Abstract
A decrease in the anterior capsule opening after cataract surgery has been observed in eyes with weakened lens zonules. It commonly occurs in diabetes mellitus, uveitis, pseudoexfoliation syndrome, high myopia, and elderly patients. Herein, we report the case of a middle-aged man with advanced retinitis pigmentosa who developed a rapid contraction of the anterior capsule after an uneventful phacoemulsification surgery that resulted in severe visual loss during the early postoperative period.
Introduction
Patients with retinitis pigmentosa are more predisposed to suffer from specific risk factors during cataract surgery. These include phototoxic retinal damage during the surgery,Citation1–Citation3 postoperative macular oedema,Citation2,Citation4–Citation6 and posterior capsular opacification.Citation7–Citation11 These conditions may result in poor visual acuity in patients with retinitis pigmentosa following the cataract surgery.
This case report highlights a rare occurrence of an aggressive anterior capsular contraction after an uneventful elective phacoemulsification surgery in a middle-aged man suffering from advanced retinitis pigmentosa. This resulted in significant visual loss during the early postoperative period.
Case report
A 49-year-old man presented with progressive, painless blurring of vision in both eyes. His best-corrected visual acuity was 6/18 in both eyes. Slit-lamp biomicroscopic examination revealed posterior subcapsular cataract in both eyes. Fundus examination revealed the presence of a hyperpigmented bony spicule in the retina, attenuated arterioles, slightly pale optic discs, and dull foveal reflex in both eyes. Intraocular pressure was normal bilaterally. Humphrey 30-2 SITA fast visual field perimetry revealed concentric contraction with generalized depression of sensitivity in both eyes.
He was advised to undergo phacoemulsification cataract surgery and provided an explanation of guarded postoperative visual outcome. He underwent the phacoemulsification surgery and implantation of a CT-Asphina® 603P (Carl Zeiss Meditec, Jena, Germany) intraocular lens under sub-Tenon anesthesia in the right eye. The surgery was uneventful. His visual acuity was found to have improved to 6/15 on the first postoperative day.
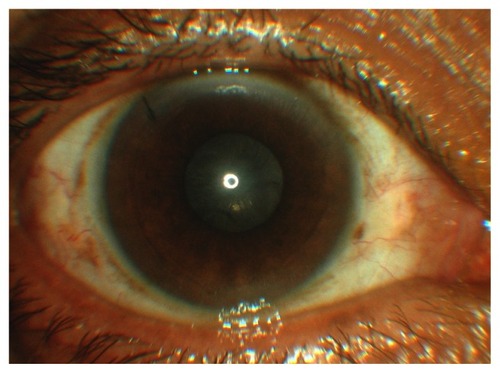
However, the patient complained of significant, painless blurring of vision in the operated eye at 2-weeks post-surgery. On examination, his visual acuity was found to have reduced to counting fingers. The anterior capsule was markedly thickened, with a near total visual axis occlusion (). The intraocular lens remained stable and enclosed centrally in the capsular bag. The fundus view was poor, and a B-scan of the right eye revealed clear vitreous and a flat retina.
Figure 1 Anterior segment photograph showing anterior capsular contraction causing a near total occlusion of the visual axis.
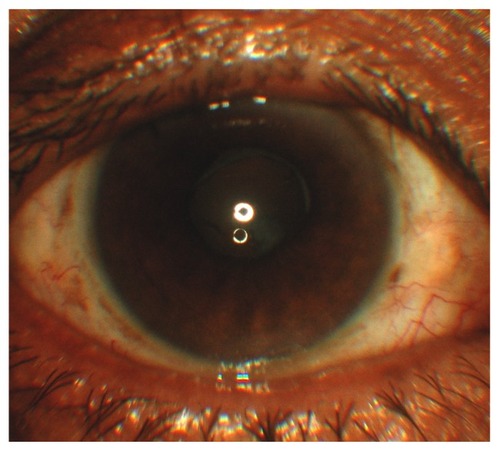
A neodymium-doped yttrium aluminum garnet (Nd:YAG) laser anterior capsulotomy was performed under local anesthesia on the affected eye, and this resulted in improvement of the patient’s visual acuity to 6/15 2-weeks later. The visual axis was cleared (). The patient was monitored at regular intervals following this.
Figure 2 Anterior segment photograph showing a clear visual axis after laser anterior capsulotomy.
Subsequently, he underwent an elective phacoemulsification surgery and AcrySof® IQ posterior chamber lens (Alcon, Hünenberg, Switzerland) implantation under sub-Tenon anesthesia in the other eye 6 months after surgery. The surgery was uneventful. A larger capsulorhexis of approximately 6 mm with multiple sites of radial incisions was performed intraoperatively. His postoperative visual acuity was 6/12. He was examined closely during the postoperative period and his visual axis remained unaffected.
The patient was last seen 2 months after the operation. His best-corrected visual acuity was 6/9 in both eyes. Refraction result showed +0.50/−0.50 × 170 for the right eye and plano/−0.75 × 110 in the left eye. There was no sign of anterior capsular contraction in the left eye.
Discussion
According to our search of the PubMED and MEDLINE databases, there are few published case reports regarding contraction of the anterior capsule following cataract surgery in patients with retinitis pigmentosa.Citation7–Citation11 The occurrence of anterior capsule contraction or phimosis has been reported, ranging from months to years after uneventful cataract surgery.Citation7,Citation8,Citation10,Citation11 It is alarming to note that our patient and Nikpoor and Stone’sCitation9 patient developed this similar problem less than a month following surgery.
It is presumed that the etiology of anterior capsule contraction in retinitis pigmentosa patients involves an imbalance between the centrifugal forces of the zonules and the forces of the intraocular lens haptics, and the centripetal forces of the proliferative and metaplastic residual lens epithelial cells.Citation12 The anterior cuboidal lens epithelial cells undergo metaplasia with myofibroblastic transformation. These altered cells contain smooth-muscle actin and contraction results in fibrous membrane formation.
Our patient developed the anterior capsule contraction 2 weeks after surgery, and was treated with anterior Nd:YAG capsulotomy. He showed a satisfactory visual acuity in the affected eye after the treatment. We postulate that a relatively smaller capsulorhexis facilitated the anterior capsule contraction in the affected eye.
The occurrence of rapid anterior capsule opacification in his right eye had warned us regarding the possibility of a similar problem occurring in the contralateral eye. Early anticipation and relevant preventive measures were therefore our main concern before proceeding with surgery in the contralateral eye.
Interestingly, Nikpoor and Stone reported a fairly similar presentation to our case.Citation9 They described a 43-year-old man with retinitis pigmentosa who suffered from rapid anterior capsular contraction in each eye within 3 weeks following an uncomplicated phacoemulsification with continuous curvilinear capsulorhexis and a single-piece acrylic intraocular lens implantation.Citation9 The anterior YAG capsulotomy was successfully performed in both eyes of their patient.
Both our patient and Nikpoor and Stone’s patient did not display signs of intraocular lens instability. This suggests that early diagnosis of this condition is extremely important. We postulate that the severity and chronicity of this condition can lead to decentration, subluxation, and even spontaneous dislocation of the intraocular lens, as described by other authors.Citation7,Citation8,Citation10,Citation11
Larger capsulorhexis size,Citation7,Citation13–Citation15 use of a capsular tension ring,Citation16,Citation17 proper selection of intraocular lens,Citation18,Citation19 careful capsular lens epithelial cell clean-up,Citation20–Citation22 and radial relaxing incisions in the anterior lens capsuleCitation9,Citation23,Citation24 have all been advocated as effective measures to prevent or limit the occurrence of anterior capsule contraction.
The CT-Asphina 603P lens was implanted in our patient’s right eye. The lens remained stable despite the development of a rapid anterior capsule opacification in the affected eye. In contrast, Lam and Visvaraja reported recently that five patients had spontaneous lens dislocations following uneventful phacoemulsification surgeries and CT-Asphina 603P posterior chamber lens implantation.Citation25 However, their patients did not display significant capsular fibrosis.
We implanted an AcrySof IQ lens during subsequent surgery on the patient’s left eye. The visual axis remained clear during his follow-up visits. A larger capsulorhexis and multiple radial incisions seemed helpful in preventing the occurrence of rapid anterior capsular contraction in this eye.
Conclusion
It remains a rare occurrence, but it is crucially important to highlight to ophthalmologists that anterior capsular contraction must be prevented in retinitis pigmentosa patients, as it may result in severe visual loss and problems with intraocular lens instability after cataract surgery.
Disclosure
The authors declare no conflicts of interest in this work.
References
- LeeBLStenbergJPMicroscope light toxicitySemin Ophthalmol199382151155
- JacksonHGarway-HeathDRosenPBirdACTuftSJOutcome of cataract surgery in patients with retinitis pigmentosaBr J Ophthalmol200185893693811466249
- CideciyanAVJacobsonSGAlemanTSIn vivo dynamics of retinal injury and repair in the rhodopsin mutant dog model of human retinitis pigmentosaProc Natl Acad Sci U S A2005102145233523815784735
- TakezawaMTetsukaSKakehashiATangential vitreous traction: a possible mechanism of development of cystoid macular edema in retinitis pigmentosaClin Ophthalmol2011524524821386918
- FetkenhourCLChoromokosEWeinsteinJShochDCystoid macular edema in retinitis pigmentosaTrans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol1977833 Pt 1OP515OP521
- FishmanGAMaggianoJMFishmanMFoveal lesions seen in retinitis pigmentosaArch Ophthalmol1977951119931996921578
- HayashiKHayashiHMatsuoKNakaoFHayashiFAnterior capsule contraction and intraocular lens dislocation after implant surgery in eyes with retinitis pigmentosaOphthalmology19981057123912439663228
- LeeHJMinSHKimTYBilateral spontaneous dislocation of intraocular lenses within the capsular bag in a retinitis pigmentosa patientKorean J Ophthalmol2004181525715255238
- NikpoorNStoneDURapid capsular phimosis in retinitis pigmentosaOphthalmic Surg Lasers Imaging20102941
- SudhirRRRaoSKCapsulorhexis phimosis in retinitis pigmentosa despite capsular tension ring implantationJ Cataract Refract Surg200127101691169411687372
- NajjarDMIgbreAOTsaiFFLate capsular bag contraction and intraocular lens subluxation in retinitis pigmentosa: a case reportJ Med Case Rep201156521320335
- DavisonJACapsule contraction syndromeJ Cataract Refract Surg19931955825898229711
- JooCKShinJAKimJHCapsular opening contraction after continuous curvilinear capsulorhexis and intraocular lens implantationJ Cataract Refract Surg19962255855908784631
- TaquriAHDevlinHCapsular phimosis following phacotrabeculectomyOphthalmic Surg Lasers Imaging200536324524815957483
- HayashiHHayashiKNakaoFHayashiFAnterior capsule contraction and intraocular lens dislocation in eyes with pseudoexfoliation syndromeBr J Ophthalmol19988212142914329930277
- TribusCAlgeCSHaritoglouCIndications and clinical outcome of capsular tension ring (CTR) implantation: A review of 9528 cataract surgeriesClin Ophthalmol200711656919668468
- GimbelHVSunRRole of capsular tension rings in preventing capsule contractionJ Cataract Refract Surg200026679179210991673
- ZambarakjiHJRauzSReynoldsAJoshiNSimcockPRKinnearPECapsulorhexis phymosis following uncomplicated phacoemulsification surgeryEye (Lond)199711Pt 56356389474309
- HayashiKHayashiHNakaoFHayashiFAnterior capsule contraction and intraocular lens decentration and tilt after hydrogel lens implantationBr J Ophthalmol200185111294129711673291
- TadrosABhattUKAbdul KarimMNZaheerAThomasPWRemoval of lens epithelial cells and the effect on capsulorhexis sizeJ Cataract Refract Surg20053181569157416129293
- SacuSMenapaceRWirtitschMBuehlWRainerGFindlOEffect of anterior capsule polishing on fibrotic capsule opacification: three-year resultsJ Cataract Refract Surg200430112322232715519082
- HansonRJRubinsteinASarangapaniSBenjaminLPatelCKEffect of lens epithelial cell aspiration on postoperative capsulorhexis contraction with the use of the AcrySof intraocular lens: randomized clinical trialJ Cataract Refract Surg200632101621162617010857
- HayashiKYoshidaMHirataAHayashiHAnterior capsule relaxing incisions with neodymium:YAG laser for patients at high-risk for anterior capsule contractionJ Cataract Refract Surg20113719710321067893
- ZhangZDSongZChenDHuangFBilateral capsule contraction syndrome following pathological myopic cataract surgeriesInt J Ophthalmol20125340640822773998
- LamHHVisvarajaSSpontaneous dislocation of intraocular lens as a late complication of uncomplicated cataract surgery: a case seriesClin Exp Optom20129519910221954950