
Abstract
Symptomatic vitreous opacities (SVO, “floaters”) in the mobile, aging vitreous that substantially interfere with daily visual activities (DVA) constitute degenerative vitreous syndrome (DVS). DVS is best distinguished from common “nuisance” floaters by use of “floater stories” written by presenting patients describing their symptoms. Here I discuss why vitreous opacity vitrectomy, though curative, has been adopted only belatedly and is still controversial, and I describe my long-term experience with its use for this disease.
QR Code

Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
© 2024 Morris. This work is published by Dove Medical Press Limited, and licensed under Creative Commons Attribution – Non Commercial (unported, v3.0) License. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed.
Introduction
Lens opacities of aging (cataracts) are commonly removed and replaced with a clear lens implant. Opacities in the vitreous gel behind the lens (“floaters”) are usually minimal and upon examination are typically considered insignificant.
Symptomatic vitreous opacities (SVO, herein synonymous with “floaters”) in the mobile, aging vitreous that substantially interfere with daily visual activities are relatively rare and are only recently receiving widespread attention. Here I discuss why vitrectomy - the only procedure that predictably cures extensive vitreous opacities () - has been adopted only belatedly and is still controversial. And I describe my long-term experience with its use for this disease.
Figure 1 (A) [Before] Image of Vitreous Opacity Vitrectomy (VOV) removing extensive vitreous opacities. (B) [After] Image of a clear visual axis following VOV.
![Figure 1 (A) [Before] Image of Vitreous Opacity Vitrectomy (VOV) removing extensive vitreous opacities. (B) [After] Image of a clear visual axis following VOV.](/cms/asset/38bb2f70-f67b-4cbe-80e0-a53fc99522f0/doph_a_12303403_f0001_c.jpg)
Why did nearly three decades elapse between the advent of pars plana vitrectomy and the first publication, in the year 2000, of its use to remove (chronic) floaters?Citation1,Citation2
Why were only seven “floater vitrectomy” articles published during the next eight years, while during the same period over seven hundred articles were published on similarly elective vitrectomy for macular pucker?Citation3
And eight years after the American Society of Retina Specialists chose our floater vitrectomy video for the 2007 Buckler award (the first time an ophthalmic society acknowledged floater vitrectomy as reasonable),Citation4 why did 75% of surveyed retina specialists still respond that they were unlikely to perform floater vitrectomy?Citation5
In order of frequency, these physicians’ answers were 1) the risks of vitrectomy, 2) unrealistic patient expectations, and 3) fear of ridicule by colleagues. Moreover, the authors of this 2015 report described floater vitrectomy as “immensely controversial”.Citation5
Who Needs Vitrectomy?
I have performed vitrectomy for symptomatic floaters since 1990, almost always in patients over 50 years of age, and more commonly in recent years, due to the availability of technologically advanced 27-gauge vitrectomy. My experience is that unrecruited patients with primary complaints attributable to chronic floaters rarely have “unrealistic expectations”. They remember continuously clear vision, and they are simply seeking to regain it.
I learned this by “deep listening” to patient’s “floater stories” (of symptoms) before the era of sophisticated imaging and the ubiquitous use of questionnaires attempting to measure “quality of life” effects.Citation6 To a sufficiently attentive and receptive physician their suffering was authentic and undeniable, yet these patients were then often regarded as obsessive or neurotic.Citation7
But much more often they were normal people who had been rejected for treatment elsewhere, likely because between floaters they still measured “20/20” on standard visual acuity testing.Citation3,Citation4 They had commonly been told, “You don’t have a problem”, or “The floaters will go away”, or “You’ll get used to them”, or “Nothing can be done”, or “There’s an operation but it’s too risky”. And they were desperate not to live the remainder of their lives dodging continual visual obscurations caused by vitreous opacities, daylight to dark.
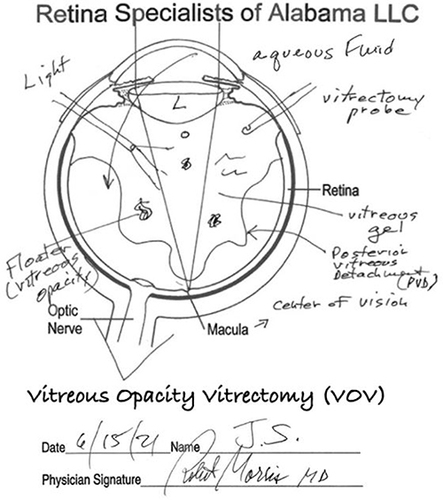
Once vitreous examination confirmed opacities correlating with a patient’s substantial symptoms, I simultaneously explained and drew the vitrectomy operation and described its risks (). I then asked patients to “go home and write your floater story before we come to a final decision”. In so doing they confronted their visual disability more directly than ever before.
Figure 2 Drawing of the VOV operation created by Robert Morris, MD.
Each floater story served a patient education and documentation purpose and helped me analyze the potential benefit before offering treatment. And patients were better able to answer the question, “Am I willing to accept the (percentage) risk of possible vision loss to regain continuously clear vision”, as we made a final decision together, to either treat or observe. I still use floater stories today to help identify appropriate patients for treatment (see https://www.floaterstories.com) and it is rare for a patient so selected to be dissatisfied with a treatment outcome.
Surgical Risks
Regarding the risks of vitrectomy, iatrogenic retinal tears have historically been of most concern. Carter, Michels et al reported a 4% incidence of peripheral retinal tears in 1990, most commonly behind entrance sites.Citation8 But cannulated, small gauge vitrectomy using high-speed cutting has since substantially reduced this complication. And wide-angle intraoperative microscopy of the peripheral retina can now assure discovery and prophylactic treatment of any new tear or existent lesion with far better visualization than was possible in the clinic preoperatively.
In 2022, I published, “Vitreous Opacity Vitrectomy (VOV): Safest Possible Removal of “Floaters”.Citation3 The methods described therein can now reduce the risks of elective vitrectomy to ~1% in patients over age 60 with posterior vitreous detachment (PVD), who constitute over 90% of presenting cases. This is similar to the risks of cataract extraction (CE), now enabling treatment of substantial SVO with an acceptably low complication rate.
In a recent series of 100 consecutive cases (mean age 66 years),Citation3 70 eyes were pseudophakic, 15 eyes underwent combined VOV/CE, and 13 eyes underwent CE within two years. PVD was present in 95% of eyes, making VOV inherently safer than in younger eyes with persistent vitreoretinal attachment. No retinal detachments occurred within one year postoperatively.
Increased understanding of the benefits of treating SVO and the reduced risks of modern VOV are now driving its greater acceptance among both general practitioners and retinal specialists.Citation9 Consequently, patients are now usually referred promptly by the initial provider to whom they present. Most affected eyes are pseudophakic,Citation3 but concomitant cataract can be treated (CE) simultaneously, or subsequently if there is progression.
Degenerative Vitreous Syndrome (DVS)
In the 2007 video mentioned above we introduced the term, “degenerative vitreous syndrome” (DVS, the spontaneous occurrence in the aging vitreous of opacities that substantially interfere with daily visual activities).Citation3,Citation4 DVS is thus distinguished from common nuisance floaters that have long been trivialized (“Oh, you just have floaters”). In this context, the term “severe floaters” would be an oxymoron.
DVS is defined subjectively by the treating physician and the informed patient, each appropriately deciding what is “substantial”, before offering treatment and before accepting treatment risks, respectively. This is true irrespective of whether a patient’s vitreous opacities or symptoms satisfy subjectively chosen numbers generated by “objective” imaging or questionnaires.
Because one patient’s daily visual activities are more challenging, their symptoms may be substantial from vitreous opacities measuring similarly to those that another patient would tolerate relatively easily, making the objective measurement of floaters and their symptoms superfluous. Yet parallel to our use of floater stories to assess and document DVS, various vision researchers still obsessively pursue measurement of vitreous opacities,Citation10 while others attempt to measure floater-related symptoms using “quality of life” questionnaires.Citation6
Both efforts reflect the discomfort of complete reliance on the history and physical examination that remain, however, the keys to individual treatment decisions, better than any measurements derived from them.Citation11 Similarly, the Medicare criteria for cataract extraction are also now primarily symptom based.Citation12
Conclusion
In summary, only a patient’s symptoms documenting substantial interference with daily visual activities and clinically correlated with vitreous opacities are sufficient, indispensable, and treatment actionable. Moreover, VOV treatment of such patients reliably restores continuously clear vision and is highly cost effective.Citation13
Measurements serve a useful research purpose in this disease. But no number in any grading system will ever guide individual treatment of symptomatic vitreous opacities better than a patient’s own words.Citation11
Disclosure
The author reports no conflicts of interest in this work. The website referenced in the article (https://www.floaterstories.com) is sponsored by the Helen Keller Foundation as a public service. The author is President of the Foundation and assisted in development of this website.
Acknowledgments
The author would like to acknowledge the DVS patients who eventually found the path back to continuously clear vision through vitrectomy.
References
- Machemer R, Buettner H, Norton EW, Parel JM.Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolary. 1971;75(4):813–820.
- Schiff WM, Chang S, Mandava N, Barile GR. Pars plana vitrectomy for persistent, visually significant vitreous opacities. Retina. 2000;20(6):591–596. PMID: 11131410. doi:10.1097/00006982-200011000-00001
- Morris RE. Vitreous Opacity Vitrectomy (VOV): safest Possible Removal of “Floaters”. Clin Ophthalmol.;16:1653–1663. PMID: 35673347; PMCID: PMC9167598. doi:10.2147/OPTH.S361557
- Morris RE, Witherspoon CD, Kimble J, Kuhn F, Roberts D, Sapp MR. Vitreous Opacity Vitrectomy (VOV) for Degenerative Vitreous Syndrome (DVS) – let’s talk about floaters. In: Video Submission, American Society of Retina Specialists 25th Annual Meeting. California, USA: Indian Wells; 2007.
- Cohen MN, Rahimy E, Ho AC, Garg SJ. Management of symptomatic floaters: current attitudes, beliefs, and practices among vitreoretinal surgeons. Ophthalmic Surg Lasers Imaging Retina. 2015;46(8):859–865. PMID: 26431302. doi:10.3928/23258160-20150909-11
- Jong JE W-D, Manning-Charalampidou SS, Vingerling H, Busschbach JJ, Pesudovs K. Patient-reported outcomes in patients with vitreous floaters: a systematic literature review. Surv Ophthalmol. 2023;68(5):875–888. PMID: 37315741. doi:10.1016/j.survophthal.2023.06.003
- Hoerauf H. Vitrectomy against floaters. In: Kirchhof B, Wang D, editors. Essentials in Ophthalmology; Vitreoretinal Surgery. New York, USA: Springer; 2007:115–124.
- Carter JB, Michels RG, Glaser BM, De Bustros S. Iatrogenic retinal breaks complicating pars plana vitrectomy. Ophthalmology. 1990;97(7):848–854. PMID: 2381696. doi:10.1016/s0161-6420(90)32492-2
- D’Amico D. Survey findings on vitreous opacities and panel of experts discussion. supplemental report. Retina Today; 2021.
- Stanga PE, Valentin Bravo FJ, Reinstein UI, et al. New terminology and methodology for the assessment of the vitreous, its floaters and opacities, and their effect on vision: standardized and kinetic anatomical and functional testing of vitreous floaters and opacities (SK VFO Test). Ophthalmic Surg Lasers Imaging Retina. 2023;54(5):306–315. doi:10.3928/23258160-20230412-02
- Floater Stories. Available from: https://floaterstories.com. Accessed 12, November, 2023.
- Medicare Guidelines for Local Coverage Determination for Cataract Extraction(including Complex Cataract Extraction). Centers for Medicare and Medicaid Services (CMS). Available from: https://www.cms.gov/medicare-coveragedatabase/view/lcd.aspx?lcdid=35091. Accessed 12, November, 2023.
- Rostami B, Nguyen-Cuu J, Brown G, Brown M, Sadun AA, Sebag J. Cost-Effectiveness of Limited Vitrectomy for Vision-Degrading Myodesopsia. Am J Ophthalmol. 2019;204:1–6. doi:10.1016/j.ajo.2019.02.032