Abstract
Background
Macular edema (ME) is caused by abnormal retinal capillary permeability and has also been described as a postoperative complication of cataract surgery (Irvine-Gass syndrome).
Objective
To present a patient with Irvine-Gass syndrome in the right eye complicated with a macular hole (MH) in the same eye and possible associations between these two entities.
Case report
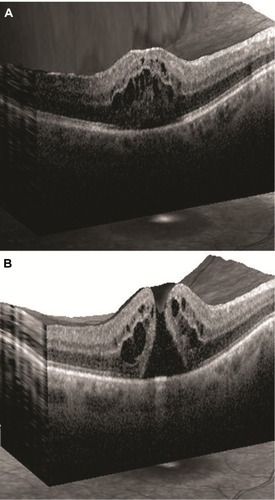
A 72-year-old male with a history of uneventful bilateral cataract surgery was followed-up with biomicroscopy and optical coherence tomography (OCT). Four weeks after cataract surgery oculus dexter (OD), there was progressive visual deterioration (best corrected visual acuity [BCVA]: 0.5). OCT disclosed cystoid ME. A parabulbar triamcinolone injection, dexamethasone 0.1% and ketorolac 0.4% eye drops, both 4 times per day OD were administered. Six weeks later (BCVA OD: 0.2), OCT revealed cystoid ME and full-thickness MH.
Conclusion
ME secondary to diabetes or central retinal vein occlusion may lead to MH by inducing focal vitreomacular traction and by triggering inflammatory mechanisms which facilitate a marked thinning of the fovea. MH may occur even in cases of pseudophakic ME, representing a rare complication of Irvine-Gass syndrome.
Introduction
Macular edema (ME) is thought to be caused by abnormal retinal capillary permeability. The resulting leakage has a detrimental effect on central retinal function, characterized by a varying decrease in visual acuity.Citation1 ME has been linked to diabetic retinopathy, retinal vein occlusion, and uveitis, while it has also been described as a postoperative complication of cataract extraction surgery (Irvine-Gass syndrome).Citation2 In this disorder, cystoid ME (CME) is observed and characterized by petalloid perifoveal leakage on fluorescein angiography.
A classification system focusing on anteroposterior and tangential vitreal traction on the foveal area as a principal cause for idiopathic macular holes (MHs) was proposed by Gass.Citation1 These tractional forces have been postulated to induce foveolar dehiscence, which facilitates hydration of middle and outer retinal layers, leading to edema and cell displacement.Citation3 Moreover, persistent vitreous adherence to the fovea coupled with shrinkage of prefoveal vitreous results in the causative traction. We present a patient with Irvine-Gass syndrome in the right eye complicated with an MH in the same eye and possible associations between these two entities.
Case report
A 72-year-old male patient underwent uneventful cataract surgery in the left eye (oculus sinister [OS]) in May 2009 and in the right eye (oculus dexter [OD]) in November 2009. No retinal pathology was present before surgery and the patient did not suffer from any systemic condition that may affect the retina. Best corrected visual acuity (BCVA) in both eyes (oculus uterque [OU]) was 1.0 1 week after each cataract extraction procedure. Four weeks following cataract surgery OD, the patient presented with progressive visual deterioration OD (BCVA OD: 0.5). Slit lamp examination did not reveal pathological findings OU; the intraocular lens (IOL) was symmetrically positioned in the capsular bag with no signs of capsule opacification. Optical coherence tomography (OCT) scans revealed CME (). No findings were observed OS. A parabulbar triamcinolone injection, dexamethasone 0.1% and ketorolac tromethamine 0.4% eye drops (4 times daily) were administered OD. Six weeks later (BCVA OD: 0.2), OCT scans revealed CME and a full-thickness MH (). Intravitreal bevacizumab administration and vitrectomy with internal limiting membrane peeling were discussed but the patient refused further management.
Figure 1 (A) Patient OCT scan depicting cystoid macular edema. (B) Patient OCT scan depicting cystoid macular edema and full-thickness macular hole (Grade IV).
Discussion
ME development depends on the associated disease with the common feature being the blood-retina barrier breakdown. During this process, Müller cells become swollen and are eventually lysed. This results in extracellular fluid accumulation in the outer plexiform and inner nuclear layers. Consequently, ME can be caused directly, due to endothelial cell damage, as it occurs in the context of diabetes mellitus and retinal vein occlusion and may lead to MH development.Citation4 MH formation may be induced by macular traction in combination with retinochoroidal atrophy in the context of recurring inflammation.Citation5
Full-thickness MH formation can be observed as early as 2 days following uncomplicated phacoemulsification.Citation6 In our case, CME was present 4 weeks postoperatively. It is conceivable that MH formation was initiated either by the conduction of phacoemulsification mechanical forces intraoperatively or by biochemical alterations postoperatively that resulted in localized vitreous liquefaction and subsequently traction. In this context, a sensible surgical strategy would be the intraoperative minimization of anterior chamber depth and capsular bag fluctuations with the use of relatively constant irrigation and aspiration settings. This could possibly result in reduced zonule damage during phacoemulsification and reduced conduction and application of mechanical forces to the macular area. Our case report suggests that MH formation may even occur in cases of pseudophakic ME, representing a rare complication of Irvine-Gass syndrome.
Disclosure
The authors report no conflicts of interest in this work.
References
- GassJDIdiopathic senile macular hole: its early stages and pathogenesis. 1988Retina200323Suppl 662963915035400
- KuppermannBDBlumenkranzMSHallerJADexamethasone DDS Phase II Study GroupRandomized controlled study of an intravitreous dexamethasone drug delivery system in patients with persistent macular edemaArch Ophthalmol2007125330931717353400
- TornambePEMacular hole genesis: the hydration theoryRetina200323342142412824853
- UnokiNNishijimaKKitaMLamellar macular hole formation in patients with diabetic cystoid macular edemaRetina20092981128113319491719
- GeorgalasIMarkomichelakisNLadasIRetinal detachment due to a macular hole in a patient with Behcet disease treated with vitrectomy and silicone oil tamponadeEur J Ophthalmol20081861023102418988182
- PattersonJAEzraEGregorZJAcute full-thickness macular hole after uncomplicated phacoemulsification cataract surgeryAm J Ophthalmol2001131679980011384582