lower in the patient subgroup with NTG: 53.5% of patients achieved an IOP reduction ≥ 20% versus untreated baseline, while 21.1% and 2.8% achieved an IOP reduction ≥ 30% and ≥40%, respectively ().
Figure 1 Percentage intraocular pressure (IOP) reduction at final visit versus untreated baseline for different patient subgroups.
Abbreviations: NTG, normal tension glaucoma; OH, ocular hypertension; PEX, exfoliative glaucoma; POAG, primary open-angle glaucoma.
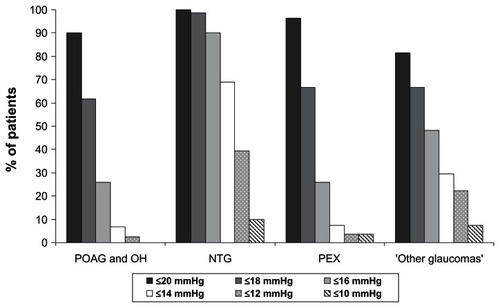
The target IOP level of ≤18 mmHg was achieved by 61.7% of patients with POAG and OH and by 98.6%, 66.7%, and 66.7% of patients with NTG, PEX, and other glaucomas, respectively. A low target IOP level of ≤14 mmHg was achieved by 6.7%, 69.0%, 7.4%, and 29.6% of patients with POAG/OH, NTG, PEX, and other glaucomas, respectively ().
Figure 2 Achievement of specific intraocular pressure levels at final visit versus untreated baseline for different patient subgroups.
Reduction in IOP in patients with POAG and OH stratified by baseline IOP levels
At month 3, mean IOP levels decreased from baseline by 5.4 ± 2.2 mmHg (−24.7%) in the subgroup of patients with baseline IOP levels ≥ 20 to 23 mmHg and by 8.3 ± 3.0 mmHg (−31.7%) in the subgroup of patients with baseline IOP levels ≥ 24 mmHg (P < 0.0001 for within-group comparison) (). Similarly large percentages of patients achieved ≥10% IOP reductions at month 3 compared with untreated baseline in both subgroups: 94.2% in the ≥20 to 23 mmHg subgroup and 98.6% in the ≥24 mmHg subgroup (P = 0.119) (). A significantly smaller percentage of patients in the ≥20 to 23 mmHg subgroup achieved IOP reductions – ≥30% compared with the ≥24 mmHg subgroup (29.7% vs 52.8% respectively; P < 0.0001%). However, significantly smaller percentages of patients in the ≥24 mmHg subgroup achieved IOP levels ≤ 21 mmHg, ≤18 mmHg, or ≤15 mmHg at month 3 (P ≤ 0.05 for IOP levels ≤ 21 mmHg and P < 0.0001 for IOP levels ≤ 18 or ≤15 mmHg) ().
Figure 3 Achievement of specific intraocular pressure (IOP) levels at final visit versus untreated baseline in all patients with primary open-angle glaucoma (POAG) and ocular hypertension (OH) and in the two subgroups stratified by baseline IOP levels at month 3 after initiation of medical treatment.
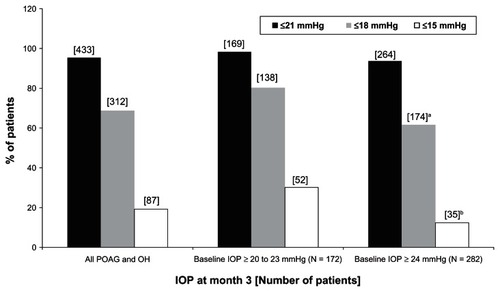
Table 3 Intraocular pressure (IOP) ± standard deviation (SD) in patients with primary open-angle glaucoma and ocular hypertension at baseline and at month 3 after initiation of medical treatment
Local tolerability and satisfaction
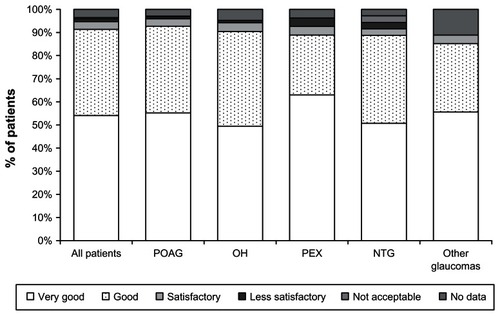
At final visit, 3 months after the initiation of medical treatment, the local tolerability of preservative-free tafluprost was rated as “very good” or “good” by 91.4% of all treatment-naive patients. Evaluation of local tolerability was comparable in all patient subgroups. Local tolerability of preservative-free tafluprost was rated as “less satisfactory” or “not acceptable” by only a few patients (1.7% of all patients; 1.2% of patients with POAG, 1.0% of patients with OH, 3.7% of patients with PEX, and 1.4% of patients with NTG) (). Most patients (96.5%) and physicians (95.2%) were either “very satisfied” or “satisfied” with the medical treatment at final visit.
Figure 4 Local tolerability of preservative-free tafluprost at month 3 for all patients and for different patient subgroups.
Safety and terminations of treatment
Few adverse events were associated with the use of preservative-free tafluprost. A total of 567 patients (97.9%) completed the study and continued preservative-free tafluprost monotherapy. Four patients (0.9%) terminated the treatment due to a lack of efficacy, two patients of their own volition, and one patient each (0.2%) in each case due to conjunctival hyperemia, conjunctival headache and increased contrast sensitivity. Further details on adverse events and terminations of treatment are shown in .
Table 4 Adverse events and terminations of treatment
Discussion
A large body of evidence exists showing that the long-term use of topical drugs containing BAK as a preservative may induce changes to the ocular surface, tear film instability, epithelial apoptosis, conjunctival inflammation, and the loss of goblet cells.Citation14–Citation18 Different studies have also confirmed that the prevalence of ocular surface disorders is high in glaucoma patients: in a study by Leung et al, 59% of patients with open-angle glaucoma or OH reported dry eye symptoms in at least one eye.Citation24 In another study by Erb et al, dry eye syndrome was diagnosed in 52.6% of glaucoma patients.Citation25 In both studies, the occurrence of dry eye syndrome increased with the number of preservative-containing anti-glaucoma drugs used. With respect to local tolerability of glaucoma medications, clinical studies report that a high proportion of glaucoma patients developed subjective symptoms such as burning and stinging, foreign body sensation, dry eye, and irritation of the ocular surface; these subjective symptoms were reported significantly less often in patients receiving preservative-free preparations.Citation19–Citation21
All these aspects are of importance when considering the treatment of treatment-naive glaucoma and OH patients in order to avoid any changes to the ocular surface and tear film induced by exposure to BAK during long-term treatment.
The results of this noninterventional, open-label, multicenter observational study demonstrate that preservative-free tafluprost can achieve good IOP control in treatment-naive patients and that the drug is well tolerated: after initiation of medical treatment with the preservative-free PGA, mean IOP decreased significantly by 6.8 mmHg (28.8%) until final visit at month 3 in all patients. Mean IOP also decreased significantly in all subgroups of patients with POAG/OH, NTG, PEX, and other glaucomas: in patients with NTG, mean IOP decreased by 3.3 mmHg from 16.6 mmHg to 13.3 mmHg. This is slightly higher than the findings of a randomized, crossover study, in which tafluprost lowered IOP by 2.3 mmHg from 15.5 mmHg to 13.2 mmHg after 12 weeks and travoprost by 2.2 mmHg from 15.4 mmHg to 13.2 mmHg.Citation29 However, it should be noted that the baseline IOP levels in the present study were higher, which may have had an impact on the IOP decrease.
Ang et al reported a decrease in mean IOP in naive patients with NTG after treatment with latanoprost from 16.9 to 14.1 mmHg (17%).Citation30 Another study found a decrease in average IOP of 1.98 mmHg (16.1%) in treatment-naive patients with NTG after medical treatment with travoprost 0.004%.Citation31 Suh et al reported a decrease in IOP of 2.71 to 3.71 mmHg (18.3% to 25.1%) in patients with NTG treated with travoprost over 12 months.Citation32 Tsumura et al reported a decrease in mean IOP of 3.9 mmHg in NTG patients from 14.5 to 10.6 mmHg after 12 weeks treatment with bimatoprost; a 20% decrease from baseline was seen in about half of the subjects.Citation33 This is consistent with our finding of a ≥20% IOP reduction in 53.5% of NTG patients treated with preservative-free tafluprost. In a 3-month study comparing the IOP-lowering efficacy of bimatoprost and latanoprost in patients with NTG, Dirks et al found a reduction in mean IOP of 3.4 mmHg with bimatoprost and 2.3 mmHg with latanoprost. In their study, mean baseline IOP values were 17.2 mmHg in the bimatoprost and 16.2 mmHg in the latanoprost treatment arm.Citation34 Two other studies found a decrease in IOP from a baseline IOP level of 13.9 mmHg by 2.5 mmHg and 2.6 mmHg for latanoprost and travoprost, respectively, and 2.6 mmHg for travoprost from a baseline IOP level of 12.9 mmHg.Citation35,Citation36
There are few reports on the effects of PGAs in patients with PEX. In a study by Konstas et al, the efficacy and safety of latanoprost and travoprost were compared in PEX patients with IOP values > 24 mmHg. After 8 weeks of treatment, mean 24-hour IOP was lowered from 25.1 ± 2.5 mmHg at baseline to 17.8 ± 2.1 mmHg on latanoprost (−7.3 mmHg) and from 25.1 ± 2.5 mmHg at baseline to 17.9 ± 2.1 mmHg (−7.2 mmHg) on travoprost.Citation37 Another study comparing bimatoprost and latanoprost in patients with PEX found a reduction in mean IOP from 26.9 ± 3.5 mmHg at baseline to 17.6 ± 3.3 mmHg (−9.3 mmHg) in the bimatoprost treatment arm and to 18.6 ± 3.6 mmHg (−8.3 mmHg) in the latanoprost treatment arm.Citation38 In the present observational study, preservative-free tafluprost lowered the mean IOP in patients with PEX from 25.8 ± 3.5 mmHg at baseline to 17.5 ± 2.4 mmHg (−8.3 mmHg) at month 3, which is in a comparable range with the published data for latanoprost, travoprost, and bimatoprost.
Uveoscleral outflow seems to be reduced in patients with exfoliation syndrome.Citation39 This may, at least in part, explain the excellent IOP response of patients with PEX to PGAs, as seen in this study. However, it also should be noted that mean baseline IOP in this patient subgroup was more than 1 mmHg higher than in other patient subgroups. A higher baseline IOP might affect the absolute and percentage IOP-lowering efficacy of glaucoma medications, as can be seen in the present study in the POAG and OH subgroups. As would be expected, absolute and percentage IOP reductions were greater in patients with POAG and OH with higher baseline IOP values (≥24 mmHg). Several other studies have reported that higher baseline IOP levels are associated with larger IOP reductions.Citation40,Citation41 This finding may partly be explained by a regression to the mean. However, in the present study, significant IOP responses to preservative-free tafluprost were seen in both subgroups of patients with POAG and OH stratified by baseline IOP levels: IOP levels ≤ 18 mmHg were achieved by 61.7%, 98.6%, 66.7%, and 66.7% of patients with POAG/OH, NTG, PEX, and other glaucomas, respectively. Also, when stratified by untreated IOP levels in patients with POAG or OH, IOP levels ≤ 18 mmHg were achieved by 80.2% and 61.7% in the ≥20 to 23 mmHg and ≥24 mmHg patient subgroups, respectively. Further, more than 94% of patients in both subgroups achieved IOP reductions ≥ 10% at month 3. These findings are consistent with a meta-analysis of studies with latanoprost in patients with glaucoma and OH showing IOP reductions > 15% in 93% of patients.Citation40 Denis et al reported a ≥10% reduction of IOP in 94% of patients with POAG and OH treated with latanoprost.Citation41
Various studiesCitation42–Citation46 have reported preservative-free tafluprost to be well tolerated and safe and we found this to be true in our study also. In the present study, only twelve patients (2.1%) terminated their medical treatment during the research period. Conjunctival hyperemia occurred in four patients (0.7%), which was fewer than in a previous study comparing latanoprost, bimatoprost, and travoprost in treatment-naive patients. In that study, hyperaemia rates of 12.5 and 17.5% were reported for patients treated with bimatoprost, 4.8 and 7.1% of patients treated with latanoprost, and 17.5 and 10% of patient treated with travoprost after 2 and 6 months respectively.Citation47 The lower rate of conjunctival hyperemia may be explained by the preservative-free formulation of tafluprost and a lower concentration of the active ingredient tafluprost.
While the present study is limited by its open-label design, the design may better reflect the treatment algorithms of day-to-day practice. Due to its observational nature, no causal relationships were revealed. Further, regression to the mean cannot be ruled out. Further well-controlled clinical studies are necessary to determine which aspects of preservative-free therapy with tafluprost may account for the observed effects.
Conclusion
In this study, preservative-free tafluprost 0.0015% was efficacious, well tolerated, and safe in treatment-naive patients. IOP response was generally good in all subgroups of patients and in both subgroups of patients with POAG and OH stratified by untreated baseline IOP levels; IOP was lowered effectively in all subgroups of patients. IOP reductions in the subgroup of patients with POAG and OH were smaller in patients with lower baseline IOP (≥20 to 23 mmHg) than in patients with higher baseline IOPs (≥24 mmHg). Preservative-free tafluprost was well tolerated; few ocular side effects were noted during the study period. Conjunctival hyperemia was observed in four patients (0.7%). Moreover, treatment with preservative-free tafluprost was safe. Few patients terminated therapy due to lack of efficacy (four patients; 0.7%) and adverse events (eight patients; 1.4%). Thus, our data suggest that preservative-free tafluprost may be especially beneficial for treatment-naive patients in order to avoid treatment-related side effects induced by treatments containing preservatives.
Disclosure
This study was financially supported by Santen Oy, Tampere, Finland. I Lanzl is a speaker for Santen Oy and F Kimmich is a consultant for Santen Oy. Medical writing, data management, and statistical analysis of the present study were done by eyecons (F Kimmich), with financial support from Santen Oy. The authors declare no other conflicts of interest in this work.
References
- HeijlALeskeMCBengtssonBHymanLBengtssonBHusseinMEarly Manifest Glaucoma Trial GroupReduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma TrialArch Ophthalmol2002120101268127912365904
- The Advanced Glaucoma Intervention Study (AGIS): 7The relationship between control of intraocular pressure and visual field deterioration. The AGIS InvestigatorsAm J Ophthalmol2000130442944011024415
- KassMAHeuerDKHigginbothamEJThe Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucomaArch Ophthalmol2002120670171312049574
- The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucomaCollaborative Normal-Tension Glaucoma Study GroupAm J Ophthalmol199812644985059780094
- European Glaucoma SocietyTerminology and Guidelines for Glaucoma3rd edSavonaDogma2008
- BeanGWCamrasCBCommercially available prostaglandin analogs for the reduction of intraocular pressure: similarities and differencesSurv Ophthalmol200853 Suppl 1S69S8419038626
- NakajimaTMatsugiTGotoWNew fluoroprostaglandin F(2alpha) derivatives with prostanoid FP-receptor agonistic activity as potent ocular-hypotensive agentsBiol Pharm Bull200326121691169514646172
- TakagiYNakajimaTShimazakiAPharmacological characteristics of AFP-168 (tafluprost), a new prostanoid FP receptor agonist, as an ocular hypotensive drugExp Eye Res200478476777615037111
- SuttonAGouwsPRopoATafluprost, a new potent prostanoid receptor agonist: a dose-response study on pharmacodynamics and tolerability in healthy volunteersInt J Clin Pharmacol Ther200846840040618793581
- UusitaloHPillunatLERopoAPhase III Study InvestigatorsEfficacy and safety of tafluprost 0.0015% versus latanoprost 0.005% eye drops in open-angle glaucoma and ocular hypertension: 24-month results of a randomized, double-masked phase III studyActa Ophthalmol2010881121920420586
- TraversoCERopoAPapadiaMUusitaloHA phase II study on the duration and stability of the intraocular pressure-lowering effect and tolerability of Tafluprost compared with latanoprostJ Ocul Pharmacol Ther20102619710420148656
- KuwayamaYKomemushiSTafluprost Multi-center Study GroupIntraocular pressure lowering effect of 0.0015% tafluprost as compared to placebo in patients with normal tension glaucoma: randomized, double-blind, multicenter, phase III studyNihon Ganka Gakkai Zasshi20101145436443 Japanese20545217
- ChabiAVarmaRTsaiJCRandomized clinical trial of the efficacy and safety of preservative-free tafluprost and timolol in patients with open-angle glaucoma or ocular hypertensionAm J Ophthalmol201215361187119622310086
- BaudouinCSide effects of antiglaucomatous drugs on the ocular surfaceCurr Opin Ophthalmol199672808610163327
- VaedeDBaudouinCWarnetJMBrignole-BaudouinFPreservatives in eye drops: toward awareness of their toxicityJ Fr Ophthalmol2010337505524 French
- BrasnuEBrignole-BaudouinFRianchoLGuenounJMWarnetJMBaudouinCIn vitro effects of preservative-free tafluprost and preserved latanoprost, travoprost, and bimatoprost in a conjunctival epithelial cell lineCurr Eye Res200833430331218398704
- LiangHBaudouinCPaulyABrignole-BaudouinFConjunctival and corneal reactions in rabbits following short- and repeated exposure to preservative-free tafluprost, commercially available latanoprost and 0.02% benzalkonium chlorideBr J Ophthalmol20089291275128218723745
- KahookMYNoeckerRQuantitative analysis of conjunctival goblet cells after chronic application of topical dropsAdv Ther200825874375118670744
- JaenenNBaudouinCPouliquenPManniGFigueiredoAZeyenTOcular symptoms and signs with preserved and preservative-free glaucoma medicationsEur J Ophthalmol200717334134917534814
- PisellaPJPouliquenPBaudouinCPrevalence of ocular symptoms and signs with preserved and preservative free glaucoma medicationBr J Ophthalmol200286441842311914211
- NordmannJPAuzanneauNRicardSBerdeauxGVision related quality of life and topical glaucoma treatment side effectsHealth Qual Life Outcomes200317514667241
- ZimmermanTJHahnSRGelbLTanHKimEEThe impact of ocular adverse effects in patients treated with topical prostaglandin analogs: changes in prescription patterns and patient persistenceJ Ocul Pharmacol Ther200925214515219284321
- AriasASchargelKUssaFCanutMIRoblesAYSánchezBMPatient persistence with first-line antiglaucomatous monotherapyClin Ophthalmol2010426126720463793
- LeungEWMedeirosFAWeinrebRNPrevalence of ocular surface disease in glaucoma patientsJ Glaucoma200817535035518703943
- ErbCGastUSchremmerDGerman register for glaucoma patients with dry eye. I. Basic outcome with respect to dry eyeGraefes Arch Clin Exp Ophthalmol2008246111593160118648841
- BaudouinCRenardJPNordmannJPPrevalence and risk factors for ocular surface disease among patients treated over the long term for glaucoma or ocular hypertensionEur J Ophthalmol Epub June 11, 2012
- LawinMJWormaldRPMigdalCSHitchingsRAThe influence of prior therapy on the success of trabeculectomyArch Ophthalmol199010811154315482244836
- Santen Oy Taflotan® [summary of product characteristics]TampereSanten Oy2008
- MizoguchiTOzakiMUnokiKDakeYEtoTAraiMA randomized crossover study comparing tafluprost 0.0015% with travoprost 0.004% in patients with normal-tension glaucoma [corrected]Clin Ophthalmol201261579158423055682
- AngAReddyMAShepstoneLBroadwayDCLong term effect of latanoprost on intraocular pressure in normal tension glaucomaBr J Ophthalmol200488563063415090413
- AngGSKerseyJPShepstoneLBroadwayDCThe effect of travoprost on daytime intraocular pressure in normal tension glaucoma: a randomised controlled trialBr J Ophthalmol20089281129113318511540
- SuhMHParkKHKimDMEffect of travoprost on intraocular pressure during 12 months of treatment for normal-tension glaucomaJpn J Ophthalmol2009531182319184304
- TsumuraTYoshikawaKSuzumuraHBimatoprost ophthalmic solution 0.03% lowered intraocular pressure of normal-tension glaucoma with minimal adverse eventsClin Ophthalmol201261547155223055677
- DirksMSNoeckerRJEarlMRohSSilversteinSMWilliamsRDA 3-month clinical trial comparing the IOP-lowering efficacy of bimatoprost and latanoprost in patients with normal-tension glaucomaAdv Ther200623338539416912020
- SawadaAYamamotoTTakatsukaNRandomized crossover study of latanoprost and travoprost in eyes with open-angle glaucomaGraefes Arch Clin Exp Ophthalmol2012250112312921858678
- NomuraYNakakuraSMoriwakiMTakahashiYShirakiKEffect of travoprost on 24-hour intraocular pressure in normal tension glaucomaClin Ophthalmol2010464364720689776
- KonstasAGKozobolisVPKatsimprisIEEfficacy and safety of latanoprost versus travoprost in exfoliative glaucoma patientsOphthalmology2007114465365717197028
- KonstasAGHollóGIrkecMDiurnal IOP control with bimatoprost versus latanoprost in exfoliative glaucoma: a crossover, observermasked, three-centre studyBr J Ophthalmol200791675776017124241
- JohnsonTVFanSCamrasCBTorisCBAqueous humor dynamics in exfoliation syndromeArch Ophthalmol2008126791492018625936
- HedmanKAlmAA pooled-data analysis of three randomized, double-masked, six-month clinical studies comparing the intraocular pressure reducing effect of latanoprost and timololEur J Ophthalmol20001029510410887918
- DenisPBaudouinCBronAFirst-line latanoprost therapy in ocular hypertension or open-angle glaucoma patients: a 3-month efficacy analysis stratified by initial intraocular pressureBMC Ophthalmol201010420181282
- HommerAMohammed RamezOBurchertMKimmichFIOP-lowering efficacy and tolerability of preservative-free tafluprost 0.0015% among patients with ocular hypertension or glaucomaCurr Med Res Opin20102681905191320553122
- UusitaloHMPillunatLEBaudouinCPhase III, 24-month study investigating the efficacy and safety of tafluprost vs latanoprost in patients with open-angle glaucoma or ocular hypertensionActa Ophthalmol200886SupplS243
- HamacherTAiraksinenJSaarelaVLiinamaaMJRichterURopoAEfficacy and safety levels of preserved and preservative-free tafluprost are equivalent in patients with glaucoma or ocular hypertension: results from a pharmacodynamics analysisActa Opthtalmol Suppl (Oxf)2008S2421419
- UusitaloHChenEPfeifferNSwitching from a preserved to a preservative-free prostaglandin preparation in topical glaucoma medicationActa Ophthalmol201088332933620546237
- JanulevičienėIDerkačIGrybauskieneLPaulauskaitėRGromnickaiteRKuzmienėLEffects of preservative-free tafluprost on tear film osmolarity, tolerability, and intraocular pressure in previously treated patients with open-angle glaucomaClin Ophthalmol2012610310922275814
- FaridiUASalehTAEwingsPComparative study of three prostaglandin analogues in the treatment of newly diagnosed cases of ocular hypertension, open-angle and normal tension glaucomaClin Experiment Ophthalmol201038767868220456437