Abstract
Background
The purpose of this study was to evaluate the results and complications of early surgical resection of large amblyogenic subdermal eyelid hemangiomas in infants after prior short-term parenteral administration of corticosteroids.
Methods
Sixteen infants were given dexamethasone 2 mg/kg/day in two divided doses for three consecutive days prior to scheduled surgical excision of large eyelid hemangiomas. The lesions were accessed via an upper eyelid crease, subeyebrow incision, or a lower eyelid subciliary incision.
Results
In all cases, surgical excision of the entire lesion was possible with no significant intraoperative or postoperative complications. The levator muscle/aponeurosis complex was involved in 31.25% of cases and was managed by reinsertion or repositioning without resection. A satisfactory lid position and contour with immediate clearing of the visual axis was achieved in all but one case (93.8%).
Conclusion
Parenteral corticosteroids helped in reducing volume and blood flow from the hemangiomas, allowing for very early total excision of large subdermal infantile hemangiomas without significant intraoperative hemorrhage. This resulted in immediate elimination of any reason for occlusion amblyopia. Long-term follow-up of visual development in these patients would help to demonstrate the effectiveness of this strategy compared with more conservative measures.
Introduction
Some authors have described large eyelid hemangiomas as “high-risk” or “clinically deceiving” lesions because, even after treatment with steroids, they display an “apparently open” visual axis.Citation1 Studies of the prevalence of amblyopia in such patients have reported rates of 50%–60%.Citation2 Present treatment strategies with either oral or local intralesional steroids, although very effective from the long-term cosmetic point of view, do not appear to achieve the desired goal as regards prevention of imminent amblyopia. Therefore, early primary surgical resection would provide an attractive alternative, but many surgeons are reluctant to perform the procedure for fear of postoperative scarring causing eyelid disfigurement or extensive bleeding potentially requiring blood transfusion.Citation3 The aim of this work was to evaluate the results and complications of early surgical resection of large amblyogenic subdermal eyelid hemangiomas in infants after short-term parenteral administration of corticosteroids.
Materials and methods
In this prospective case series, 16 infants with large subdermal upper or lower lid hemangiomas, without orbital extension, were given parenteral dexamethasone 2 mg/kg/day in two divided doses for three consecutive days prior to scheduled surgical excision of the tumor. The decision for early surgery was taken after parental counseling, explaining the benefits and risks and with the approval of the local research ethics committee. Steroids were given under the supervision of a pediatrician. A detailed history and physical examination were performed, including recording of body weight, height, skull circumference, and blood pressure, as well as hematologic investigations for baseline blood sugar, electrolytes, and abnormalities of coagulation. These measurements were repeated three months after steroid administration. Hemangiomas were included if the lesions were large enough to occupy more than half of the lid margin, extended beyond the eyelid region, and obstructed the visual axis. Preoperative computed tomography enabled specific localization, accurate measurement, and determination of the extent of the lesions. No Doppler studies were needed because all cases were restricted to the eyelids with no orbital involvement. Surgical removal was done by one of the authors (REE) and the lesions were biopsied. Any intraoperative or postoperative complication was recorded. Withdrawal of steroids was not necessary because the duration of therapy did not exceed three days, according to the protocol of withdrawal of steroid therapy.Citation4 Treatment of amblyopia was initiated soon after surgery.
Results
The mean age of the infants was 3.93 ± 2.8 (1–11) months, and approximately two thirds were female (n = 10, 62.5%). Most of the hemangiomas (n = 13, 81.2%) affected the upper eyelid. All lesions caused obscuration of the visual axis with mechanical ptosis leading to corneal deformation. The average size of the hemangiomas was 3.22 ± 1.15 cm × 2.63 ± 1.15 cm. Preoperative steroids caused a change in the texture and color as well as size of the lesions, and the overlying skin became wrinkled with ulceration and sloughing of some areas. The tumors were accessed via an upper eyelid crease incision (in 10 cases), a subeyebrow incision in the upper eyelid (in three cases), or a subciliary incision in the lower eyelid (in three cases). Dissection was mainly carried out in a blunt fashion and aided by careful cauterization. Complete resection was attempted, leaving only small residues of hemangioma around the lacrimal gland, lacrimal canaliculi, or near the roots of the eyelashes. The levator muscle and aponeurosis were identified, carefully separated and, if involved, reinsertion and/or repositioning of the residual muscle was done without further muscle resection. This was required in five cases (31.25%). Biopsy confirmed infantile hemangioma in all cases. A satisfactory appearance and lid position with immediate clearing of the visual axis was achieved in all but one case which had severe postoperative ptosis. No intraoperative complications or uncontrollable intraoperative hemorrhage was encountered, and no donor blood transfusion was required. No postoperative hemorrhage occurred. Other than expected sloughing of the overlying skin due to necrosis of the hemangioma, no preoperative complications from steroids or withdrawal symptoms were noted, and there was no adrenal suppression or growth retardation. Three months after resection, mean corneal astigmatism was 0.87 ± 0.85 diopters. No recurrences have been noted during a follow-up period of 4.25 ± 1.77 (3–9) months.
Discussion
Hemangioma of the eyelid accounts for 1%–3% of all cases of hemangioma in newborns.Citation5 It may be deep subdermal or superficial (known as a strawberry nevus) or sometimes a combination of both. Subdermal hemangiomas tend to undergo more rapid and more prolonged growth than superficial ones.Citation6 Ultrasonographic examination shows that these lesions have a very high blood flow in feeding vessels, ie, about 2–3 orders of magnitude greater than in normal capillary beds.Citation7 Large hemangiomas can result in amblyopia due to occlusion of the visual axis or astigmatism. Other authors have suggested that a size greater than 1 cm in largest diameter is an important predictor of amblyopia.Citation8 Early surgical removal in infancy, if possible, would be beneficial, considering that even a 1–2-week period of visual deprivation in this critical period has been demonstrated to have the potential to cause permanent cortical visual deficits.Citation1
Surgical excision of eyelid hemangiomas is usually indicated for removal of small, involuted, well localized residual lesions (and likely to leave an esthetically more acceptable scar) and for lesions that continue to cause amblyopia despite treatment with oral or intralesional steroids, or both. However, there is limited experience in the literature of primary excisional surgery, especially in infants.Citation3,Citation5,Citation9–Citation11 In one report of six hemangiomas treated primarily with surgical resection,Citation3 two cases required intraoperative donor blood transfusion to control severe intraoperative hemorrhage, and one case had postoperative wound transudation and wound dehiscence. The same patient later needed surgical scar revision. Other studies showing successful primary removal without complications either reported on a few moderately sized lesions,Citation5,Citation9 or removal done under ultrasonic guidance using a Dissectron.Citation10,Citation11 In this case series, preoperative parenteral corticosteroid injections, known to reduce volume and blood flow in haemangiomas,Citation12 allowed for even large subdermal infantile hemangiomas to be completely and safely excised without postoperative fibrosis or disfigurement (). The idea for this came from a previous reportCitation13 of using pulsed intravenous methylprednisolone followed by oral corticosteroids in children with periocular hemangioma in whom the visual prognosis was poor. That study showed that short-term parenteral corticosteroids alone achieved rapid shrinking of hemangiomas and complete resolution of their visual impact within two days, which would appear to be more rapid than with usual oral corticosteroid therapy.
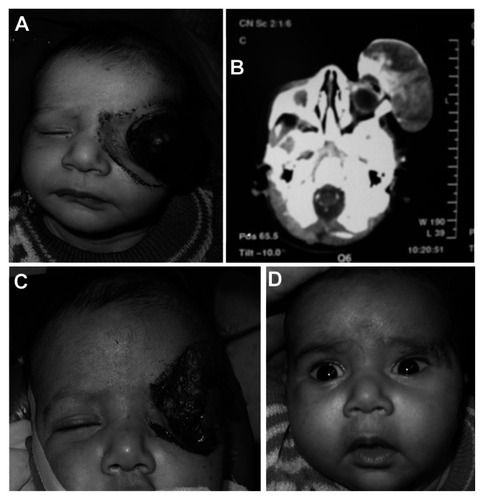
Figure 1 (A) Two-month-old boy presenting with a huge “tennis ball” hemangioma with (B) computed tomography scan showing no orbital extension. (C) Three days after parenteral steroids showing a marked decrease in size with sloughing of the overlying skin. (D) Two weeks after surgical removal.
Systemic side effects are reported in the literature to occur in 27%–44%Citation14,Citation15 of cases when corticosteroids are used for prolonged treatment of periorbital hemangiomas. These include behavioral changes, insomnia, cushingoid appearance, and hypertension, which were all avoided in our study. Despite the high parenteral steroid dose given, adrenal suppression and/or growth retardation were not noted during the short period of follow-up. However, the long-term repercussions, if any, of early parenteral steroid therapy on the natural growth and development of such very young infants remain to be assessed by longer follow-up.
Resection of the levator muscle/aponeurosis, despite involvement in almost one third of cases (31.25%), was not performed at this stage to avoid postoperative lid retraction. Postoperative ptosis was avoided in these cases by careful identification and suturing of healthy tissue. Only one case of severe postoperative ptosis due to an unidentifiable levator muscle was encountered using this technique.
It has been demonstrated that the longer a complicated periocular hemangioma is observed, the greater the astigmatism and the less amenable it will be to correction following tumor removal.Citation16,Citation17 In one study,Citation17 the degree of astigmatism improved from 2.75 to 0.80 diopters in infants younger than three months undergoing surgical resection and from 3 to 1.1 diopters in older children. In our series, astigmatism was only measured postoperatively because the large size of the lesion did not permit accurate preoperative measurements, and was found to be insignificant (0.87 ± 0.85) in accordance with the figures previously mentioned.
Conclusion
Early surgical resection of large eyelid hemangiomas following short, high-dose, parenteral corticosteroid administration is safe and results in immediate elimination of amblyogenic factors. Surgical removal from the very thin and underdeveloped infant eyelid requires an excellent knowledge of eyelid anatomy to avoid massive intraoperative bleeding and postoperative ptosis. Long-term follow-up of the visual development of these patients would help to confirm the advantages of this strategy compared with more conservative measures.
Acknowledgment
The authors thank the guardians of the patients in this study for agreeing to publication of photographs to show the effect of treatment in this study.
Disclosure
This paper was presented in part as a poster at the European Society of Ophthalmic Plastic and Reconstructive Surgery annual meeting held on September 9–11, 2010, in Munich, Germany. Otherwise, the authors report no conflicts of interest in this work.
References
- FrankRCCowanBJHarropARAstleWFMcPhalenDFVisual development in infants: visual complications of periocular haemangiomasJ Plast Reconstr Aesthet Surg20106311819097831
- HaikBGJakobiecFAEllsworthRMJonesISCapillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 casesOphthalmology1979865760792545208
- WalkerRSCusterPLNeradJASurgical excision of periorbital capillary haemangiomasOphthalmology19941018133313408058277
- JacobsTPWhitlockRTEdsallJHolubDAAddisonian crisis while taking high dose glucocorticoids. An unusual presentation of primary adrenal failure in two patients with underlying inflammatory diseasesJ Am Med Assoc19882601420822084
- SlaughterKSullivanTBoultonJO’ReaganPGoleGEarly surgical intervention as definitive treatment for ocular adnexal capillary haemangiomaClin Experiment Ophthalmol200331541842314516430
- TambeKMunshiVDewsberyCAinsworthJRWillshawHParulekarMVRelationship of infantile periocular hemangioma depth to growth and regression patternJ AAPOS200913656757020006818
- VerityDHRestoriMRoseGENatural history of periocular capillary haemangiomas: changes in internal blood velocity and lesion volumeEye (Lond)200620101228123717019424
- SchwartzSRBleiFCeislerESteeleMFurlanLKodsiSRisk factors for amblyopia in children with capillary hemangiomas of the eyelids and orbitJ AAPOS200610326226816814181
- AldaveAJShieldsCLShieldsJRSurgical excision of selected amblyogenic periorbital capillary hemangiomasOphthalmic Surg Lasers199930975475710574498
- MomtchilovaMPelosseBDinerPAVazquezMPLarocheLAmblyopia and peri-ocular capillary hemangioma of infancy: screening and clinical course before and after surgeryJ Fr Ophtalmol2004271011351140 French15687923
- ClaudeOPicardAO’SullivanNUse of ultrasonic dissection in the early surgical management of periorbital haemangiomasJ Plast Reconstr Aesthet Surg200861121479148518037085
- VerityDHRoseGERestoriMThe effect of intralesional steroid injections on the volume and blood flow in periocular capillary haemangiomasOrbit2008271414718307146
- DelesalleFStaumontDHoumanyMABreviereGMPietteFPulse methylprednisolone therapy for threatening periocular haemangiomas of infancyActa Derm Venereol200686542943216955189
- RanchodTMFriedenIJFredrickDRCorticosteroid treatment of periorbital haemangioma of infancy: a review of the evidenceBr J Ophthalmol20058991134113816113367
- PopeEKrafchikBRMacarthurCOral versus high-dose pulse corticosteroids for problematic infantile hemangiomas: a randomized, controlled trialPediatrics20071196e1239e124717485449
- LeviMSchwartzSBleiFSurgical treatment of capillary hemangioma causing amblyopiaJ AAPOS200711323023417344079
- ArnejaJSMullikenJBResection of amblyogenic periocular hemangiomas: indications and outcomesPlast Reconstr Surg2010125127428120048618