
Abstract
To review the latest surgical advances and evolving clinical use of scleral bio-tissue for reinforcement in the eye and review the published literature on novel surgical applications of scleral allograft bio-tissue. Conventional surgical procedures for scleral reinforcement using homologous scleral allograft have been traditionally ab-externo interventions comprising of anterior or posterior reinforcement of the sclera for clinical indications such as trauma, scleromalacia, glaucoma drainage device coverage, scleral perforation, buckle repair as well as posterior reinforcement for pathologic myopia and staphyloma. There have been a few novel ab-interno uses of scleral bio-tissue for reinforcement in both retina and glaucoma. Over the last decade, there has been an increase in peer-reviewed publications on scleral reinforcement, reflecting more interest in its clinical applications. With favorable biological and biomechanical properties, scleral allograft may be an ideal substrate for an array of new applications and surgical uses.
Background
The history of donor scleral allograft tissue use goes back over half a century as a durable biocompatible material widely used in ophthalmic surgery.Citation1 Scleral tissue has been used for multiple purposes in ophthalmology, predominantly in glaucoma surgery, such as glaucoma drainage devices (GDDs) implantation, where a scleral patch is used to cover the tube reducing the rates of erosion.Citation2–4 Providing structural integrity is also an important indication for scleral graft use, as in conditions where scleral thinning is present with an imminent risk of perforation.Citation5–7 Unlike donor cornea, scleral allograft tissue is readily available, representing 4–5% of total eye bank tissue allocations, and the use of sectional donor tissue allows the eye banks to maximize the sclera tissue obtained from a single donor.Citation8 Furthermore, the tissue is immunologically safe and easy to process and transport, with a shelf life exceeding 1year when stored in optimal conditions.Citation9,Citation10
Scleral Anatomy
The sclera is a dense connective tissue that corresponds to more than 80% of the outer surface area of the globe, with the main function of providing a firm substrate to protect the intraocular structures.Citation11 It comprises three layers: episclera, stroma and inner sclera (lamina fusca). The episclera is more of an envelope not inherent to the scleral biomatrix and corresponds to a layer of connective tissue that is highly vascularized. The stroma is the major scleral tissue layer, essentially avascular and acellular. It is composed of a dense collagenous structure, mainly type I and III collagen and proteoglycans.Citation12 The dense connective tissue provides the sclera the biomechanics properties of being flexible yet durable. The lamina fusca represents a thin, avascular, brown layer on the inner surface of the sclera. The sclera thickness varies across the surface from 0.3 mm at its thinnest at the attachment of the rectus muscles to more than 1.2 mm posteriorly.Citation11,Citation12 There are significant variations in scleral thickness and rigidity between individuals.Citation13 Previous studies have shown that the sclera composition and elasticity are variable in normal patients and are altered with aging.Citation13,Citation14 The sclera tissue is hydrophilic, porous, and has a relatively high permeability, which is why transscleral drug delivery is under increasing interest.Citation15,Citation16
Scleral Allograft Properties
Scleral allograft tissue has important properties, making it useful and desirable as a bio-tissue substrate for structural reinforcement and reconstruction. Many of the advantages of the use of sclera tissue are being readily available from donor eyes, easy to manipulate, and well tolerated with minimal inflammatory reaction.Citation6,Citation12 The essential acellular nature is important as it has limited risk of having antigen-presenting cells and has a low immunogenic profile, further enhanced by the sterilization process.Citation17,Citation18 Scleral allograft () is non-biodegradable and has high structural integrity, a high tensile strength and non-brittle, leathery physical properties, making it resilient and an ideal substrate for structural reinforcement.Citation12,Citation19 Its flexibility and conformability enable a wide range of surface applications when used to patch graft a scleral wall defect. In addition, the sclera is highly permeable and hydrophilic, with important properties regarding aqueous conductivity for bio-stenting and outflow maintenance and scaffolding.Citation15,Citation16 It is homologous and native to the surrounding tissue when used for endo- or epi-scleral reinforcement. This happens to be of further importance regarding implant fibrosis as homologous scleral tissue has one of the lowest index of material stiffness mismatch when implanted adjacent to the scleral surface, thereby reducing the potential for fibrosis and macrophage activation as compared to synthetic implants composed of rigid materials like metal or plastic.Citation20,Citation21
Figure 1 Scleral patch graft.

Sterilization and Storage of Scleral Allograft
The donor selection and screening process follows U.S Food and Drug Administration (FDA) regulations and the Eye Bank Association of America (EBBA) standards. A serum sample from the donor is tested for HIV, Hepatitis B and C and Syphilis.
It is important to ensure that the tissue sterilization and storage method does not change the structural properties of sclera, which could compromise its performance. The ideal method should combine the maximum capacity to eliminate pathogens while keeping the scleral integrity as much as possible. Sterilization with gamma radiation allows for reliable long-term storage and has become the standard method for sclera storage.Citation22 The use of gamma-irradiated tissue has the advantage of inactivating most pathogens, decreasing the risk of disease transmission, and is a highly standardized process consistent with the sterilization of most medical devices.Citation23 Several methods have been described for scleral tissue storage, including short-term storage (up to 30 days) using sterile saline with gentamicin and longer storage, allowing the tissue to be easily stored for up to 2 years.Citation9,Citation10,Citation24,Citation25 The last can be achieved using glycerin, 95% ethanol or freeze-drying. Glycerin has traditionally been used for scleral storage, having a great ability to maintain structural integrity compared to other storage methods.Citation17 However, it can be ineffective for the inactivation of some organisms, like specific viruses and prions. Alcohol preservation (ethanol 70–95%) offers robust tissue sterilization and is a simple, cost-effective methodology. Soaking the tissue for 40 minutes in basic saline solution before clinical use is recommended, effectively removing all traces of ethanol.Citation10
Clinical Applications of Scleral Allograft for Ab-Externo Reinforcement
Several alternatives exist, but sclera tissue remains popular due to its strength, availability, ease of use, and storage. Conventional use over the last several decades has been mostly through an ab-externo approach to reinforce the ocular surface and the integrity of the scleral interface/wall and protect the ocular tissues from the erosive effects of implantable hardware such as glaucoma drainage devices.Citation1,Citation2,Citation5
Use for Scleral Reinforcement of Glaucoma Drainage Devices
For a few decades, glaucoma drainage devices (GDD) have been used to surgically control IOP in patients with glaucoma. Amongst the complications associated with these devices, tube exposure is potentially vision-threatening and poses a risk for the development of endophthalmitis.Citation23 Rates of tube exposure in the literature range from 3–9% in the first 5 years,Citation1–4 with younger age and preoperative inflammation considered as risk factors for an erosion.Citation26 The rates of exposure between different GDDs appear to be similar.Citation27
Using a biotissue, like sclera, to cover the tube can potentially decrease conjunctiva erosion.Citation28 Other tissues, such as the cornea, pericardium, fascia lata and dura mater, are also available.Citation29 Choosing the ideal tissue for tube coverage is critical, and sclera seems to provide a firm and durable coverage for GDD. A study comparing the pericardium and sclera graft for tube cover showed that patch thinning occurred faster in the pericardium group (33 months) compared to sclera (66 months).Citation2 Scleral graft has also been used during scleral fistula closure at the time of tube repositioning during surgical revision.Citation30 One specific disadvantage of the scleral graft is the thickness and color, which may be a cosmetic issue.
Use for Scleral Reinforcement in Post-Trabeculectomy Revision Procedures
Scleral allograft can also be helpful in trabeculectomy revision procedures. Chronic thinning and disintegration of the scleral flap and conjunctival tissues after trabeculectomy can result in late bleb leakage, and antifibrotic adjuvants can increase the risk of those complications.Citation31 Managing hyperfiltration or bleb leakage is always a challenge, and using a scleral patch graft in trabeculectomy revisions can offer a long-term solution for hypotony. Previous studies have shown good outcomes when using a scleral patch associated with conjunctiva advancement for managing late bleb leaks and hypotony for overfiltration.Citation32,Citation33
Use for Scleral Reinforcement Due to Scleral Thinning and Necrosis
Scleral thinning is a well-reported complication following pterygium excision, retinal detachment repair, systemic vasculitis, scleritis, high myopia, or trauma. In rare cases, it results in staphyloma formation, scleral perforation, and uveal exposure.Citation5,Citation7,Citation8 Reinforcement of thin or perforated sclera is necessary and is considered an ophthalmic emergency. Scleral allograft has been successfully used to treat corneoscleral pathology such as scleral perforations, corneoscleral melts, scleromalacia, as well as in the repair of intercalary staphyloma, which forms between the ciliary body and the limbus in patients with Marfan’s syndrome.Citation6,Citation34,Citation35
Use of Donor Sclera to Coat Orbital Implants
The sclera is also widely used in oculoplastics for wrapping orbital implants after enucleation.Citation36 Coating orbital implants with scleral graft reduces the risk of implant exposure and rejection.Citation37
Use of Donor Sclera in Oculoplastic Applications
Scleral allograft has been used in the treatment of cicatricial entropion. While not a common application today, surgical splicing of the graft to the tarsoconjunctival layer of the entropic eyelid allows spontaneous epithelialization and anatomic recovery of the eyelid architectureCitation38,Citation39 Scleral allograft has proven to be excellent substrate as a spacer for eyelid reconstruction surgery in cases of upper and lower lid retraction.Citation40 A retrospective review by Feldman et alCitation41 on the use of donor sclera as a spacer graft in eyelid retraction surgery is informative of the long term outcomes with scleral allograft as well as the evolution of the surgical technique over time.
Novel Applications of Scleral Allograft for Ab-Interno Reinforcement
More recently, ab-interno surgical applications are opening new possibilities for advanced surgical techniques allowing intraocular use of scleral tissue. When minimally modified to precise geometries and delivered with ab-interno micro-interventional instrumentation, the scleral bio-tissue can provide durable and non-resorbable structural reinforcement for glaucoma and retina surgical applications. The biomaterial properties of the scleral graft can enable a new frontier of clinical utility for both conductive and/or occlusive scaffolding with intraocular implantation.
Retinal Applications
In the surgical retinal field, scleral patch can be used to manage optic disc pit maculopathy.Citation42 In a case series, the use of autologous scleral patch has shown to be well tolerated in the posterior segment when implanted into the optic disc pit (ODP) to occlude (“plug”) subretinal cerebrospinal fluid leakage and resolve the fluid accumulation.Citation42,Citation43 Better resolution of the maculopathy was seen when vitrectomy with internal limiting membrane (ILM) peeling was combined with ODP plug compared to the procedure without the plug.Citation43 Another example is an ab-interno endoscleral patch graft for a leaking sclerotomy that could not be sutured closed because of necrosis of the surrounding tissue.Citation44
Glaucoma Applications
In glaucoma, the uveoscleral outflow can be enhanced by creating a cyclodialysis cleft to surgically control intraocular pressure, first described by Heine in 1905.Citation45 While effective in lowering the IOP, durability was limited due to spontaneous closure of the cyclodialysis cleft.Citation46 Devices targeting the suprachoroidal space were developed to prevent cleft closure and may offer more predictable and sustained outcomes.Citation47–49 Synthetic suprachoroidal devices such as polyimide stents showed long-term outflow enhancement and sustained IOP reduction but were associated with accelerated endothelial cell loss in the cases where the implantable hardware was anteriorized and close to the cornea.Citation50 Further challenges with synthetic implants in the suprachoroidal space may be in part due to the significant stiffness mismatch between synthetic materials such as metal and plastic and the surrounding ocular tissue.Citation51,Citation52
Using scleral allograft to enhance uveo-scleral outflow is another promising clinical application of ab-interno scleral tissue reinforcement (). Homologous conforming bio-tissue has potential advantages over rigid implantable hardware devices because of its porosity, hydrophilic aqueous permeability and structural stability without the fibrosis-inducing bio-mechanical mismatch to the surrounding native tissues. Intraocular implantation of a scleral allograft in the supraciliary space has been shown to structurally enhance and maintain the suprachoroidal outflow because of the conductive and reinforcing properties of the allograft acellular matrix ().Citation53 Early results are encouraging in that respect - in a study with 12 months of follow-up, flexible conforming bio-tissue was well tolerated without anterior chamber inflammation, anterior synechiae or corneal adverse events. The allograft remained well positioned within the cyclodialysis cleft with no evidence of migration.Citation53
Figure 2 The scleral allograft microtrephined into a minimally-modified, bio-scaffolding implant. Photo courtesy with permission from Iantrek.
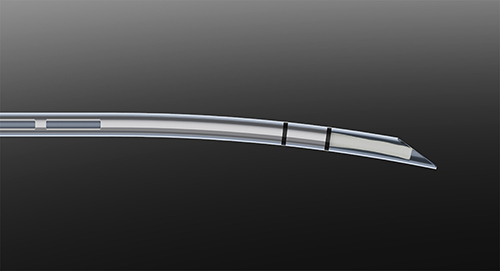
Figure 3 Scleral allograft used for intraocular reinforcement. (A) Gonioscopic image of two allograft spacers used for cyclodialysis bio-scaffolding and reinforcement. (B) OCT image of an allograft intraocular spacer (C) Scleral allograft bio-scaffolding spacer during ab-interno surgical deployment.
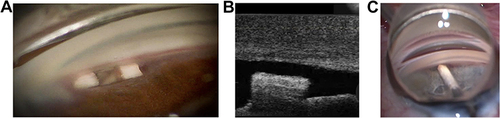
Different surgical techniques and allograft formulations have been developed in the effort to augment uveo-scleral outflow. In one application, scleral allograft tissue is minimally modified for optimal aqueous permeability which can allow its use as a conductive bio-stent in the supraciliary space.Citation53 In another formulation, allograft tissue is processed to maximize the structural integrity of the collagen matrix so it can be implanted as a scaffolding and reinforcement material of the cyclodialysis thus creating a durable supraciliary filtration reservoir for sustained aqueous outflow.Citation53 In the former approach, the primary outflow mechanism is through the porous bio-stent implant while in the latter, the outflow is mainly through the reinforced endogenous cyclodialysis.
Ab-interno scleral reinforcement may have other future applications for structural support, stabilization, stenting and other conductive or occlusive interventions in the management of hypotony, over-filtration or for enhanced aqueous outflow.
Conclusions
Scleral allograft has demonstrated excellent safety as an inert biocompatible and non-biodegradable material that can provide tectonic support and preserve the integrity of the scleral interface, as well as protect the ocular tissues from the erosive effects of implantable hardware such as glaucoma drainage devices. Novel applications of homologous scleral allograft for ab-interno reinforcement and scaffolding allow intraocular use of scleral tissue and have demonstrated promising results in the surgical treatment glaucoma and retina conditions.
Disclosure
Dr Ticiana De Francesco is a consultant to Iantrek, outside the submitted work. Dr Tsontcho Ianchulev reports patents for and is the founder of Iantrek Inc. Dr Douglas Rhee is a consultant to Iantrek, during the conduct of the study; grants from and a consultant to AbbVie / Allergan, Alcon, Ocular Therapeutix, and Avellino, outside the submitted work. Dr Louis Pasquale is a paid consultant to Twenty Twenty. Dr Ike Ahmed is a consultant to Iantrek. The authors report no other conflicts of interest in this work.
References
- Freedman J. Scleral patch grafts with Molteno setons. Ophthalmic Surg. 1987;18(7):532–534. PMID: 3627691.
- Wigton E, C Swanner J, Joiner W, et al. Outcomes of shunt tube coverage with glycerol preserved cornea versus pericardium. J Glaucoma. 2014;23(4):258–261. PMID: 22955016. doi:10.1097/IJG.0b013e31826a96e8
- Pakravan M, Yazdani S, Shahabi C, Yaseri M. Superior versus inferior Ahmed glaucoma valve implantation. Ophthalmology. 2009;116(2):208–213. PMID: 19062098. doi:10.1016/j.ophtha.2008.09.003
- Wishart PK, Choudhary A, Wong D. Ahmed glaucoma valves in refractory glaucoma: a 7-year audit. Br J Ophthalmol. 2010;94(9):1174–1179. PMID: 19965829. doi:10.1136/bjo.2009.165357
- Nguyen QD, Foster CS. Scleral patch graft in the management of necrotizing scleritis. Int Ophthalmol Clin. 1999;39(1):109–131. PMID: 10083910. doi:10.1097/00004397-199903910-00011
- Sangwan VS, Jain V, Gupta P. Structural and functional outcome of scleral patch graft. Eye. 2007;21(7):930–935. PMID: 16601740. doi:10.1038/sj.eye.6702344
- Karaca U, Usta G. The usability of lamellar scleral autograft in ocular perforation treatment. Int Ophthalmol. 2022;42(2):377–383. PMID: 34176032. doi:10.1007/s10792-021-01922-x
- Hodge C, Sutton G, Devasahayam R, et al. The use of donor scleral patch in ophthalmic surgery. Cell Tissue Bank. 2017;18(1):119–128. PMID: 27878655. doi:10.1007/s10561-016-9603-4
- Romanchuk KG, Nair P, Grahn B. How long can donor sclera be safely stored? Cornea. 2003;22(6):569–572. PMID: 12883353. doi:10.1097/00003226-200308000-00016
- Töteberg-Harms M, Bredehorn-Mayr T. Preparation and use of human sclera grafts in ophthalmic surgery. Dev Ophthalmol. 2009;43:105–108. Epub 2009 Jun 3. PMID: 19494641. doi:10.1159/000223843
- Watson PG, Young RD. Scleral structure, organisation and disease. A review. Exp Eye Res. 2004;78(3):609–623. PMID: 15106941. doi:10.1016/s0014-4835(03)00212-4
- Boote C, Sigal IA, Grytz R, Hua Y, Nguyen TD, Girard MJA. Scleral structure and biomechanics. Prog Retin Eye Res. 2020;74:100773. PMID: 31412277; PMCID: PMC7187923. doi:10.1016/j.preteyeres.2019.100773
- Rada JA, Achen VR, Penugonda S, Schmidt RW, Mount BA. Proteoglycan composition in the human sclera during growth and aging. Invest Ophthalmol Vis Sci. 2000;41(7):1639–1648. PMID: 10845580.
- Coudrillier B, Pijanka J, Jefferys J, et al. Collagen structure and mechanical properties of the human sclera: analysis for the effects of age. J Biomech Eng. 2015;137(4):041006. PMID: 25531905; PMCID: PMC4340195. doi:10.1115/1.4029430
- Olsen TW, Edelhauser HF, Lim JI, Geroski DH. Human scleral permeability. Effects of age, cryotherapy, transscleral diode laser, and surgical thinning. Invest Ophthalmol Vis Sci. 1995;36(9):1893–1903. PMID: 7543465.
- Prausnitz MR, Noonan JS. Permeability of cornea, sclera, and conjunctiva: a literature analysis for drug delivery to the eye. J Pharm Sci. 1998;87(12):1479–1488. PMID: 10189253. doi:10.1021/js9802594
- Schirmbeck T, Cruz AA. Biomechanical and histological evaluation of glycerol-preserved human sclerae. Arq Bras Oftalmol. 2007;70(6):988–990. PMID: 18235912. doi:10.1590/s0004-27492007000600019
- Coudrillier B, Tian J, Alexander S, Myers KM, Quigley HA, Nguyen TD. Biomechanics of the human posterior sclera: age- and glaucoma-related changes measured using inflation testing. Invest Ophthalmol Vis Sci. 2012;53(4):1714–1728. PMID: 22395883; PMCID: PMC3630906. doi:10.1167/iovs.11-8009
- Elsheikh A, Geraghty B, Alhasso D, Knappett J, Campanelli M, Rama P. Regional variation in the biomechanical properties of the human sclera. Exp Eye Res. 2010;90(5):624–633. PMID: 20219460. doi:10.1016/j.exer.2010.02.010
- Blakney AK, Swartzlander MD, Bryant SJ. The effects of substrate stiffness on the in vitro activation of macrophages and in vivo host response to poly(ethylene glycol)-based hydrogels. J Biomed Mater Res A. 2012;100(6):1375–1386. PMID: 22407522; PMCID: PMC3339197. doi:10.1002/jbm.a.34104
- Ayyala RS, Michelini-Norris B, Flores A, Haller E, Margo CE. Comparison of different biomaterials for glaucoma drainage devices: part 2. Arch Ophthalmol. 2000;118(8):1081–1084. PMID: 10922202. doi:10.1001/archopht.118.8.1081
- Fernandes JB, Matayoshi S, Osaka JT, Tolosa EC, Nunes TP, Moura Eda M. Comparative analysis between sclera treated with glycerin and sclera treated with gamma irradiation, alkali and glycerin in the reconstruction of anophthalmic socket: experimental study in rabbits]. Arq Bras Oftalmol. 2007. 70(4):639–647. Portuguese. PMID: 17906761. doi:10.1590/s0004-27492007000400015
- Miekka SI, Forng RY, Rohwer RG, et al. Inactivation of viral and prion pathogens by gamma-irradiation under conditions that maintain the integrity of human albumin. Vox Sang. 2003;84(1):36–44. PMID: 12542732. doi:10.1046/j.1423-0410.2003.00256.x
- Frota C, Lima Filho AA, Dias AB, Lourenço AC, Antecka E, Burnier MN. Freeze-drying as an alternative method of human sclera preservation. Arq Bras Oftalmol. 2008;71(2):137–141. PMID: 18516408. doi:10.1590/s0004-27492008000200002
- Colvard DM, Waller RR, Campbell RJ, Friedt R. Sterilization of scleral homografts with ionizing irradiation. Am J Ophthalmol. 1979;87(4):494–496. PMID: 443314. doi:10.1016/0002-9394(79)90237-x
- Chaku M, Netland PA, Ishida K, Rhee DJ. Risk factors for tube exposure as a late complication of glaucoma drainage implant surgery. Clin Ophthalmol. 2016;10:547–553. PMID: 27099461; PMCID: PMC4820194. doi:10.2147/OPTH.S104029
- Gedde SJ, Feuer WJ, Lim KS, et al.; Primary Tube Versus Trabeculectomy Study Group. Postoperative complications in the primary tube versus trabeculectomy study during 5 years of follow-up. Ophthalmology. 2022;129(12):1357–1367. PMID: 35835336; PMCID: PMC9691562. doi:10.1016/j.ophtha.2022.07.004
- Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed versus baerveldt study: five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. PMID: 27544023. doi:10.1016/j.ophtha.2016.06.035
- Smith MF, Doyle JW, Ticrney JW. A comparison of glaucoma drainage implant tube coverage. J Glaucoma. 2002;11(2):143–147. PMID: 11912362. doi:10.1097/00061198-200204000-00010
- Panarelli JF, Banitt MR, Sidoti PA. Scleral fistula closure at the time of glaucoma drainage device tube repositioning: a novel technique. Arch Ophthalmol. 2012;130(11):1447–1451. PMID: 23143444. doi:10.1001/archophthalmol.2012.2219
- Dubey S, Prasanth B, Acharya MC, Narula R. Conjunctival erosion after glaucoma drainage device surgery: a feasible option. Indian J Ophthalmol. 2013;61(7):355–357. PMID: 23571238; PMCID: PMC3759109. doi:10.4103/0301-4738.99852
- O’Rourke M, Moran S, Collins N, Doyle A. Bleb reconstruction using donor scleral patch graft for late bleb leak and hypotony. Eur J Ophthalmol. 2021;31(3):1039–1046. PMID: 32450728. doi:10.1177/1120672120924343
- Pathak Ray V, Badakere SV. Long-term outcomes of blebs repaired with scleral patch graft and conjunctival advancement in late-onset leak post-trabeculectomy. Indian J Ophthalmol. 2021;69(9):2496–2501. PMID: 34427251; PMCID: PMC8544101. doi:10.4103/ijo.IJO_148_21
- Oh JH, Kim JC. Repair of scleromalacia using preserved scleral graft with amniotic membrane transplantation. Cornea. 2003;22(4):288–293. PMID: 12792468. doi:10.1097/00003226-200305000-00002
- Sahay P, Dhanda S, Maharana PK, Titiyal JS. Intercalary staphyloma in Marfan syndrome: a dreaded complication of scleral incision. Indian J Ophthalmol. 2019;67(7):1161–1162. PMID: 31238437; PMCID: PMC6611239. doi:10.4103/ijo.IJO_1672_18
- Soll DB. Donor sclera in enucleation surgery. Arch Ophthalmol. 1974;92(6):494–495. PMID: 4279648. doi:10.1001/archopht.1974.01010010508009
- Inkster CF, Ng SG, Leatherbarrow B. Primary banked scleral patch graft in the prevention of exposure of hydroxyapatite orbital implants. Ophthalmology. 2002;109(2):389–392. PMID: 11825828. doi:10.1016/s0161-6420(01)00904-6
- Tenzel RR, Miller GR, Rubenzik R. Cicatricial upper lid entropion. Treated with banked scleral graft. Arch Ophthalmol. 1975;93(10):999–1000. PMID: 1180758. doi:10.1001/archopht.1975.01010020783008
- Dryden RM, Soll DB. The use of scleral transplantation in cicatricial entropion and eyelid retraction. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977;83(4 Pt 1):669–678. PMID: 898487.
- Doxanas MT, Dryden RM. The use of sclera in the treatment of dysthyroid eyelid retraction. Ophthalmology. 1981;88(9):887–894. PMID: 7301305. doi:10.1016/s0161-6420(81)80002-4
- Feldman KA, Putterman AM, Farber MD. Surgical treatment of thyroid-related lower eyelid retraction: a modified approach. Ophthalmic Plast Reconstr Surg. 1992;8(4):278–286. PMID: 1476977. doi:10.1097/00002341-199212000-00007
- Travassos AS, Regadas I, Alfaiate M, Silva ED, Proença R, Travassos A. Optic pit: novel surgical management of complicated cases. Retina. 2013;33(8):1708–1714. PMID: 23644559. doi:10.1097/IAE.0b013e31828e699c
- Babu N, Kohli P, Ramasamy K. Comparison of various surgical techniques for optic disc pit maculopathy: vitrectomy with internal limiting membrane (ILM) peeling alone versus inverted ILM flap ‘plug’ versus autologous scleral ‘plug’. Br J Ophthalmol. 2020;104(11):1567–1573. PMID: 32029434. doi:10.1136/bjophthalmol-2019-315075
- Joshi M, Iezzi R, Baratz KH. Endoscleral Patch Graft: a Novel Closure for Complex Pars Plana Scleral Defects. Ophthalmol Retina. 2017;1(6):564–566. PMID: 31047458. doi:10.1016/j.oret.2017.03.008
- Heine L. Die Cyklodialyse, eine neue Glaukomoperation. Deutsche Med Woch. 1905;31:824.
- De Francesco T, Ahmed IIK. Surgical augmentation of the suprachoroidal space: a novel material and implant. Clin Ophthalmol. 2023;17:2483–2492. PMID: 37637970; PMCID: PMC10456019. doi:10.2147/OPTH.S409958
- Vold S, Ahmed II, Craven ER, et al.; CyPass Study Group. Two-year COMPASS trial results: supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology. 2016;123(10):2103–2112. PMID: 27506486. doi:10.1016/j.ophtha.2016.06.032
- Ianchulev T, Weinreb RN, Kamthan G, Calvo E, Pamnani R, Ahmed IK. Biotissue stent for supraciliary outflow in open-angle glaucoma patients: surgical procedure and first clinical results of an aqueous drainage biostent. Br J Ophthalmol. 2023:bjo-2022–322536. Epub ahead of print. PMID: 36593090. doi:10.1136/bjo-2022-322536
- Denis P, Hirneiß C, Durr GM, et al. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br J Ophthalmol. 2022;106(1):65–70. PMID: 33011690; PMCID: PMC8685654. doi:10.1136/bjophthalmol-2020-316888
- Lass JH, Benetz BA, He J, et al. Corneal endothelial cell loss and morphometric changes 5 years after phacoemulsification with or without cypass micro-stent. Am J Ophthalmol. 2019;208:211–218. PMID: 31377278. doi:10.1016/j.ajo.2019.07.016
- Carnicer-Lombarte A, Barone DG, Dimov IB, et al. Mechanical matching of implant to host minimises foreign body reaction. bioRxiv. 2019;829648.
- Carnicer-Lombarte A, Chen ST, Malliaras GG, Barone DG. Foreign body reaction to implanted biomaterials and its impact in nerve neuroprosthetics. Front Bioeng Biotechnol. 2021;9:622524. PMID: 33937212; PMCID: PMC8081831. doi:10.3389/fbioe.2021.622524
- Ianchulev T, Ahmed II, Kamthan G, Calvo E, Pamnani R, Ahmed IK. Novel suprachoroidal biostent for reinforced cyclodialysis: microinterventional technique and first-in-human results. Am Acad Ophthalmol Meet. 2023;108(2):217–222.