Abstract
We report here a patient with type 1 Duane’s retraction syndrome and multiple congenital abnormalities as a result of the VACTERL association. The presented combination of Duane’s retraction syndrome and the VACTERL association has not been reported in the literature. The present case was instructive for reviewing the continuous spectrum of ocular anomalies that accompany the VACTERL association.
Introduction
The VATER association was first described in 1973 as the nonrandom co-occurrence of five defects, ie, vertebral anomalies (V), anal atresia (A), esophageal atresia and/or trachea-esophageal fistula (TE) and radial and renal anomalies (R). Subsequently, cardiovascular anomalies (C) and limb defects (L) were also included defining the acronym VACTERL association.Citation1,Citation2 Although numerous syndromes associated with VACTERL have been identified the etiology remains unknown.Citation3,Citation4
Duane’s retraction syndrome is a congenital oculomotor anomaly that is accompanied by retraction of the globe and characterized by simultaneous narrowing of the palpebral fissure on attempted adduction, limitation of abduction, slight limitation of adduction, and elevation or depression of the globe during adduction.Citation5 Patients with Duane’s retraction syndrome have a 10–20 times greater risk of having other congenital malformations.Citation6
In the present report, we describe the unusual occurrence of type 1 Duane’s retraction syndrome with multiple congenital abnormalities due to the VACTERL association.
Case report
A 2-year-old child was referred to the Strabismus Department at the Prof Dr N Reşat Belger Beyoglu Education and Research Eye Hospital for evaluation of strabismus. This female infant was the first child of nonconsanguinous parents, and her family history was negative for congenital anomalies. The mother was 29 years old and the father was 30 years old. The mother had no history of diabetes or exposure to teratogenic agents, such as lead lovastatin, dibenzepin, or exogenous sex hormones. There was no history of smoking, alcohol, drug abuse, or any infectious disease. The child who had a normal prenatal ultrasound at 14 weeks’ gestation, was born after an otherwise uncomplicated pregnancy. A triple test was not performed on the mother during her pregnancy. A cesarean section was performed at 38 weeks. The infant’s weight and length at birth were 2720 g and 44 cm, respectively. Her head circumference was not measured at that time.
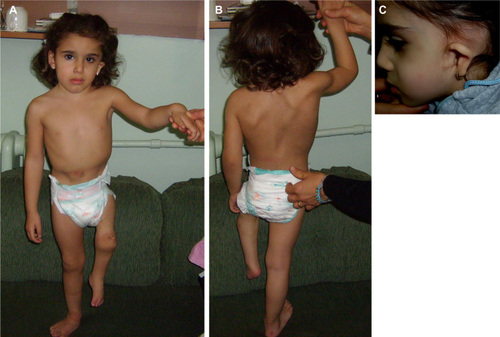
At the pediatric surgery consultation, a perineal fistula, anterior anal ectopia, and anal stenosis were detected. Renal problems included a crossed fused renal ectopic duplicate kidney on the left side, renal agenesis on the right side (on intravenous pyelogram), and grade 2 vesicoureteral reflux (on voiding cystourethrogram). At the neurological consultation, the motor function of the upper extremities was normal, but a motor deficit was determined in the left lower extremity. Left ankle plantar flexion and dorsiflexion were 0/5 with an absent Achilles reflex. Magnetic resonance imaging of the cervical and dorsolumbar spine revealed partial fusion of the D5-D6 vertebrae, hemivertebrae and partial fusion of L4-L5-S1, scoliosis (dorsolumbar to right, lumbosacral to left), spina bifida at the L4-S1 level, a tethered spinal cord combined with intradural lipoma at the L3-L4 level, and syringomyelia at the L2-L3 level. Major limb malformation included shortness of the left lower limb, primarily due to hypoplasia of the stylopod and zeugopod, hypoplasia of muscles, and subcutaneous fatty tissue in these two parts, pes equinovarus on the left side, and impaired movement of the left genu with a 90º flexion contracture of the left knee, and a hypoplastic thumb and fingers on the left side. A radiographic evaluation confirmed the previously identified malformations and also demonstrated a short tibia and femur, malformed carpal bones, and hypoplasia of all skeletal components of the second ray on the left lower limb. Dysgenesis of the left hemipelvis and sacrum, dysplasia of the left femur, and hypoplasia of muscles in the front and back of thigh were identified on magnetic resonance imaging of the hip ( and ). She had low-set microtia on the left side (); furthermore, pure tone audiometry revealed a 60 dB hearing level in the left ear and a normal range of hearing in the right ear. An echocardiogram did not show any intracardiac anomalies.
Figure 1 (A) Front view of the patient, showing facial asymmetry, pes equinovarus on the left side, a 90 degree flexion contracture of the left knee, and marked shortness of the lower limb. Hypoplasia of the muscles and subcutaneous fat in the stylopod with overt reduction of the limb circumference were also noted. (B) Back view of the patient, showing scoliosis and tethered cord. (C) A low-set left ear and atretic pinna (left microtia).
The patient and her family were referred to the Department of Medical Genetics. The girl had a normal female karyotype (46, XX) in cultured blood lymphocytes. Her chromosomal analysis, based on 400–550 bands per haploid karyotype, did not reveal any abnormalities. There was no family history of eye or genetic defects, and her parents’ karyotypes were normal. She had no chromosomal abnormalities or known genetic disorders, such as Fanconi syndrome, Feingold syndrome, Baller-Gerold syndrome, or germline mutation in the PTEN gene.
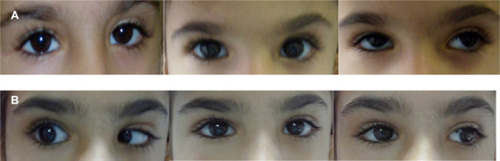
The ophthalmic examination revealed a corrected visual acuity of 16/20 in the right eye and 20/20 in the left eye. The pupils were equal, round and reactive to light, with no evidence of a relative afferent pupillary defect. The cycloplegic refraction value was +3.50, −1.00 á 15° in the right eye and +3.75, −1.00 á 40° in the left eye. On motility examination, we determined 15 Δ esotropia via the Krimsky method. Slit-lamp biomicroscopy revealed normal anterior and posterior segments in both eyes. The intraocular pressures were normal. The patient had a −2 restriction on right abduction, narrowing of the palpebral fissures, globe retraction, and upshoot on attempted adduction. The other versions and ductions were normal. The patient exhibited facial asymmetry. The ophthalmological examination revealed type 1 Duane’s retraction syndrome in the right eye ().
Figure 2 Right type 1 Duane’s syndrome. (A) Preoperative appearance (−2 restriction on abduction, narrowing of the palpebral fissures, globe retraction, and upshoot on attempted adduction of right eye). (B) Postoperative appearance (−1 restriction of right abduction, no globe retraction or upshoot, orthotropic in primary position).
At 5 months of age, the infant underwent surgery for her tethered cord. At one year of age, she underwent an operation for flexion contracture of her left knee. The patient received a staged reconstruction surgery under colostomy. She underwent anal transposition surgery and posterior sagittal anorectoplasty at 18 months of age. The colostomy remained open until healing from the posterior sagittal anorectoplasty was achieved. After healing was completed the colostomy was closed. The patient had lack of continence which improved after the surgery. At 4 years of age, she underwent a left ear operation.
Strabismus surgery was performed when the patient was 2 years of age, with no complications. She underwent a right medial rectus recession (5 mm) operation. Postoperatively, the patient was orthotropic in the primary position. She had no globe retraction or upshoot on attempted adduction and a −1 restriction of right abduction ().
Discussion
The VATER association describes a rare condition characterized by a sporadic combination of specific birth defects. The VATER or VACTERL association (an acronym for vertebral defects, anorectal malformations, cardiac defects, tracheo-esophageal fistulas, renal anomalies, and limb anomalies) represents a statistically related pattern of associated anomalies. The diagnosis of a VACTERL association is made when three or more features of the association are present.Citation3 The most commonly associated anomalies in these patients are anorectal malformations (55%–90%), tracheo-esophageal fistulas (50%–80%), renal anomalies (50%–80%), vertebral anomalies (36%–80%), cardiac anomalies (40%–80%), and limb anomalies (40%–50%).Citation7,Citation8 Lower limb defects do occur in the VATER association but are far less frequent than upper limb defects.Citation9 Our case displayed four characteristics of the VACTERL association, including anorectal, renal, vertebral, and lower limb defects. In addition, she had auricular atresia of the left ear. Vertebral anomalies can occur in any segment of the spine and may be associated with neurologic abnormalities.Citation10 Our patient had tethered cord syndrome. In this syndrome, neurological deficits are generally irreversible. In children, early surgery is recommended to prevent further neurological deterioration.Citation11–Citation13 We determined some neurological deficits early, so we performed tethered cord surgery at 5 months of age.
Although numerous etiologies are known to be responsible for the VATER/VACTERL association, the pathogenesis remains unknown in the majority of cases.Citation2 This association has also been described as the result of teratogenic exposures, such as lead, lovastatin, dibenzepin, maternal diabetes, exogenous sex hormones, chromosomal abnormalities such as Del(6)q, 9qh+, supernumerary ring chromosome, and Del(13)(q31.1qter), and known genetic disorders such as Fanconi syndrome, Feingold syndrome, Baller-Gerold syndrome, and germline mutation in the PTEN gene.Citation14–Citation22 A primary developmental field defect resulting from failure of mesodermal cell migration during early blastogenesis ie, during the first 4 weeks of development has been suspected,Citation3,Citation4 as well as a multifactorial origin.Citation23 However, in our case, no teratogenic exposures, chromosomal abnormalities, or known genetic disorders could be recognized. The rare familial occurrence of VATER/ VACTERL association is in favor of a genetic origin with either autosomal dominant or recessive mode of inheritance.Citation24 Moreover, recently, the observation of VATER/VACTERL association in a Gli mutant mouse has suggested that impairment of the sonic hedgehog pathway could also be responsible for this phenotype.Citation25 Some authors have reported that the VATER/VACTERL association has been described as a result of respiratory chain deficiency.Citation2
Patients with the VACTERL association have eye defects.Citation26 Their ophthalmic findings include ptosis, strabismus, myopia, hypermetropia, amblyopia, anisometropia, cloudy corneas, microcornea, congenital corneal anesthesia (ie, recurrent erosions, keratitis, ulcers, and leukomas), anisocoria and heterochromia iridis, cataracts, and lacrimal system abnormalities.Citation26–Citation28 The most common associations are coloboma and microphthalmos.Citation27 The retina and posterior segment are seldom involved. A unique case of Coats’ disease combined with the VATER association has been reported.Citation29 To our knowledge, there have been no reports of a patient with Duane’s retraction syndrome and the VACTERL association. In the present case study, we report the unusual occurrence of type 1 Duane’s retraction syndrome in a child with the VACTERL association. Duane’s retraction syndrome is a congenital disorder of eye motility. The pathogenetic mechanism of this syndrome is abnormal rectus innervation of the affected eye by axons that are destined for the medial rectus.Citation5,Citation6 Genetic and environmental factors may be responsible for Duane’s retraction syndrome,Citation6 but these causes had been ruled out in our case. The gene responsible for the gene has been mapped to 8q13.3.Citation30 Specification of mammalian motor neurons and mutations in the Pax 6 gene may be responsible for the aberrant innervation in Duane’s retraction syndrome.Citation31 The Pax gene family consists of developmental control genes and plays an important role in the development of the vertebral column, genitourinary tract, and central nervous system.Citation32 In our patient, chromosomal analysis did not reveal any aberrations. In the majority of cases of VACTERL association, the pathogenesis remains unknown.Citation3,Citation4
In conclusion, our patient presented an unusual combination of Duane’s retraction syndrome and VACTERL association, which has not been previously reported. This case is instructive for reviewing the continuous spectrum of ocular anomalies that accompany the VACTERL association. The cause of the association between VATER/VACTERL and Duane syndrome is not clear, but these two syndromes might be the result of defective mesodermal development during embryogenesis.
Acknowledgments
The authors would like to acknowledge the generous and helpful assistances of Serdar Sander from the Department of Pediatric Surgery, Istanbul Kanuni Sultan Süleyman, Training and Research Hospital, and Serdar Cevik, from the Department of Neurosurgery, Medical Faculty, Bezmi Alem Foundation University. The authors obtained parental consent to use the images shown.
Disclosure
The authors report no conflicts of interest in this work.
References
- QuanLSmithDWThe VATER association. Vertebral defects, anal atresia, T-E fistula with esophageal atresia, radial and renal dysplasia: a spectrum of associated defectsJ Pediatr1973821041074681850
- Thauvin-RobinetCFaivreLHuetFAnother observation with VATER association and a complex IV respiratory chain deficiencyEur J Med Genet200649717716473312
- Martinez-FriasMLFriasJLVACTERLY as primary, polytopic developmental field defectsAm J Med Genet199983131610076879
- Martinez-FriasMLFriasJLPrimary developmental field III: clinical and epidemiological study of blastogenetic anomalies and their relationship to different MCA patternsAm J Med Genet19977011159129734
- Von NoordenGKCamposESpecial forms of strabismusBinocular Vision and Ocular Motility: Theory and Management of Strabismus6th edSt Louis, MOMosby2002
- PfaffenbachDDCrossHEKearnsTPCongenital anomalies in Duane’s retraction syndromeArch Ophthalmol1972886356394628563
- ChittmittrapapSSpitzLKielyEMOesophageal atresia and associated anomaliesArch Dis Childhood1989643643682705799
- SolomonBDVACTERL/VATER associationOrphanet J Rare Dis201165621846383
- FernbachSKGlassRBJThe expanded spectrum of limb anomalies in the VATER associationPediatr Radiol1988182152203368246
- BarnesJCSmithWLThe VATER associationRadiology1978126445449622495
- BoopFARussellAChadduckWMDiagnosis and management of the tethered cord syndromeJ Ark Med Soc1992893283311286983
- IskandarBJFulmerBBHadleyMNOakesWJCongenital tethered spinal cord syndrome in adultsJ Neurosurg1998889589619609288
- van LeeuwenRNotermansNCVandertopWPSurgery in adults with tethered cord syndrome: outcome study with independent clinical reviewJ Neurosurg20019420520911302621
- LevineFMuenkeMVACTERL association with high prenatal lead exposure; similarities to animal models of lead teratogenicityPediatrics1991873903922000280
- GhidiniASichererSWillnerJCongenital abnormalities (VATER) in a baby born to a mother using lovastatinLancet1992339141614171350826
- MerlobPNaorNDrug induced VATER association: is dibenzepin a possible cause?J Med Genet1994314237914930
- LoffredoCAWilsonPDFerenczCMaternal diabetes: an independent risk factor for majör cardiovascular malformations with increased mortality of affected infantsTeratology2001649810611460261
- KaufmannRLBirth defects and oral contraceptivesLancet197311396
- CintiRPrioloMLeroneMMolecular characterisation of a supernumerary ring chromosome in a patient with VATER associationJ Med Genet2001381411134233
- McNealRMSkoglundRRFranckeUCongenital anomalies including the VATER association in a patient with a del(6)q deletionJ Pediatr197791957960925830
- CelliJvan BokhovenHBrunnerHGFeingold syndrome: clinical review and genetic mappingAm J Med Genet A2003122A29430014518066
- ReardonWZhouXPEngCA novel germline mutation of the PTEN gene in a patient with macrocephaly, ventricular dilatation, and features of VATER associationJ Med Genet20013882082311748304
- KhouryMJCorderoJFGreenbergFA population study of the VACTERL association: evidence for its etiologic heterogeneityPediatrics1983718158206835768
- AuchterlonieIAWhiteMPRecurrence of the VATER association: within a sibshipClin Genet1982211221247083612
- Martínez-FriasMLBermejoEFriasJLThe VACTERL association: lessons from the sonic hedgehog pathwayClin Genet20016039739811903345
- SayBGreenbergDHarisRDelongSLColdwellJGThe radial dysplasia/imperforate anus/vertebral anomalies syndrome (the VATER association): developmental aspects an deye findingsActa Paediatr Scand197766233235842344
- KallenKRobertECastillaEEMastroiacovoPKallenBRelation between oculo-auriculo-vertebral (OAV) dysplasia and three other non-random associations of malformations (VATER, CHARGE, and OEIS)Am J Med Genet A2004127A263415103713
- HarrisonARDaileyRAWobigJLBilateral congenital lacrimal anlage ducts (lacrimal fistula) in a patient with the VACTERL associationOphthal Plast Reconstr Surg200218149150
- HonCKoTCCoats disease and VATER association in a 5-year-old boyArch Ophthalmol20041221232123315302670
- OMIM™Mendelian Inheritance in Man. MIM Number 126800Baltimore, MDJohns Hopkins University2004 Available from: http://www.ncbi.nlm.nih.gov/omim/Accessed February 22, 2013
- OsumiNHirotaAOhuchiHPax-6 is involved in the specification of hindbrain motor neuron subtypeDevelopment1997124296129729247338
- StrachanTReadAPPax genesCurr Opin Genet Dev199444274387919921