
Abstract
Purpose
To determine if there was an association between severity of glaucoma and intraocular pressure (IOP) and medication (med) outcomes for patients in the ROMEO (Retrospective, Observational, Multicenter Evaluation of OMNI) study.
Setting
Eleven ophthalmology practices in 8 US states.
Design
Post-hoc analysis of all eyes enrolled and treated with ab interno canaloplasty and trabeculotomy in the retrospective, multicenter ROMEO study.
Methods
Eyes were grouped according to visual field mean deviation (MD): mild (MD better than −6 dB), moderate (MD between −6 and −12 dB), advanced (−12 dB or worse). IOP and med outcomes at 12 months were compared across groups. Least squares regression was used to assess the relationship of MD with month 12 IOP. Outcomes for 1st and last MD deciles were compared as a sensitivity analysis.
Results
One hundred and twenty-seven eyes were available for analysis including 79 mild, 42 moderate, 6 advanced. Most eyes had a reduction in IOP at Month 12 (70%) with most at 18 mmHg or less. Percentage IOP reduction was similar across the groups (mild 16.9%, moderate 18.6%, advanced 18.0%) with mean month 12 IOP between 14 and 16 mmHg. Medications were also reduced in all three groups; −0.8 (mild, P < 0.001), −0.55 (moderate, P < 0.05), and −1.0 (advanced, P = 0.139, ns). Regression analysis revealed no relationship between month 12 IOP and MD. Med reductions were observed for all groups with a reduction of 1 or more medications seen in (%, 95% CI) 69%, 59–79 (mild), 50%, 35–65 (moderate), and 60%, 21–99 (advanced). Secondary interventions tended to have greater incidence with worse MD likely reflecting lower desired IOP targets.
Conclusion
Analysis of data from the ROMEO study suggests that similar meaningful IOP and med reductions can be expected across the range of disease severity studied.
Introduction
Minimally invasive glaucoma surgery is generally positioned between the first-line treatments (drop or laser therapy) for early glaucoma, and traditional incisional surgery for advanced glaucoma. This positioning was formalized in a joint position statement from the American Glaucoma Society and the US Food and Drug Administration published in 2015.Citation1 However, MIGS usage has evolved with a more expansive role in the current treatment paradigm; the possibility for earlier surgical intervention is a common theme in discussions of MIGS.Citation2,Citation3 Concomitant use with cataract surgery has made glaucoma surgery an accepted option for patients with very mild disease, while demonstrated effectiveness for some MIGS has also been shown for standalone use in refractory glaucoma.Citation4–6 But what about advanced glaucoma? While sometimes conflated, refractory and advanced are not the same. Refractory glaucoma is simply glaucoma that is hard to control and, from a regulatory standpoint, includes eyes that have uncontrolled intraocular pressure (IOP) despite a prior traditional incisional surgery or cilioablative procedure and maximally tolerated medical therapy.Citation1 Advanced glaucoma can be refractory or not but has generally not been studied in MIGS. Limited available data suggest that there may be less favorable outcomes for advanced glaucoma where the visual field mean deviation was worse than −15 dB.Citation7 This could be due to a more extensively damaged distal outflow system in advanced glaucoma, including reduced patency of collector channels,Citation8,Citation9 or simply due to generally lower target pressures for such patients which would result in “failure” when additional surgical intervention is employed.Citation7 The ROMEO (Retrospective, Observational, Multicenter Evaluation of OMNI) study was the first multicenter study reporting outcomes for glaucoma patients that had undergone ab interno circumferential canaloplasty and trabeculotomy, either combined with cataract surgery or as a standalone procedure.Citation3,Citation8 The aim of the present post hoc analysis of data from the ROMEO studyCitation3,Citation10 was to see if there was an association between clinically important outcomes (IOP and medication reduction) and status of the patient visual field preoperatively.
Methods
All data were collected as part of the ROMEO study. ROMEO was a multicenter, IRB approved, retrospective case series conducted at 11 multi-subspecialty ophthalmology practices in the United States. ROMEO was approved by the WCG IRB (Puyallup, WA) and adhered to the tenets of the Declaration of Helsinki. Waiver of consent was granted by the IRB because of the retrospective and observational nature of the study. The study included primary open-angle glaucoma patients, (122 of 129, 95%) who had undergone canaloplasty and trabeculotomy with the OMNI Surgical System (Sight Sciences, Menlo Park, CA) either combined with cataract surgery or as a standalone procedure. As the patients in ROMEO were treated in the course of normal clinical practice and not within a prospective protocol-defined environment, there was no medication washout pre-operatively or at the Month 12 endpoint. Full eligibility criteria, a complete description of the OMNI surgical technique, the extent of the OMNI procedure for both canaloplasty and trabeculotomy, and the complete results for all pre-planned endpoints have been published previously.Citation3,Citation10 A single eye per patient was included and where both eyes would have qualified, the first eye treated was selected.
Eyes were grouped by the baseline visual field mean deviation (MD); better than −6 dB (mild), between −6 and −12 dB (moderate), and −12 dB or worse (advanced) in alignment with a commonly used glaucoma staging criterion.Citation11 Two eyes without a baseline visual field were excluded. A sensitivity analysis compared IOP and medication outcomes for the best and worst deciles grouped by MD.
SigmaStat 4.0 (Systat Software, Inc, San Jose, CA, USA) was used for statistical analyses. Mean IOP and mean ocular hypotensive medication use were calculated for each subgroup at baseline and Month 12. Patient-level IOP response was evaluated by plotting baseline IOP versus Month 12 IOP in a scatterplot. The number and proportion of eyes with an IOP reduction, no change, or an increase is reported for each subgroup. One-way ANOVA or Kruskal–Wallis ANOVA on ranks (where normality test failed) were used to evaluate difference between subgroups for IOP and medications at baseline and Month 12. One-tailed t-tests or Mann–Whitney rank sum tests were used to make within-subgroup comparisons between baseline and Month 12. A linear regression of baseline MD versus Month 12 IOP was used to evaluate the possible association between these variables.
Results
Patient demographics and baseline characteristics were overall similar between groups (). Most of the patients had mild glaucoma (n = 79, median MD −2.7 dB) followed by moderate (n = 42, median MD −8.0 dB) and advanced (n = 6, median MD −13.3). The balance between a combined procedure and standalone was even for the advanced subgroup with an increasing proportion of combination cases going from moderate to mild. Similarly, there was a trend to increasing age with increasing severity. The overwhelming majority in all subgroups had a diagnosis of primary open-angle glaucoma (POAG). While baseline IOP and medication use was similar in the mild and moderate groups, it was noticeably higher for advanced (20.0 mmHg on 2.8 medications versus 17.1 and 17.2 mmHg on 1.7 and 1.9 medications) although analysis of variance failed to detect a statistically significant difference between groups for either likely due to the small sample size for advanced and the consequent low statistical power for the test. Not unexpectedly, the proportion of patients requiring secondary intervention increased from mild to moderate to advanced.
Table 1 Patient Demographics and Characteristics
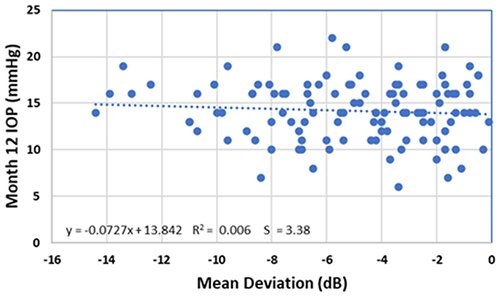
Mean IOP was significantly decreased for all three groups (−17.0 to −18.6%, P < 0.05 to P < 0.001) with Month 12 IOP at or near 14 mmHg for the mild and moderate groups and 16.4 mmHg for advanced. Mean baseline IOP for advanced was approximately 3 mmHg higher than for the other 2 cohorts (). A scatterplot of baseline IOP versus Month 12 IOP () shows that 92.4% of all patients had a Month 12 IOP of 18 or less, 70.3% of the patients had an IOP reduction, and 10.2% had no change in IOP. Of the 12 patients with no change in IOP, 10 of these had a reduction in medications; one medication decrease for 8, and 2 had a three or four medication reduction. Seven of these 12 were on zero medications at Month 12. Of note, only one eye in the advanced group did not have an IOP reduction and a Month 12 IOP below 18 mmHg. This eye went from 16 to 19 mmHg but medications were reduced from 4 to 1. Linear regression analysis did not suggest a relationship between visual field MD and IOP measured at Month 12 (). The least squares line is nearly horizontal and the r2= 0.006.
Figure 1 Mean IOP at Baseline (blue) and Month 12 (Orange) for Mild, Moderate and Severe groups. No significant difference between groups at Baseline or Month 12 (P = 0.213 and 0.269, respectively). * P<0.05, ** P<0.01, *** P<0.001.
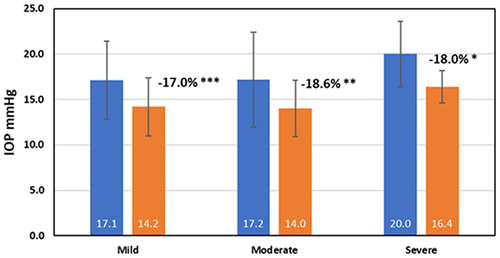
Figure 2 Scatterplot of Baseline IOP (x-axis) versus Month 12 IOP (y-axis) for Mild (black circles), Moderate (red circles), Advanced (blue circles). Diagonal is the line of no change. Dashed horizontal line at 18 mmHg.
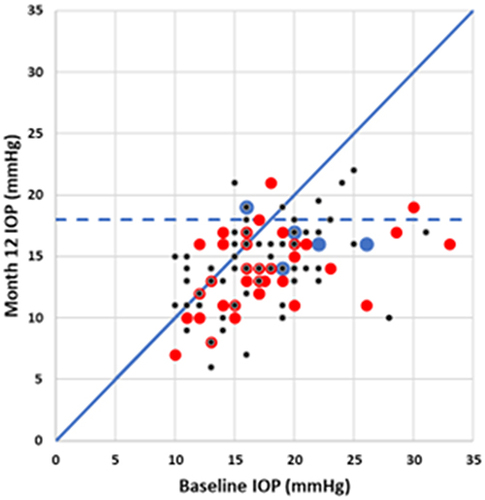
Figure 3 Scatterplot of Mean Deviation (x-axis) versus Month 12 IOP (y-axis). Dotted line is least squares regression line.
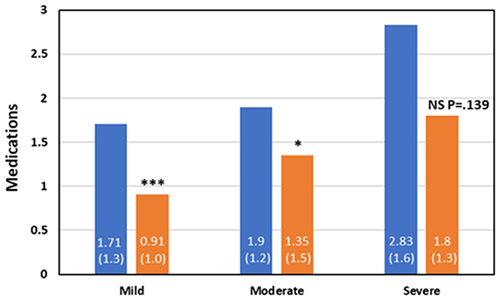
Decreases in mean medication usage were observed for all three cohorts (). These were 0.8 (mild, P < 0.001), 0.55 (moderate, P < 0.05), and 1.0 (advanced, P = 0.139, ns). The proportion of patients with a reduction of one or more medications (of those on at least one medication at baseline) was similar across groups (95% CI); 69% (59–79) (mild), 50% (35–65) (moderate), and 60% (21–99) (advanced).
Figure 4 Mean Medications at Baseline (blue) and Month 12 (Orange) for Mild, Moderate and Severe groups. No significant difference between groups at Baseline or Month 12 (P = 0.145 and 0.161, respectively). * P<0.05, *** P<0.001. Numbers in parentheses are standard deviations.
As a sensitivity analysis, IOP and medication reductions were evaluated for the 13 patients with the mildest (0.5 ± 2.7 dB) and the most advanced MD (−12.2 ± 1.4 dB). IOP and medications for the mildest decile went from 17.9 mmHg on 1.8 medications to 15.1 mmHg on 0.8 medications at 12 months. For the advanced group, these were 18.2 mmHg on 2.9 medications going to 15.1 mmHg on 1.6 medications. These results are consistent with the findings of the main analysis.
There were 9 secondary surgical interventions; 1 occurred in the six advanced patients (17%), 5 in 42 moderate patients (12%), and 3 in 79 mild patients (4%).
Discussion
MIGS has become an increasingly popular surgical option for glaucoma treatment since its introduction in the US in 2012. The increased safety of MIGS has been seen as a reasonable trade-off for less IOP-reduction when compared to trabeculectomy or tube shunts.Citation12 However, the use of MIGS in more advanced disease has been questioned due to concerns of efficacy. There is evidence that pressure related changes to the patency of the outflow system, and in particular the closing off of collector channel ostia are contributors to increased outflow resistance and it is reasonable to assume that in more advanced glaucoma where the pressure insult has been present for a longer period, these changes may be more profound.Citation8,Citation9,Citation13 Indeed, AGS-FDA guidelines discourage inclusion of patients with advanced glaucoma in MIGS implant clinical trials. However, the reasons given include the risk of progression resulting from medication washout periods, the possible randomization to a relatively ineffective control treatment (eg, cataract surgery only), and to protect patients from a potentially ineffective novel procedure.Citation1 While all three of these reasons make sense in the context of a randomized clinical trial for a new unproven procedure, they may not be valid in real-world medical practice with MIGS—a group of established procedures with known and documented effectiveness.
The OMNI surgical system has an indication for use that is not restricted to a specific stage or stages of disease.Citation14 Nevertheless, published studies have included mainly mild to moderate glaucoma. In the prospective GEMINI study eligibility was limited to mild and moderate glaucoma; the mean (SD) MD was −3.7 dB (3.6).Citation15 The TREY study was a retrospective multicenter study of OMNI used as a standalone treatment in patients who previously had a trabecular bypass stent and were no longer adequately controlled. There was no restriction for eligibility based on stage of disease and this was reflected in the patients enrolled; mean MD was −6.2 dB (7.0), with 7 of 27 (26%) categorized as advanced (MD < −12 dB, mean = −15.3 dB (2.6)). Interestingly, at last, follow-up, the advanced group had the lowest mean IOP (14.7 mmHg) and the greatest mean IOP reduction (−8.0 mmHg) when compared to the mild and moderate groups (18.3 mmHg, −5.5 mmHg, and 15.8 mmHg, −8.0 mmHg, respectively).Citation6 Similarly, in a 24-month retrospective study, Yadgarov et al found that canaloplasty + trabeculotomy with OMNI was equally effective in IOP-lowering across mild, moderate, and severe glaucoma. The advanced subgroup had the lowest mean IOP at 24 months, 13.0 mmHg, which may reflect treatment to a lower target IOP as this subgroup had greater average medication use (1.48 medications at 24 months versus 0.95 moderate and 0.31 mild).Citation16
Several other studies have found OMNI to be effective in patients with advanced glaucoma damage. Brown et al reviewed results with OMNI in a small cohort (41 eyes) that was primarily mild-moderate glaucoma but did include some with advanced disease (n was not reported). The authors found a significant linear relationship between preoperative IOP and post-operative IOP reduction with all data points clustered around the least-squares regression line which suggests that response to treatment was associated with starting IOP and not with stage of disease.Citation17 Bleeker et al retrospectively compared short-term 6-month IOP and medication outcomes for 27 eyes with mild-moderate disease and 16 with severe that were treated with 360 degree canaloplasty and 180 degree trabeculotomy using OMNI. While the severe group had higher baseline IOP and medication use (27.6 mmHg, 2.3 medications versus 20.8 mmHg, 2.0 medications), at Month 6 severe eyes averaged 12.7 mmHg and mild-moderate 16.7 mmHg; both groups averaged 1.6 medications.Citation18 Taken together, these studies suggest that IOP and medication outcomes for canaloplasty coupled with trabeculotomy using the OMNI are not correlated with glaucoma stage and that very good outcomes can be obtained across the disease severity spectrum. Our analysis of results from the ROMEO study are consistent with these other reports. In the present study, we failed to detect an association between effectiveness (or lack thereof) with visual field mean deviation.
The Grover et al study of GATT indicated a much higher probability of failure for the subgroup of patients with a pre-operative MD worse than −15 dB (approximately 80% probability of failure) than for the less advanced patients (20–40% probability of failure).Citation7 However, failure criteria were defined as a secondary surgery to control IOP or postoperative IOP that was not reduced by at least 20%, or was 21 mmHg or more at or after six months. The composite nature of this failure definition makes it difficult to separate the relative contributions of each of the failure modes. By this definition, an eye that had a pre-operative IOP of 18 mmHg which was decreased to 15 mmHg at 6 months (−17%) would be a failure equivalent to an eye that required a trabeculectomy at 6 months. Concluding that GATT was ineffective in advanced disease based on this analysis could be erroneous.
Additional insight can be obtained from the Grover et al study by comparing outcomes for subgroups with differing severity of MD.Citation7 POAG combined with cataract surgery and “Other” glaucoma combined with cataract surgery had mean MD of −6.5 dB and −11.8 dB but, despite this difference in mean MD, had very similar outcomes at 24 months.Citation7 The POAG combined group was 14.1 mmHg, 1.0 medications from 22.5 mmHg on 2.9 medications and the Other group was 14.5 mmHg on 1.2 medications from 25.7 mmHg on 3.0 medications. Viewed this way, the effectiveness appears to have been independent of MD.
The high failure rate noted by Grover et al in advanced glaucoma may instead reflect a higher incidence of secondary surgical intervention (SSI).Citation7 In OMNI studies, the incidence of SSI increases from GEMINI<ROMEO<TREY which parallels the average severity in these studies. The Yadgarov et al study also observed the highest incidence of SSI in the eyes with severe glaucomatous damage (11% vs 4 or 5%).Citation15 While one could conclude that canaloplasty + trabeculotomy is less effective in IOP and medication reduction with increasing severity, the data presented here argue against that. Another explanation is that the effectiveness bar is higher when glaucoma is advanced. Ophthalmologists set target pressures for patients based on the stage of the disease.Citation19 Achieving a 20% reduction in IOP and an IOP of 15 mmHg is likely fine for a mild or moderate patient but could be above target for a patient with advanced glaucoma and require further glaucoma surgery. Therefore, it is not surprising to see higher rates of SSI in advanced glaucoma; an indication of the general need for a lower target pressure rather than strictly a lack of effectiveness.
To date, there is limited data establishing the efficacy of MIGS in patients with advanced glaucoma. This analysis suggests that OMNI can be just as effective at lowering IOP and reducing medication usage in advanced glaucoma as it is in mild and moderate glaucoma. This study does have limitations that should be discussed. First, this is a post hoc analysis of a retrospective study. However, the study included all available eligible patients treated with OMNI thus mitigating the risk of selection bias. The study was multicenter mitigating the risk of investigator or center bias. Moreover, a retrospective study of patients treated in actual clinical practice, in our view, provides data more generalizable to the actual outcomes others may obtain with OMNI. Second, the majority of patients in this study were mild or moderate with a small number of patients having advanced visual field loss, extrapolation of these findings are therefore limited. Nevertheless, we feel confident that for the range of visual field deficits included, the study conclusions are valid.
Conclusion
The superior safety profile of MIGS compared to trabeculectomy and tube shunts makes it tempting to prefer MIGS in patients with advanced glaucoma. It is critically important to know whether MIGS is helpful in patients with advanced visual field loss. The concern about efficacy in advanced patients has led to speculation that there is something about the distal outflow pathway—which is not accessed by MIGS—that limits efficacy when glaucoma is advanced. The current study suggests that OMNI is still effective in patients with more extensive visual field damage. Confirmation of these results through additional studies, with a greater representation of patients with advanced field loss, is needed to determine the role of MIGS in glaucoma patients with advanced disease.
Disclosure
JED, AEH and RHB are employees of Sight Sciences. The authors report no other conflicts of interest in this work.
Data Sharing Statement
The authors do not intend to share participant-level data. Other queries or requests should be directed to the corresponding author (JD).
Additional information
Funding
References
- Caprioli J, Kim JH, Friedman DS, et al. Special commentary: supporting innovation for safe and effective minimally invasive glaucoma surgery: summary of a joint meeting of the American Glaucoma Society and the Food and Drug Administration, Washington, DC, February 26, 2014. Ophthalmology. 2015;122(9):1795–1801. doi:10.1016/j.ophtha.2015.02.029
- Radcliffe N. The case for standalone micro-invasive glaucoma surgery: rethinking the role of surgery in the glaucoma treatment paradigm. Curr Opin Ophthalmol. 2023;34(2):138–145. doi:10.1097/ICU.0000000000000927
- Hirsch L, Cotliar J, Vold S, et al. Canaloplasty and trabeculotomy ab interno with the OMNI system combined with cataract surgery in open-angle glaucoma: 12-month outcomes from the ROMEO study. J Cataract Refract Surg. 2021;47(7):907–915. doi:10.1097/j.jcrs.0000000000000552
- Yang SA, Mitchell W, Hall N, et al. Trends and usage patterns of minimally invasive glaucoma surgery in the United States: IRIS® registry analysis 2013–2018. Ophthalmol Glaucoma. 2021;4(6):558–568. doi:10.1016/j.ogla.2021.03.012
- Sarkisian SR, Mathews B, Ding K, Patel A, Nicek Z. 360° ab-interno trabeculotomy in refractory primary open-angle glaucoma. Clin Ophthalmol. 2019;13:161–168. doi:10.2147/OPTH.S189260
- Terveen DC, Sarkisian SR, Vold SD, et al. Canaloplasty and trabeculotomy with the OMNI surgical system in OAG with prior trabecular microbypass stenting. Int Ophthalmol. 2023;43(5):1647–1656. doi:10.1007/s10792-022-02553-6
- Grover DS, Smith O, Fellman RL, et al. Gonioscopy-assisted transluminal trabeculotomy: an ab interno circumferential trabeculotomy: 24 months follow-up. J Glaucoma. 2018;27(5):393–401. doi:10.1097/IJG.0000000000000956
- Aktas Z, Ozmen MC, Atalay HT, Ucgul AY. Evaluation of the episcleral venous wave during gonioscopy assisted transluminal trabeculotomy in patients with advanced glaucoma. Eye. 2019;33(4):668–673. doi:10.1038/s41433-018-0254-5
- Elhusseiny AM, Jamerson EC, Menshawey R, Tam EK, El Sayed YM. Collector channels: role and evaluation in Schlemm’s canal surgery. Curr Eye Res. 2020;45(10):1181–1187. doi:10.1080/02713683.2020.1773866
- Vold SD, Williamson BK, Hirsch L, et al. Canaloplasty and trabeculotomy with the OMNI system in pseudophakic patients with open-angle glaucoma: the ROMEO study. Ophthalmol Glaucoma. 2021;4(2):173–181. doi:10.1016/j.ogla.2020.10.001
- Hodapp EPR, Anderson D. Clinical Decisions in Glaucoma. Mosby Co, St Louis MO; 1993.
- Francis BA, Akil H, Bert BB. Ab interno Schlemm’s canal surgery. Dev Ophthalmol. 2017;59:127–146.
- Lewczuk K, Jablonska J, Konopinska J, Mariak Z, Rekas M. Schlemm’s canal: the outflow ‘vessel’. Acta Ophthalmol. 2022;100(4):e881–e890. doi:10.1111/aos.15027
- OMNI Surgical System. Menlo Park, CA: Sight Sciences, Inc; 2021.
- Gallardo MJ, Pyfer MF, Vold SD, et al. Canaloplasty and trabeculotomy combined with phacoemulsification for glaucoma: 12-month results of the GEMINI study. Clin Ophthalmol. 2022;16:1225–1234. doi:10.2147/OPTH.S362932
- Yadgarov A, Dentice K, Aljabi Q. Real-world outcomes of canaloplasty and trabeculotomy combined with cataract surgery in eyes with all stages of open-angle glaucoma. Clin Ophthalmol. 2023;17:2609–2617. doi:10.2147/OPTH.S422132
- Brown RH, Tsegaw S, Dhamdhere K, Lynch MG. Viscodilation of Schlemm canal and trabeculotomy combined with cataract surgery for reducing intraocular pressure in open-angle glaucoma. J Cataract Refract Surg. 2020;46(4):644–645. doi:10.1097/j.jcrs.0000000000000107
- Bleeker AR, Litchfield WR, Ibach MJ, Greenwood MD, Ristvedt D, Berdahl JP. Terveen DC Short-term efficacy of combined ab interno canaloplasty and trabeculotomy in pseudophakic eyes with open-angle glaucoma. Clin Ophthalmol. 2022;16:2295–2303. doi:10.2147/OPTH.S367896
- Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern. Ophthalmology. 2021;128:P71–P150.