
Abstract
Purpose
To report the outcomes of using a sutureless human amniotic membrane dehydrated matrix (HAMDM) in the management of a range of ocular surface conditions utilizing a digital ocular surface disease assessment tool.
Methods
Two UK NHS Trusts — Queen Victoria Hospital Foundation Trust (East Grinstead and Maidstone) and Tunbridge Wells Trust (Kent) — prospectively treated patients with ocular surface disease with sutureless HAMDM. The patient cohort was assessed for resolution of epithelial defects, ocular surface inflammation, and best-corrected visual acuity pre- and posttreatment. Measurements of ocular surface inflammation and epithelial defect size were assessed using AOS digital imaging software, a validated tool for objective grading of bulbar conjunctival redness and measurement of corneal epithelial defects.
Results
A total of 47 applications of sutureless HAMDM on 46 eyes of 46 patients (25 male, 21 female, age 9–94 years) were assessed across various etiologies for an average of 24.0±14.1 days. Patients with limbal stem-cell deficiency (n=17), persistent epithelial defects (n=16), neurotrophic corneal disease (n=7), filamentary keratitis (n=2), corneal erosion (n=1), corneal thinning (n=1), ocular surface inflammation (n=1), and traumatic corneal laceration (n=1) were included in the study. Across all patents, 63% of eyes showed complete healing of epithelial defects and 32.6% of eyes showed partial resolution. The average rate of healing (wound closure) was 0.36 mm2 per day across the overall patient cohort, and the rate of healing in cases with complete resolution of epithelial defects was 0.41 mm2 per day. Inflammation across all four quadrants of the ocular surface remained stable. Visual acuity across the patient cohort remained stable (61%) and improved in 26% of patients (0.06±0.51 logMAR).
Conclusion
Sutureless HAMDM application can be accomplished in just a few minutes and effectively treat a range of ocular surface disease in a clinical, nonsurgical setting. The AOS imaging software offered a quantitative methodology for measuring epithelial defect size and inflammation state.
Introduction
Ocular surface disease (OSD) is a multifactorial disease of the ocular surface (lids, conjunctiva, and cornea) and is characterized by tear-film instability, ocular surface dryness, and inflammation with or without ocular surface epithelial breakdown. OSD is a global health-care problem and is estimated to affect 5%–30% of the population.Citation1,Citation2 The disease state can be driven by underlying pathology, including lid-margin disease, infection, trauma, or multifactorial changes in ocular homeostasis.Citation3 OSD is a significant cause of ocular discomfort and visual disturbances affecting patients’ overall ocular health and general well-being.Citation4
Persistent epithelial defects (PEDs) often present as a challenging condition associated with OSD. They are defined as failure of reepithelialization in 14 days with standard treatment.Citation5 Management of OSD involving PEDs requires a stepwise approach based on etiology. The standard first-line approach in such situations includes increased frequency of topical lubrication, blood-derived products (autologous/allogeneic serum application), bandage contact lens, punctal occlusion, epithelial debridement, or temporary lid closure (eg, Botulinum toxin injection to the tarsal plate or temporary tarsorrhaphy).Citation6 Transplantation of the amniotic membrane for the management of OSD has been a popular treatment adjunct in ophthalmology since the 1990s due to its healingCitation7 and anti-inflammatory properties,Citation8 antifibrotic activity, and pain-reducing capacity.Citation9
The amniotic membrane is the innermost layer of the placental sac and is harvested from consenting women giving birth through elective cesarean sections.Citation10 For superficial OSD, the amniotic membrane can be applied epithelial side down as a temporary biological dressing to cover the deepithelialized area, protecting from mechanical and environmental factors whilst providing an environment conducive to healing.Citation11 This temporary biological dressing is commonly referred to as a “patch” or “onlay graft.Citation10,Citation12 An amniotic membrane patch acts as a physical barrier between the damaged eye surface and eyelid helping to prevent the formation of symblepharon and ankyloblepharon.Citation10 At the same time, the amniotic membrane acts a physical barrier to infiltrating inflammatory cells and can release bioactive factors to limit inflammation progression, fibrosis, angiogenesis, and support epithelialization.Citation10,Citation13,Citation14 This synergy of effects can make amniotic membrane transplantation an effective treatment adjunct for patients with OSD.Citation10 A patch is not incorporated into the ocular surface permanently, but instead either degrades over time or is removed once depleted or the underlying defect heals. Recent advances in amniotic membrane preservation and application techniques have allowed for the tissue to be transplanted in an outpatient “in-office” setting.Citation15 The use of a specialized bandage contact lenses or mounted plastic symblepharon rings removes the need for sutures and thus costly and complex surgical management.Citation15,Citation16 This has opened access to amniotic membrane to a wider range of patients with OSD.
Historically, the ability to objectively measure a patient’s disease state, such as ocular surface inflammation, epithelial defect size, and rate of healing, has been extremely limited, with most of these outcome measures being assessed subjectively or through patient-led outcome evaluation.Citation17 Current standard methodologies for measuring ocular epithelial defects involve horizontal and vertical ruler measurement, ignoring the overall defect shape or area, whereas the standardized methodology for reporting ocular inflammation is set through the Standardization of Uveitis Nomenclature (SUN) working group.Citation18 However, this is a qualitative measurement, which although standardized through the SUN group, does not give a quantitative measurement to note more detailed changes in the patients’ ocular health. Therefore, the objective of this publication is to report prospective outcomes in the management of a range of OSDs with or without PEDs using a sutureless human amniotic membrane dehydrated matrix (HAMDM) through an objective digital assessment tool (AOS; Advanced Ophthalmic Solutions, UK).
Methods
Patients were prospectively audited across two UK NHS centers — Queen Victoria Hospital, East Grinstead (a tertiary care center) and Maidstone and Tunbridge Wells Trust, Kent (general hospital), UK — between July 2021 to June 2022. Patients were managed by the same clinicians at both hospitals. Patients included in the audit suffered OSD, particularly ocular surface inflammation, with or without an epithelial defect. Patients that were lost to follow-up due to being unable to attend were excluded from the audit. The audit was registered with the local institutional boards at both hospitals and adhered to the tenants of the Declaration of Helsinki. Informed consent was received from all patients or through a parent or legal guardian if they were <18 years of age.
Patients were treated with a 12 mm-diameter HAMDM (Omnigen C, NuVision Biotherapies, UK), applied using a bespoke bandage contact lens with 16 mm diameter and 8.8 mm base curve (OmniLenz C, NuVision Biotherapies), which is specially designed to load and retain the amniotic membrane at the ocular surface. All patients were treated with topical anesthesia (proxymetacaine 0.5% eye drops) prior to treatment application as per the manufacturer’s guidelines.Citation19 Using a standardized aseptic technique, the HAMDM was removed from its packaging and loaded onto the concave side of the OmniLenz using straight tying forceps, allowed to rehydrate, and then the OmniLenz was applied with the HAMDM oriented epithelial side down against the ocular surface. Treatment duration was determined by clinical progress, which varied in different etiologies. Once complete, the OmniLenz and residual HAMDM were removed from the ocular surface. If the patient demonstrated partial healing, clinician discretion was used to either place an additional HAMDM or use alternative treatment options.
All patients were given topical antibiotics (chloramphenicol 0.5% eye drops) as a concomitant medication during the procedure, or an antimicrobial sensitivity specific treatment for those patients with an active infection. The HAMDM and OmniLenz application were combined with tarsorrhaphy for some patients that required additional support to retain the treatment at the ocular surface, due to eyelid or forniceal abnormalities.
Pretreatment and throughout follow-up, patient eyes were imaged using the AOS. This has been validated as an image-measurement and grading tool with superior reliability indices compared to subjective methods employed by Efron and Cornea and Contact Lens Research Unit grading systems.Citation20 Photographs of all patients were taken through slit-lamp photography (superior, inferior, nasal, and temporal bulbar conjunctiva, as well as highlighted epithelial defects using fluorescein staining) prior to HAMDM application and following HAMDM removal (). The principal measurements were corneal epithelial defect size (mm2), inflammation based on level of hyperemia on the four bulbar conjunctival surfaces ( and ), and rate of epithelial healing (difference in epithelial defect size before and after HAMDM application divided by time in days).
Figure 1 A patient’s epithelial defect highlighted by fluorescein stain under blue filter uploaded to AOS software.
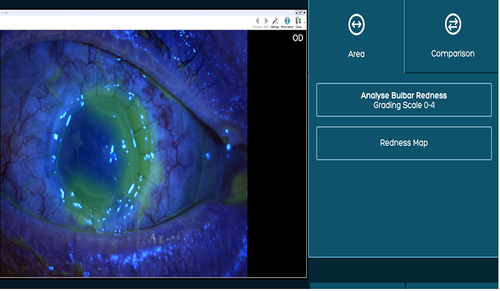
Figure 2 The white to white (WTW) is marked using the AOS software ruler tool. The highlighted epithelial defect is then measured (mm2) using the area tool in comparison to WTW measurement.
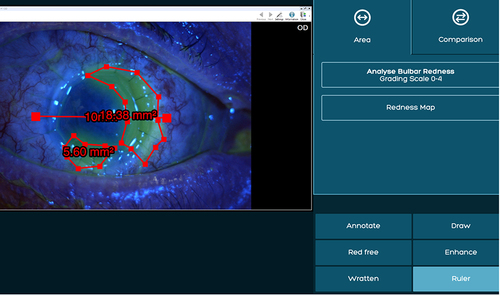
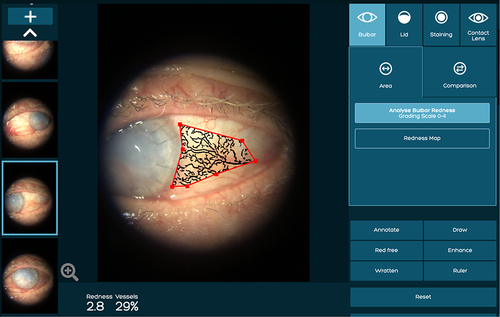
Figure 3 An example of temporal bulbar conjunctival inflammation score measurement followed by marking the desired area using the area tool.
All patients were assessed for best-corrected visual acuity (BCVA) pre- and posttreatment. The primary outcome for this cohort of patients was complete resolution of the ocular surface defect following treatment with the HAMDM. Complete healing was defined as complete closure of the epithelial defect or complete resolution of the ocular inflammation at the final follow-up appointment. Partial healing was defined as a reduction in ocular inflammation or reduction in the size of the epithelial defect between first application and final follow-up. Secondary outcome measures comprised time to heal, change in epithelial defect size (percentage and mm2), average epithelial defect reduction per day, BCVA, and ocular surface inflammation grading by measurement of bulbar conjunctival blood vessels/injection (percentage).
Results
A total of 46 eyes of 46 patients with various ocular surface etiologies were included in this audit and treated with sutureless HAMDM (). Of the 46 patients, 36 were recruited from Queen Victoria Hospital and 10 from Maidstone and Tunbridge Wells Hospitals. The patient cohort consisted of 25 men (54.3%) and 21 women (45.7%), with an average age of 56.9±28.8 (9–94) years. The average time between first presentation and HAMDM treatment was 25.1±25.2 days.
Table 1 Demographics of the patient cohort
Of the 46 patients, 97.8% (n=45) of patients received one HAMDM application, with a further 2.2% (n=1) receiving two applications. Patients had an average HAMDM treatment time of 24.0±14.1 days. All patients received unilateral treatment. The average follow-up was 56.1±29.4 days. One patient was excluded from the audit due to loss to follow-up during the study period ().
The indications treated within the audit are noted in . These comprised limbal stem-cell deficiency (n=17), PEDs (n=16), neurotrophic cornea (n=7), filamentary keratitis (n=2), corneal erosion (n=1), corneal thinning (n=1), ocular surface inflammation (n=1), and laceration (n=1). Average HAMDM treatment duration was 24.0±14.1 days. All patients received unilateral treatment. The average follow-up was 56.1±29.4 days.
Table 2 Patient etiology and duration of sutureless amniotic membrane treatment
For the overall patient cohort, the average wound reduction was 8.7±11.1 mm2. For these patients, the average rate of wound reduction per day was 0.36±0.79 mm2/day. For completely resolved patients, the average wound reduction was 10.3±11.1 mm2, and this patient cohort experienced a healing rate of 0.41±0.79 mm2/day.
Patients in the neurotrophic cornea and PED cohorts experienced the best complete-resolution results (n=6, 85.7% and n=14, 87.6%, respectively). The limbal stem-cell deficiency cohort saw mostly partial resolution (n=11, 64.7%); however, many of these patients (n=6, 55%) required surgical intervention, including corneal grafts (n=3, 50%), amniotic membrane grafting (n=2, 33%) and limbal stem-cell transplantation (n=1, 16.7%). There was a single case (n=1, 2.2%) of a deteriorated state in a patient with ocular surface inflammation due to chronic Stevens–Johnson syndrome. Following sutureless HAMDM treatment, this patient developed an epithelial defect that healed uneventfully within 1 week after removal of the HAMDM.
The largest group of patients in the cohort were those with limbal stem–cell deficiency (37%), defined by a loss of limbal anatomy following an ocular event.Citation21 Patients were defined as limbal stem cell–deficient when they had lost more than 3 clock hours of limbal ischemia. For patients in this cohort, limbal stem-cell deficiency had resulted from ocular burns (n=7), Stevens–Johnson syndrome (n=6), aniridia (n=1), pemphigoid (n=1), perforation (n=1), and penetrating keratoplasty (n=1) (). The mean length of treatment for this patient cohort was 24.6±19.7 days.
The second main cohort of patients treated with HAMDM was PED (39.1%) (). These defects were due to infectious keratitis (n=6), penetrating keratoplasty (n=4), Fuchs endothelial dystrophy (n=2), entropion (n=1), neurotrophic cornea (n=1), ocular burns (n=1), and Peters anomaly (n=1). No adverse events were noted throughout the study. The mean length of treatment for this patient cohort was 23.8±9.8 days.
Table 3 Breakdown of persistent epithelial defect patient cohort
All patients were treated with topical antibiotics and topical lubricants as concomitant medications to limit the risk of infection and allow for patient comfort throughout treatment (). A range of other concomitant medications was also given to patients: topical steroids (78.3%), analgesia (43.5%), antiproteases (37.0%), systemic immunosuppressants (21.7%), topical immunosuppressants (17.4%), oral antibiotics (13.0%), systemic steroids (13.0%), plasma eye drops (13.0%), tarsorrhaphy (13.0%), and botulinum toxin (6.5%), dependent on the indication. Overall healing outcomes saw 29 patients (63%) have complete resolution of the ocular surface epithelial defect, with an additional 15 (32.6%) experiencing partial resolution of the ocular surface ().
Table 4 Concomitant medications
Table 5 Overall patient outcomes
As a secondary outcome measure, patients had their BCVA mapped throughout treatment. At first presentation, the average BCVA was 1.63±0.82 logMAR. Following treatment, the average had improved to 1.56±0.88 logMAR. Within this cohort, 28 patients (61%) experienced no change to their BCVA. Conjunctival blood-vessel count was measured throughout the audit using digital imaging software to measure bulbar conjunctival injection as a measure of ocular surface inflammation (). Four quadrants of the ocular surface were measured due to an inability to measure the complete conjunctival area in one image. There was no statistical difference in the presence of blood vessels in any area of the ocular surface across all patients (paired t test). The nasal quadrant showed the largest (7%±6.4%) reduction in blood vessel congestion between first presentation and final appointment.
Table 6 Degree of ocular surface inflammation: bulbar conjunctival blood vessel congestion scores through AOS digital assessment tool
The patients in the audit had a range of follow-up treatments (). In sum, 17 (37%) required follow-up surgery; however, 13 (76.5%) procedures would have taken place regardless of the application of sutureless HAMDM application. Application of HAMDM was to resolve and stabilize the ocular surface prior to the patient undergoing surgical intervention.
Table 7 Follow-up treatments for patients following treatment with HAMDM
Discussion
OSD embodies a range of indications, including corneal damage (erosion, thinning, neurotrophic changes, and laceration), ocular surface inflammation, filamentary keratitis, PED, and limbal stem-cell deficiency. These conditions disrupt the homeostasis of the ocular surface, and if not appropriately managed can lead to stromal melting, scarring, or even perforation, with a threat of long-term visual impairment.
Primary ocular surface disorders (keratoconjunctivitis sicca, neurotrophic disease secondary to herpes stromal keratitis, chemical injury) and systemic conditions affecting the limbal stem cells (Stevens–Johnson syndrome, ocular cicatricial pemphigoid) are the risk factors responsible for PED development. In these conditions, the ocular surface experiences prolonged inflammatory episodes that can alter the normal functioning of the epithelial basement membrane and limbal stem cells.Citation22 Neurotrophic disease accompanied by herpes stromal keratitis is known to be initiated by immunopathological processes involving T cell–mediated responses governed by proinflammatory cytokines. principally IL1 release from affected epithelial cells.Citation23 The amniotic membrane, alongside its other mentioned mechanisms, also secretes IL1ra, which has been proved to be a natural antagonist of IL1.Citation23 Late PED development is one of the serious postoperative complications following penetrating keratoplasty, affecting 4.2% of this group.Citation23 This is more commonly associated with limbal stem-cell deficiency leading to increased risk of infection, stromal collagen destruction, and corneal neovascularization threatening graft survival.Citation24
The effectiveness of HAMDM (Omnigen) in the treatment of PED of various etiologies (n=90) has been reported,Citation15 with complete resolution of 63.6% and partial healing of 23.3% (). The PED-healing rate in this cohort (n=16) was 87.6% showing complete resolution and 6.2% partial resolution. Although our patient cohort was smaller, the research was conducted by the same clinician group, and it may be assumed that improvement in healing outcome is due to greater clinical experience and confidence in treatment use, as well as better patient selection. In addition to this, these assessments were conducted prospectively to ensure more accurate mapping of complex OSD patients presenting to these centers in the UK.
Table 8 Results of persistent epithelial defect treatment with amniotic membrane and plasma eye drops: comparison between studies
The application of plasma eye drops in the treatment of OSD of various etiologies has been noted in the literature.Citation26 Chiang et alCitation25 studied 36 patients with corneal PEDs and reported a complete healing rate of 63.9% of patients at the 4-week time point. Therefore, the data in this cohort show an improvement in healing outcome from that study (). The treatment of patients with plasma eye drops required continuous repeat application and patient compliance, which is not required with sutureless HAMDM treatment. Abdelghany et al reported on the value of plasma eye drops and amniotic membrane being used as a combined therapy for severe OSD patients.Citation27
From presentation to final follow-up, patients were imaged and analyzed using a digital ocular surface assessment tool. This enabled for accurate wound-size calculation (mm2) and wound-healing rate, providing better understanding of changes in defect status between appointments. The system allowed for direct size measurements of irregularly shaped defects. The system mapped the size of the epithelial defect, the rate of closure of the wound, and blood-vessel congestion in the bulbar conjunctiva, which was used as a measure of ocular surface inflammation. Due to limitations with the imaging software, an assumption of a 10 mm limbus-to-limbus reading was assumed, with all epithelial defect sizes measured against this. This ensured accurate mapping in changes for all patients; however, it should be noted that limbus-to-limbus length differs among individuals.Citation28
There is a lack of studies documenting the rate of healing of defects in terms of millimeters squared per day. Lazreg et alCitation29 reported on changes in epithelial defect size for corneal PEDs following corneal scrubbing in a cohort of 17 patients. These patients showed an average epithelial defect size of 0.9±2.3 mm2 at day 18 compared to an average epithelial defect size of 0.4±1.4 mm2 at day 24, showing similar outcomes between the two groups. However, corneal scrubbing causes discomfort at the ocular surface for patients, and unlike amniotic membrane treatment cannot provide an inflammation-controlling mode of action.
The current standard of care within UK centers is to measure inflammation through the SUN working group scale. This highlights the need for an objective scale for inflammation measurement, and AOS software provides this measurement on the bulbar conjunctiva. Through the measurement of blood vessels, a quantitative value for inflammation can be noted as a percentage. However, due to the area for measurement being selected by the user, there is potential misreporting through the measurement of varied areas. The introduction of automatic measurements would remove any misreporting and allow for better integration into the health-care system through reducing the requirements on the health-care professional. However, this study was the first real-world experience of the use of this digital software in a hospital setting. Further studies involving digital assessment tools for objective assessment and patient-related outcome measures upon OSD patient follow-up would pave the way to improving the care that these patients receive.
Conclusion
In this cohort, a large range of OSD etiologies were able to be treated using sutureless HAMDM, which showed extensive tissue-application potential. The ease of application of the HAMDM in an outpatient setting using a bandage contact lens allowed for more superficial OSDs to be treated. The sutureless treatment was well tolerated by patients throughout the audit, with no patients rejecting the HAMDM due to discomfort. As there were no serious adverse events, the application of sutureless HAMDM has been shown to be both a safe and effective treatment for OSD. To be able to confirm more conclusive results for each indication, studies of greater numbers in specific indications are required.
The digital imaging software provided the ability to account for defect size and shape through area measurements and presented a methodology for measuring inflammation at the conjunctival surface. However, for it to be fully integrated as a digital solution into the health-care system, more accuracy in limbal length measurements and automation in taking measurements is required. This would have the potential to improve the flow of patients in the health-care pathway and be introduced as a tool for virtual consultations. Additionally, a method for measurement of blood vessels on the cornea would improve care for patients with OSD.
Ethics Approval and Informed Consent
This audit was approved as a prospective audit by the local institutional review boards at Queen Victoria Hospital NHS Foundation Trust (approval 627) and Maidstone and Tunbridge Wells NHS Trust (approval LOC/01573) and adhered to the Declaration of Helsinki. All participants provided informed consent for their involvement in the audit.
Author Contributions
All authors made a significant contribution to the reported work. This includes involvement in conception, audit design, execution, acquisition of data, analysis and interpretation of data, manuscript drafting or review, critical review of the manuscript, and revision of the manuscript. All authors have agreed upon the journal for submission, have given final approval to the manuscript, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
- Mylla Boso AL, Gasperi E, Fernandes L, Costa VP, Alves M. Impact of ocular surface disease treatment in patients with glaucoma. Clin Ophthalmol. 2020;14:103–111. doi:10.2147/OPTH.S229815
- Rana HS, Akella SS, Clabeaux CE, Skurski ZP, Aakalu VK. Ocular surface disease in thyroid eye disease: a narrative review. Ocul Surf. 2022;24:67–73. doi:10.1016/j.jtos.2022.02.001
- Katzman LR, Jeng BH. Management strategies for persistent epithelial defects of the cornea. Saudi J Ophthalmol. 2014;28(3):168–172. doi:10.1016/j.sjopt.2014.06.011
- Dahlgren MA. Persistent epithelial defects. In: Albert DM, Miller JW, editors. Albert & Jakobiec’s Principles and Practice of Ophthalmology. Philadelphia: Elsevier; 2008:749–759.
- Ljubimov AV, Saghizadeh M. Progress in corneal wound healing. Prog Retin Eye Res. 2015;49:17–45. doi:10.1016/j.preteyeres.2015.07.002
- Meller D, Pauklin M, Thomasen H, Westekemper H, Steuhl KP. Amniotic membrane transplantation in the human eye. Dtsch Arztebl Int. 2011;108(14):243–248. doi:10.3238/arztebl.2011.0243
- Liu T, Zhai H, Xu Y, et al. Amniotic membrane traps and induces apoptosis of inflammatory cells in ocular surface chemical burn. Mol Vis. 2012;18:2137–2146.
- Sharma N, Singh D, Maharana PK, et al. Comparison of amniotic membrane transplantation and umbilical cord serum in acute ocular chemical burns: a randomized controlled trial. Am J Ophthalmol. 2016;168:157–163. doi:10.1016/j.ajo.2016.05.010
- Walkden A. Amniotic membrane transplantation in ophthalmology: an updated perspective. Clin Ophthalmol. 2020;14:2057–2072. doi:10.2147/OPTH.S208008
- Malhotra C, Jain AK. Human amniotic membrane transplantation: different modalities of its use in ophthalmology. World J Transplant. 2014;4(2):111–121. doi:10.5500/wjt.v4.i2.111
- Dua HS, Gomes JA, King AJ, Maharajan VS. The amniotic membrane in ophthalmology. Surv Ophthalmol. 2004;49(1):51–77. doi:10.1016/j.survophthal.2003.10.004
- Niknejad H, Peirovi H, Jorjani M, Ahmadiani A, Ghanavi J, Seifalian AM. Properties of the amniotic membrane for potential use in tissue engineering. Eur Cell Mater. 2008;15:88–99. doi:10.22203/eCM.v015a07
- Tseng SC, Li DQ, Ma X. Suppression of transforming growth factor-beta isoforms, TGF-beta receptor type II, and myofibroblast differentiation in cultured human corneal and limbal fibroblasts by amniotic membrane matrix. J Cell Physiol. 1999;179(3):325–335. doi:10.1002/(SICI)1097-4652(199906)179:3<325::AID-JCP10>3.0.CO;2-X
- Maqsood S, Elsawah K, Dhillon N, et al. Management of persistent corneal epithelial defects with human amniotic membrane-derived dry matrix. Clin Ophthalmol. 2021;15:2231–2238. doi:10.2147/OPTH.S299141
- McDonald MB, Sheha H, Tighe S, et al. Treatment outcomes in the DRy Eye Amniotic Membrane (DREAM) study. Clin Ophthalmol. 2018;12:677–681. doi:10.2147/OPTH.S162203
- Pflugfelder SC, Baudouin C. Challenges in the clinical measurement of ocular surface disease in glaucoma patients. Clin Ophthalmol. 2011;5:1575–1583. doi:10.2147/OPTH.S24410
- Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature for Reporting Clinical Data. Results of the first international workshop. Am J Ophthalmol. 2005;140(3):509–516. doi:10.1016/j.ajo.2005.03.057
- OmniLenz bespoke bandage contact lens; 2023. Available from: https://www.nu-vision.co.uk/omnilenz. Accessed December, 2023.
- Huntjens B, Basi M, Nagra M. Evaluating a new objective grading software for conjunctival hyperaemia. Cont Lens Anterior Eye. 2020;43(2):137–143. doi:10.1016/j.clae.2019.07.003
- Haagdorens M, Van Acker SI, Van Gerwen V, et al. Limbal stem cell deficiency: current treatment options and emerging therapies. Stem Cells Int. 2016;2016:9798374. doi:10.1155/2016/9798374
- Tsai RJF, Tseng SCG. Effect of stromal inflammation on the outcome of limbal transplantation for corneal surface reconstruction. Cornea. 1995;14(5):439–449. doi:10.1097/00003226-199509000-00001
- Brija~ak M, Dekaris I, Gagro A, et al. Therapeutic effect of amniotic membrane in persistent epithelial defects and corneal ulcers in herpetic keratitis. Coll Antropol. 2008;32(Suppl. 2):21–25.
- Seitz B, Langenbucher A, Nguyen NX, Ro ̈mer AK, Ku ̈chle M, Naumann GOH. Risk factors for new corneal epithelial defects after penetrating keratoplasty. AAO-poster, Abstract; 168; 2003.
- Chiang CC, Chen WL, Lin JM, Tsai YY. Allogeneic serum eye drops for the treatment of persistent corneal epithelial defect. Eye. 2009;23(2):290–293. doi:10.1038/sj.eye.6703079
- Giannaccare G, Versura P, Buzzi M, Primavera L, Pellegrini M, Campos EC. Blood derived eye drops for the treatment of cornea and ocular surface diseases. Transfus Apher Sci. 2017;56(4):595–604. doi:10.1016/j.transci.2017.07.023
- Abdelghany AA, Bahrawy ME, Alio JL. Combined platelet rich plasma and amniotic membrane in the treatment of perforated corneal ulcers. Eur J Ophthalmol. 2022;32(4):2148–2152. doi:10.1177/11206721211049100
- Rüfer F, Schröder A, Erb C. White-to-white corneal diameter: normal values in healthy humans obtained with the Orbscan II topography system. Cornea. 2005;24(3):259–261. doi:10.1097/01.ico.0000148312.01805.53
- Lazreg S, Labetoulle M, Renault D, Baudouin C. Fast and sustained healing of resistant corneal ulcers using corneal scrubbing and matrix regenerating therapy. Eur J Ophthalmol. 2021;31(3):959–966. doi:10.1177/1120672120921379