Abstract
Background
The purpose of this paper is to report the successful treatment of corneal scarring and high corneal astigmatism secondary to previous pterygium surgery with diamond burr superficial keratectomy using mitomycin C.
Methods
Four patients with corneal scarring and high corneal astigmatism related to previous pterygium surgery underwent diamond burr superficial keratectomy with application of mitomycin C. Anterior segment photography and corneal topographic analysis were obtained preoperatively and postoperatively in all patients.
Results
Six months after surgery, corneal astigmatism and corneal aberrations were reduced in all patients. A clear cornea was achieved in all cases. No complications were noted during the follow-up period.
Conclusion
Diamond burr superficial keratectomy with application of mitomycin C is a potentially effective and simple procedure for treating patients with corneal scarring and high corneal astigmatism secondary to previous pterygium surgery.
Introduction
Pterygium is an ocular surface disorder seen frequently in ophthalmology practice. It has a considerable negative effect on corneal refractive status, which has been previously reported in various studies on refraction, keratometry, and corneal topography.Citation1 Pterygium may cause visual impairment by local flattening of the cornea and inducing with-the-rule astigmatism.Citation2,Citation3
Previous studies have demonstrated that the topographical changes in the cornea and visual impairment induced by pterygium can be reversed following removal.Citation2,Citation3 However, sometimes a pterygium surgery that was not performed effectively causes a remnant pterygium tissue on the cornea, which leads to corneal scarring, high astigmatism, and reduced visual function. Few studies have been reported in the literature related to corneal scarring and high corneal astigmatism secondary to pterygium surgery and their treatment.
Herein we report four cases with corneal scarring and high corneal astigmatism caused by pterygium remnant after pterygium surgery and treatment of these conditions with diamond burr superficial keratectomy and application of mitomycin C.
Materials and methods
Retrospective chart analysis was performed for four patients who were referred to our hospital for treatment of corneal scarring and high corneal astigmatism secondary to residual pterygium tissue after pterygium surgery. Phototherapeutic keratectomy was offered to all the patients by previous clinics. The advantages and disadvantages of our treatment were fully explained, and informed consent was obtained from each patient.
After a complete history was taken, all patients underwent a comprehensive ocular examination. Anterior segment imaging was achieved by a high definition external camera and a corneal topographic analysis was performed using a Scheimpflug camera (Sirius, Costruzioni Strementi Oftalmici, Italy) with a Placido disc topographer at baseline and at postoperative follow-up.
Surgical procedure
All surgeries were performed with topical anesthesia by the same surgeon (EBO) at the Beyoglu Eye Research and Training Hospital. The corneal epithelium around the pterygium remnant was removed down to Bowman’s layer and residual pterygium tissue was scraped by a crescent knife. Diamond burr polishing was then performed to smooth the entire corneal surface. A handheld battery-driven ophthalmic burr with a 3.3 mm diameter diamond-dusted sphere was used to polish the corneal surface for approximately 10–15 seconds. To avoid haze, mitomycin C (0.2 mg/mL) was applied for one minute with a Weck-Cel® sponge (Beaver-Visitec International, Waltham, MA, USA) and the eye was thoroughly irrigated with balanced salt solution. A soft bandage contact lens was placed on the eye at the end of the procedure. Postoperatively, the patient was instructed to instill a topical steroid, a topical antibiotic, and artificial tears, each four times daily, for one month after surgery. The contact lens was removed five days after the procedure. The patients were followed for at least six months.
Results
Demographic characteristics and clinical outcomes for the patients are shown in . On refractive examination, four patients had low uncorrected and best spectacle-corrected visual acuity, which had improved by six months after surgery (). In all four patients, slit-lamp examination revealed corneal scarring and residual tissues in the area of previous pterygium tissue at baseline ( and ). At six months postoperatively, the corneal lesions were decreased or had disappeared. Corneal topographic evaluation revealed high corneal astigmatism and elevated high corneal aberrations ( and ). After surgery, the corneal astigmatism and corneal aberrations were reduced ().
Figure 1 Appearance of case 2 (A) before and (B) six months after surgery.
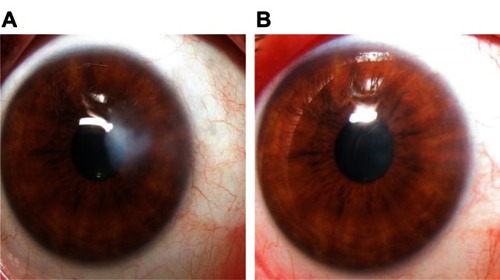
Figure 2 Appearance of case 3 (A) before and (B) six months after surgery.
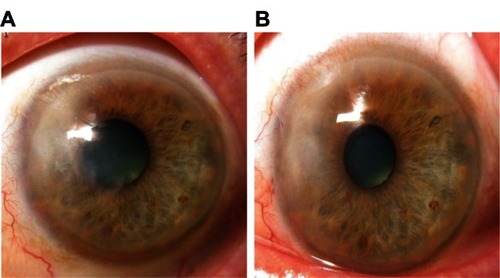
Figure 3 Corneal topography of case 1 (A) before and (B) six months after surgery.
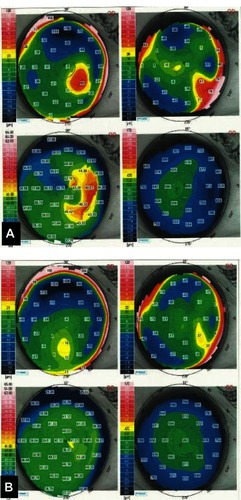
Figure 4 Corneal topography of case 2 (A) before and (B) six months after surgery.
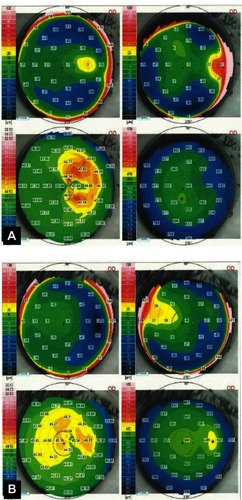
Table 1 Visual and refractive changes in patients before and six months after surgery
Table 2 Higher order corneal aberrations in patients before and six months after surgery
Discussion
Pterygium can induce a significant amount of astigmatism in proportion to its size. It generally causes with-the-rule corneal astigmatism that is hemimeridional on the side of the pterygium, which results in a localized flattening of the cornea central to the leading apex. Although many previous studiesCitation1,Citation2 have established that pterygium surgery decreases pterygium-induced astigmatism, corneal distortion may not be completely normalized in eyes with advanced pterygium, and irregular topographical changes may persist especially if the pterygium reached the paracentral zone of the cornea.Citation4 On the other hand, a pterygium remnant after pterygium surgery may cause visual impairment secondary to corneal scarring or induced astigmatism.
There are several modalities available to treat eyes with anterior corneal scars, which may be post-traumatic, post-infectious, or post-pterygium excision.Citation5,Citation6 Excimer laser phototherapeutic keratectomy is the most commonly recommended technique for superficial corneal opacities localized over one-third of the superficial stroma. Phototherapeutic keratectomy is also used to smooth irregular corneal surfaces caused by corneal disease, thereby improving the optical properties of the cornea and resulting in improved visual function.Citation7 Scars following pterygium surgery can be treated either as a primary scar or as a topography-guided treatment, with correction of irregular astigmatism.Citation5,Citation6
Herein we describe a simple, cheap, and effective procedure to treat anterior corneal scars and high corneal astigmatism related to previous pterygium surgery. Using this procedure, we achieved a decrease in corneal astigmatism and corneal aberrations, which resulted in visual improvement. This procedure has some advantages over phototherapeutic keratectomy. First, this technique does not induce a tissue reaction as in the case of excimer laser ablation. Second, the technique is cheaper than phototherapeutic keratectomy. Although requiring only a crescent knife and a handheld battery-driven ophthalmic burr, excimer laser phototherapeutic keratectomy requires more comprehensive equipment. Third, one of the difficulties with phototherapeutic keratectomy is preoperative estimation of the depth of pathology and determination of the amount of tissue to be removed during the procedure. However, this technique described here allows controlled scraping of the lesion.
This study has some limitations, including a small sample size and a short follow-up period. Larger studies with long-term follow-up are needed to validate our findings. Moreover, we did not address the safety of mitomycin C. Several studies have reported that use of topical mitomycin C during pterygium surgery had a deleterious effect on the corneal endothelium postoperatively.Citation8–Citation10
Conclusion
In conclusion, diamond burr superficial keratectomy with application of mitomycin C is a simple and effective procedure for treatment of corneal scarring secondary to previous pterygium surgery. This technique might be considered by surgeons in cases with anterior corneal scars related to pterygium surgery. However, larger prospective studies are required to confirm the effectiveness of the procedure.
Disclosure
The authors have no proprietary interests or conflicts of interest related to this work.
References
- YagmurMOzcanAASariSErsözTRVisual acuity and corneal topographic changes related with pterygium surgeryJ Refract Surg200521216617015796222
- CinalAYasarTDemirokATopuzHThe effect of pterygium surgery on corneal topographyOphthalmic Surg Lasers2001321354011195741
- PesudovsKFigueiredoFCCorneal first surface wavefront aberrations before and after pterygium surgeryJ Refract Surg200622992192517124890
- TomidokoroAOshikaTAmanoSEguchiKEguchiSQuantitative analysis of regular and irregular astigmatism induced by pterygiumCornea199918441241510422852
- MaloneyRKThompsonVGhiselliGDurrieDWaringGO3rdO’ConnellMA prospective multicenter trial of excimer laser phototherapeutic keratectomy for corneal vision loss: the Summit Phototherapeutic Keratectomy Study GroupAm J Ophthalmol199612221491608694083
- ZaidmanGWHongAVisual and refractive results of combined PTK/PRK in patients with corneal surface disease and refractive errorsJ Cataract Refract Surg200632695896116814053
- DogruMKatakamiCYamanakaARefractive changes after excimer laser phototherapeutic keratectomyJ Cataract Refract Surg200127568669211377896
- BaharIKaisermanILangeAPThe effect of mitomycin C on corneal endothelium in pterygium surgeryAm J Ophthalmol2009147344745218992871
- KheirkhahAIzadiAKiarudiMYNazariRHashemianHBehrouzMJEffects of mitomycin C on corneal endothelial cell counts in pterygium surgery: role of application locationAm J Ophthalmol2011151348849321236405
- AvisarRApelIAvisarIWeinbergerDEndothelial cell loss during pterygium surgery: importance of timing of mitomycin C applicationCornea200928887988119654528