Abstract
Background
Scleral buckle surgery is not a commonly performed surgical procedure in Sub-Saharan Africa due to a paucity of trained vitreo retinal surgeons. The aim of the study was to review sclera buckle procedures with a view to evaluating the anatomical and visual outcomes.
Methods
Case records of patients that had scleral buckle surgery at the Retina Unit of the University College Hospital, Ibadan, Nigeria, between 2007 and 2010 were reviewed. Information retrieved included patients’ demographics, duration of symptoms, and presenting vision. Other information included site of retinal break, extent of retinal detachment, involvement of the fellow eye, and macular involvement. Postoperative retina reattachment and postoperative visual acuity were also recorded. Proportions and percentages were used to analyze data.
Results
Forty five eyes of 42 patients were studied with a male to female ratio of 1.6:1. The mean age was 47.7 years (±17.6 years). The median duration before presentation was 3 months (range: 5 days – 156 months). Subtotal retinal detachment was found in 35 eyes (77.8%) while total retinal detachment occurred in ten eyes (22.2%). Thirty four eyes (75.6%) had “macular off ” detachments. At 6 weeks, there was an improvement in visual acuity in 23 eyes (51.1%), while visual acuity remained the same in nine eyes (20%) and was worse in 13 eyes (28.9%). Anatomical attachment was seen in 43 eyes (95.6%) on the operation table, in 40 eyes (90.9%) at first day postoperatively and in 32 eyes (86.5%) at 6 weeks after surgery.
Conclusion
Outcome of sclera buckle surgery for rhegmatogenous retinal detachment may be improved in developing countries of Sub Sahara Africa if adequate awareness is created to educate the populace on early presentation.
Introduction
Scleral buckling is one of the most established techniques for the treatment of primary rhegmatogenous retinal detachment. Jules Gonin performed the first successful retinal detachment surgery after accurate localization of retinal breaks, drainage of subretinal fluid and thermo cautery.Citation1 He presented his work to the Swiss Ophthalmology Society and laid the foundation for retinal detachment surgery.Citation2 Ernst Custodis performed the first sclera buckle surgery.Citation3 Charles Schepens developed the indirect ophthalmoscope with sclera depressor and performed the first buckling surgery in the United StatesCitation4 while Harvey Lincoff introduced the silicone sponge and modern cryotherapy.Citation5,Citation6
The scleral buckling procedure has resulted in improved vision especially when it is performed in fresh retinal detachment.Citation7–Citation9,Citation11,Citation12 In the developing countries like Nigeria, resources are scarce and vitrectomy facilities are not readily available. Scleral buckling surgeries give hope to people with rhegmatogenous retinal detachment.
The aim of this study is to highlight the anatomical and visual outcomes of scleral buckle in relation to the pattern of presentation of rhegmatogenous retinal detachment at the University College Hospital (UCH), Ibadan, Nigeria.
Material and methods
This is a retrospective interventional case series of all patients who had scleral buckling surgeries done at the Retina and Vitreous Unit of the Department of Ophthalmology, University College Hospital, Ibadan, Nigeria, from October 2007 to May 2010. Information retrieved from the case records include sociodemographic data, source of referral, site of retinal breaks, macular involvement, involvement of fellow eye, visual acuity (VA) at pre -and post-scleral buckle surgery, anatomical success of the procedure, visual outcome, complications, and reoperations.
Scleral buckle surgery in our center is mostly performed under local anesthesia in adults with general anesthesia used for children. The procedure included conjunctiva peritomy, recti muscle bridle sutures, localization of breaks with indirect ophthalmoscopy and cryotherapy to retinal breaks. Scleral anchor sutures using spatulated 5-0 dacron sutures (Ethicon, Johnson & Johnson, New Brunswick, NJ, USA) are applied over the retinal breaks. Silicone or rubber sponges are then applied. Subretinal fluid drainage is done in eyes with bullous retinal detachments and long standing detachments with a 25 gauge needle close to the horizontal meridian. Air is injected into the vitreous cavity in eyes with superior breaks. Anatomical (attachment) success was defined as the apposition of the sensory retina to the retinal pigment epithelium. This was checked on the table, at discharge and at 6 weeks. Good visual outcome was defined as improvement in VA of at least two lines using the illuminated Snellen’s chart at 6 weeks. Fair visual outcome was defined as improvement in Snellen VA of one line. Fellow eye involvement was defined as the presence of features predisposing to retinal detachment seen in the other eye, such as retinal breaks or tears and lattice degeneration.
Results
Forty two patients were analyzed with a male to female ratio of 1.6:1. Forty five eyes of these 42 patients had surgeries and were studied. All the patients had phakic retinal detachments. Three patients had bilateral retinal detachment (one male, two female). Fifty one percent (23 eyes) had left eye surgeries while 48.9% (22) of surgeries were performed on right eyes. The patients’ ages ranged between 11–79 years (mean: 47.7 years, standard deviation ± 17.6 years).
The median duration before presentation was 3 months (5 days – 156 months) and the median duration between presentation and surgery was also 3 months (1 day – 5 months). Twenty four people (53.3%) were referred from private eye clinics. Twenty one eyes (46.7%) had retinal breaks located at the superotemporal quadrant, 13 (28.9%) had breaks in the inferotemporal quadrant and eight eyes (17.8%) had retinal breaks in the inferonasal quadrant. Superonasal quadrant break was found in one eye. One patient had breaks in both the superotemporal and superonasal quadrants. In one eye, the break could not be found but the probable site was suspected by the Lincoff’s rule. Thirty two eyes (72.7%) had horseshoe tears while ten eyes had atrophic holes (22.7%). Two eyes (4.6%) had giant retina tears. The fellow eye had pathological changes that may predispose to retinal detachment in 38% of the studied patients, while lens opacity was present in 19 eyes (42.2%). Subtotal retinal detachment was found in 35 eyes (77.8%) while total retinal detachment occurred in ten eyes (22.2%). Thirty four eyes (75.6%) had “macular off ” detachments while eleven eyes (24.4%) did not have macular involvement. Sponge plus an encirclement band were used in 27 eyes (60%) while 18 eyes (40%) had sponge alone applied to close the breaks. Subretinal fluid (SRF) drainage was done in 38 (84.4%) eyes.
Postoperative complications seen included raised intraocular pressure in five eyes. Reoperation occurred in five eyes due to the reopening of breaks from proliferative vitreo retinopathy (PVR).
At presentation, 24 eyes (53.3%) had VA <3/60, ten eyes (22.2%) had VA between 6/18 and 3/60, and eleven eyes (24.4%) had VA >6/18. However, the proportion of patients with VA $3/60 increased from 47.7% pre-operatively to 59.1% on the first post-operative day (P = 0.008) and the proportion of patients with VA $3/60 increased to 66.7% by 6 weeks after surgery (P = 0.005) ().
Table 1 Visual outcome of scleral buckle surgery in Ibadan, Sub-Saharan Africa
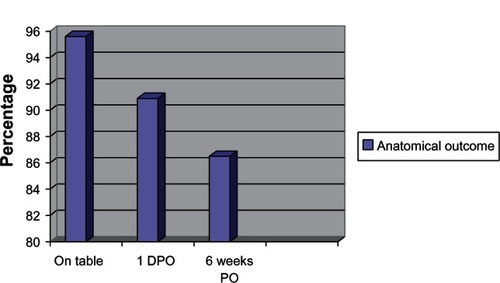
With regards to visual outcome at 6 weeks, there was an improvement in VA in 23 eyes (51.1%), while VA remained the same in nine eyes (20%), and was worse in 13 eyes (28.9%). Among the 23 eyes with improvement, the VA improved by one Snellen line in five (21.7%) eyes; by two lines in ten (43.5%) eyes; and by three or more lines in eight (34.8%) eyes . Anatomical attachment was seen in 43 eyes (95.6%) on the operation table, in 40 eyes (90.9%) at first day postoperative and in 32 eyes (86.5%) at 6 weeks post operation ().
Figure 1 Anatomical outcome of sclera buckle surgery in Ibadan, Sub-Saharan Africa.
Discussion
This study showed that scleral buckle surgery for rhegmatogenous retinal detachment gives fairly good anatomical and visual outcomes. This is similar to previous studies in NigeriaCitation7 and East Africa.Citation8 Scleral buckle surgery positive outcomes are reported to be greater than 90 percent and it is appropriate for most primary rhegmatogenous retinal detachment. It is the procedure with the most documented follow up.Citation9 The outcomes might have been better in this study. The median period of presentation was 3 months after onset of symptoms, and about two-thirds of the patients presented with “macular off ” detachments. The late presentation and macular involvement are likely to have adversely affected the visual outcome. In an earlier study in Nigeria, over 90% of patients presented with “macular off ” detachments.Citation7 This is not unconnected to problems of diagnosis and late referrals. After diagnosis some of our patients still encountered delays before surgery due to financial constraints.
Encirclement was done in more than half of the cases. Most patients presented with PVR requiring encirclement. A single silicone sponge was used in the remaining cases as they had grade B or less PVR changes. Subretinal fluid drainage was performed in most cases especially in long standing cases, highly bullous detachments and the elderly with poor retina pigment epithelial (RPE) function.
Complications of surgery included raised intraocular pressure in five patients. All the cases were controlled on topical antiglaucoma medications. Reopening of breaks was noted in five patients necessitating reoperations with buckle adjustment and reinforcement.
Retinal reattachment occurred in most patients (95.6%) on the operating table. The proportion reduced to about 86.5% at six weeks post-operatively. The proportion with blind eyes at presentation reduced from 59% to 33% at 6 weeks post-operatively. Proliferative vitreo retinopathy may have been responsible for the poor outcome in some of the patients who presented for surgery late. Performing vitrectomy for this group of patients may have helped improve visual outcome. It has been shown that vitrectomy produces less operating time, accurate localization of holes, less refractive changes and less reoperation.Citation10,Citation12 Vitrectomy facilities are inadequate or unavailable in Sub-Sahara Africa. Scleral buckle surgery has also been found to be effective with studies reporting comparative results.Citation11,Citation12
In conclusion, scleral buckle surgery for rhegmatogenous retinal detachment may have a better outcome in developing countries of Sub-Saharan Africa if adequate awareness is created to educate the populace on early presentation. Scleral buckle surgery is advised in recent detachments with single peripheral retinal breaks. Provision of vitrectomy services may also improve the success rate of intervention especially in patients with longstanding retinal detachments.
Limitations
The study being a retrospective review is prone to problems with data retrieval. A prospective study will overcome these problems.
Acknowledgments
The assistance of the record staff of the Eye Clinic, University College Hospital, Ibadan, Nigeria in making it possible to retrieve case notes is appreciated.
Disclosure
The authors report no conflicts of interest in this work.
References
- GoninJLa pathologenie du decollement spontane de la retine. [The spontaneous pathology of the detachment of the retina]Ann D’Oculist (Paris)1904132230 French
- GoninJThe treatment of detached retina by searing the retinal tearsArch Ophthalmol193045621625
- CustodisE[Treatment of retinal detachment by circumscribed diathermal coagulation and by scleral depression in the area of tear caused by imbedding of a plastic implant]Klin Monbl Augenheilkd Augenarztl Fortbild19561294476495 German13386159
- SchepensCLProgress in detachment surgeryTrans Am Acad Ophthalmol Otolaryngol19515560761514866956
- LincoffHABarasIMcLeanJModifications to the Custodis procedure for retinal detachmentArch Ophthalmol19657316014237781
- LincoffHAMcleanJMNanoHCryosurgical treatment of retinal detachmentTrans Am Acad Ophthalmol Otolaryngol19646841243214169749
- AlhassanMBRabiuMMOlongusuaYAhmedAOutcome of scleral buckling for primary rhegmatogenous retinal detachment in NigeriaMed Sci Monit20051112:CR589CR59316319791
- YorstonDJalaliSRetinal detachment in developing countriesEye20021635335812101440
- SchwartzSGKuhlDPMcPhersonARTwenty-year follow up for sclera bucklingArch Ophthalmol200212032532911879136
- SharmaYRKarunanithiSAzadRVFunctional and anatomic outcome of scleral buckling versus primary vitrectomy in pseudophakic retinal detachmentActa Ophthalmol (Scand)20058329329715948779
- AhmadiehHMoradianSFaghihiHBuckling versus primary vitrectomy in pseudophakic and aphakic retinal detachmentOphthalmology20051121421142915961159
- HeimannHBartz-SchmidtKUBornfeldScleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical studyOphthalmology20071142142215418054633