
Abstract
Purpose
The present study evaluated the efficacy of suprachoroidal injection of Triamcinolone Acetonide (SCTA) in diabetic macular edema (DME) following pars plana vitrectomy (PPV) using a modified microneedle.
Patients and methods
A prospective interventional study was conducted on 60 eyes of 60 patients with centrally involved diabetic macular edema following pars plana vitrectomy (PPV). SCTA was performed at the baseline and repeated after 3 months in case of persistent subretinal or intraretinal fluid, central macular thickness (CMT) more than 300 µm or visual loss by more than one line of the Snellen chart.
Results
The present study detected significant reduction of the CMT from 498.3 ± 94.8 µm at the baseline to 212.3 ± 11.9 µm after 12 months of injection with p < 0.001 and a significant improvement of best corrected visual acuity (BCVA) from 1 (0.9–1.2) at the baseline to 0.5 (0.3–0.7) after 12 months of injection with p < 0.001. The intraocular pressure (IOP) increased significantly after 3 months of injection with p < 0.001 and then gradually declined to its normal level after 6 months. Inner segment/outer segment (IS/OS) disruption was the only significant predictor of the final CMT; however, the number of injections, IS/OS disruption, baseline BCVA and the HbA1C level were the significant predictors of the final BCVA after injection.
Conclusion
Suprachoroidal injection of TA using this microneedle resulted in significant anatomical and functional improvement in previously vitrectomized diabetic macular edema patients with no recorded ocular or systemic adverse events.
Introduction
Macular edema (ME) is defined as accumulation of intraretinal or subretinal fluid in the macular area that occurs on top of multiple retinal disorders including retinal vein occlusion (RVO), uveitis and diabetic retinopathy and is considered a leading cause of visual loss.Citation1–3 Pars plana vitrectomy (PPV) is a surgical procedure that deals with complications of proliferative diabetic retinopathy in the form of persistent premacular and vitreous hemorrhage, tractional retinal detachment and epimacular membranes.Citation4 PPV can improve retinal oxygenation and clear all inflammatory cytokines and vascular endothelial growth factor (VEGF) from the vitreous cavity with subsequent visual improvement.Citation5,Citation6 Macular edema following PPV is seen in about 15% of cases,Citation7 and the main mechanism of ME is alteration of Muller cell aquaporin channels induced by inflammation along with disruption of the tight junctions in the retinal pigment epithelium (RPE) with subsequent derangement of foveal water balance.Citation8
Nowadays, anti-VEGF agents and steroids are considered the mainstay in the treatment armamentarium of diabetic macular edema;Citation9,Citation10 however, with the lack of the vitreous in vitrectomized patients, the half life of anti-VEGF agents is markedly reduced if compared to steroids as a dexamethasone implant. This illustrates the superiority of steroids over anti- VEGF agents in treating diabetic macular edema in vitrectomized patients;Citation11,Citation12 however, ocular hypertension and secondary glaucoma remain the main adverse effects of intravitreal steroids.Citation13,Citation14
The suprachoroidal space (SCS) is a new drug delivery route to the posterior segment of the eye.Citation15,Citation16 Suprachoroidal injection of steroids achieved more than 10-fold higher concentration in the retina and choroid and a lower concentration in the anterior segment structures (lens, iris and ciliary body) if compared to intravitreal injection.Citation17 This limits the incidence of secondary glaucoma and cataract formation with a suprachoroidal route of injection.Citation18,Citation19 The suprachoroidal injection of steroids has been reported to achieve very good results in patients with noninfectious uveitis, retinal vein occlusion and diabetic macular edema.Citation19–22
The present study investigates the use of a minimally invasive modified custom microneedle for suprachoroidal injection of Triamcinolone Acetonide (SCTA) for diabetic macular edema following pars plana vitrectomy.
Methods
Study Design
A prospective interventional study was conducted on 60 eyes of 60 patients with centrally involved diabetic macular edema following pars plana vitrectomy (PPV) for diabetic vitreous hemorrhage and tractional retinal detachment. Cases were recruited from the Ophthalmology Department, Tanta University, Egypt in October 2022 and the results were obtained in October 2023. The study was performed as per 1964 Helsinki Declaration principles. Sample size was calculated using MedCalc program for Windows, version 14.8.1 aided by a previous study in which the mean BCVA (log MAR) before SCTA injection was 1.05 and the standard deviation was 0.41. Three months post injection, the mean BCVA (log MAR) was 0.73 and the standard deviation was 0.41.Citation23 Considering alpha error of 1% and beta error of 5%, the study required a total sample size of 60 patients.
Participants
Sixty eyes of 60 patients with centrally involved diabetic macular edema presented more than 6 months following PPV with central macular thickness (CMT) more than 300 µm detected by optical coherence tomography (OCT). All cases were pseudophakic. Assessment of glycated hemoglobin (HbA1C) level was done for all subjects at the baseline. All patients underwent careful ophthalmic examination including BCVA assessment by log MAR for statistical analysis purposes, intraocular pressure (IOP) measurement by applanation tonometry, examination of the anterior segment by slit lamp and posterior segment by slit lamp biomicroscopy using a +78 D lens and indirect ophthalmoscopy. Swept source optical coherence tomography (SW-OCT) with a vertical scan protocol centered on the fovea was performed for all patients at the baseline. Exclusion criteria included high myopic patients, candidates who received other DME treatment strategies such as laser treatment and intravitreal injection of anti-VEGF agents or steroids, patients with coexistent post-diabetic vitrectomy vitreous hemorrhage, post-diabetic vitrectomy epimacular membranes and other retinal diseases like retinal vascular occlusion, age-related macular degeneration (AMD), choroidal neovascular membrane (CNV), chorioretinitis, infectious and noninfectious posterior uveitis. Moreover, patients known to be glaucomatous or with IOP > 20 mmHg and patients with hazy ocular media that interfered with good OCT images were also excluded.
Surgical Technique
Suprachoroidal injection of Triamcinolone Acetonide (SCTA) was performed under complete aseptic technique in the operation room by a single experienced surgeon (AEN). Prior to injection, all patients received topical antibiotic eye drops (Gatifloxacin 0.3%, Tymer; Jamjoom, Egypt) 3 times daily for three days. Pupillary dilatation was done using topical Mydriacyl eye drops (Tropicamide 1%, Alcon). Anesthesia was performed (Benoxinate hydrochloride 0.4%, Benox; Epico, Egypt) 10 minutes before the procedure. Sterilization of the periocular area was done using 10% povidone iodine (Betadine) and sterilization of the eye was performed by instillation of 5% povidone iodine into the conjunctival cul de sac for 3 minutes and then the eye was draped and a lid speculum was applied. Regarding the customization of the microneedle, a 30 gauge 1 cc insulin syringe was introduced into the lumen of 24 gauge intravenous branula. In order to allow 1 mm of the insulin syringe to be exposed, the 24 gauge branula was cut and trimmed to act as a stopper to the 30 gauge needle (the final appearance of the custom microneedle is shown in ). In respect to the technique of suprachoroidal injection, 0.1 ml (4 mg) of Triamcinolone Acetonide (TA) (Kenacort A by GlaxoSmithKline, Brentford, UK) was injected in the inferotemporal quadrant 4 mm from the limbus with the bevel directed backwards. After introduction of the needle, injection was completed once no resistance was detected. Finally, rapid application of a cotton-tipped applicator before withdrawal of the needle to avoid drug reflux.Citation21,Citation22 Immediate fundus examination is essential to exclude central retinal artery occlusion, suprachoroidal hemorrhage and to detect unintended entry of TA into the vitreous cavity. Application of an eye patch for several hours was done after instillation of one drop of (Gatifloxacin 0.3%, Tymer; Jamjoom, Egypt). The patients were examined the next and the third day post injection to exclude adverse events like uveitis, endophthalmitis, ocular hypertension, vitreous hemorrhage and retinal detachment. Swept source optical coherence tomography (SW-OCT) with vertical scan protocol centered on the fovea was performed for all patients after 1, 3, 6, 9 and 12 months. Reinjection was performed after 3 months in case of one or more of the following: persistent subretinal or intraretinal fluid, CMT more than 300 µm or visual loss by more than one line of the Snellen chart.
Figure 1 The final appearance of the custom microneedle.

Statistical Analysis
Categorical variables were expressed as number and percentage, while mean and standard deviation were used to express normally distributed data. Central macular thickness (CMT), BCVA (log MAR) and IOP changes at the baseline and 1, 3, 6, 9 and 12 months were compared using repeated measure ANOVA test. Correlation between the final CMT (µm), final BCVA (log MAR) and other variables were evaluated using correlation coefficient. Multivariable linear regression analysis was used to detect the independent predictors of the final CMT (µm) and the final BCVA (log MAR). Factors entered in regression analysis for the final CMT (µm) included sex, inner segment/outer segment (IS/OS) disruption, baseline CMT (µm), baseline BCVA (log MAR) and number of injections. While age, HbA1C, IS/OS disruption, baseline CMT (µm), baseline BCVA (log MAR) and number of injections were the factors entered in the regression analysis of the final BCVA (log MAR). Final BCVA (log MAR) entered into regression analysis was transformed into normal using a two-step approach for transforming continuous variables to normal.Citation24 Categorical variables were entered in the model as dummy variables. They are coded as: 0 for absent (IS/OS) disruption and 1 for the presence of IS/OS disruption. p ≤ 0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., 2017).
Results
Sixty eyes of 60 patients were included in the present study. The mean HbA1C level in the studied patients was 8.01 ± 1.04%. Inner segment/outer segment (IS/OS) disruption was detected in 30 patients by OCT. Throughout the period of the study, 20 patients received a single injection, 27 patients received 2 injections while the remaining 13 patients received 3 injections. These clinical and socio-demographic data are presented in .
Table 1 Sociodemographic and Clinical Characters of the Studied Patients
The present study detected significant reduction of the CMT from 498.3 ± 94.8 µm at the baseline to 212.3 ± 11.9 µm after 12 months of injection with p < 0.001 (). Regarding BCVA, the present study detected significant improvement of BCVA (log MAR) from 1 (0.9–1.2) at the baseline to 0.5 (0.3–0.7) after 12 months of injection with p < 0.001 (). The IOP increased significantly after 3 months of injection with p < 0.001 and then gradually declined to its normal level after 6 months of injection and remained stable until the end of the study (). These results are illustrated in .
Figure 2 Changes in CMT at the baseline and after 1, 3, 6, 9 and 12 months.
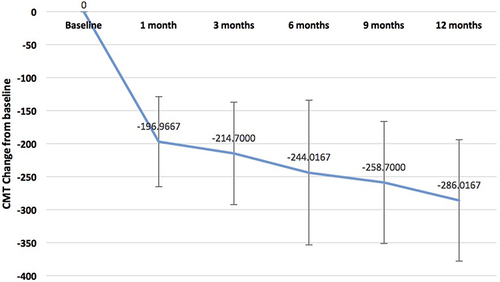
Figure 3 Changes in BCVA at the baseline and after 1, 3, 6, 9 and 12 months.
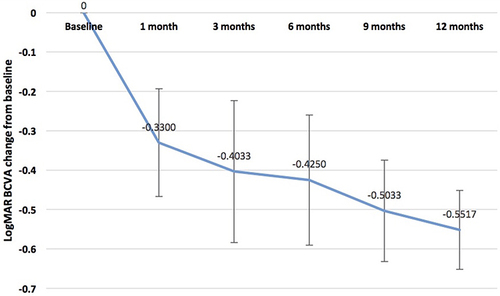
Figure 4 Changes in IOP at the baseline and after 1, 3, 6, 9 and 12 months.
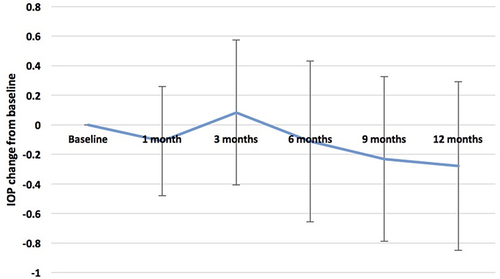
Table 2 Changes in CMT (µm), BCVA (Log MAR) and IOP (mmHg) at the Baseline and 1, 3, 6, 9 and 12 Months
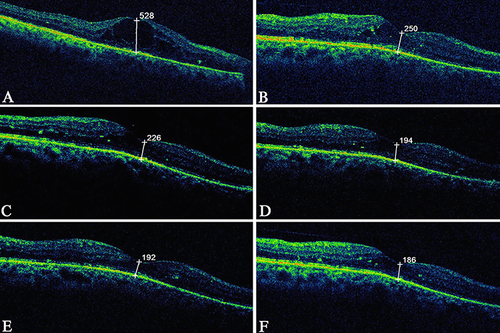
Reduction of the central macular thickness with improvement of the BCVA following single SCTA is illustrated in which shows the OCT of a male patient aged 51 years presented with diabetic macular edema after left PPV for diabetic vitreous hemorrhage since 8 months.
Figure 5 OCT of a male patient aged 51 years with history of left PPV for diabetic vitreous hemorrhage since 8 months, the patient received single SCTA: (A) OCT at the baseline showing cystoid macular edema with IS/OS disruption, the CMT is 528 µm, the BCVA (log MAR) is 1.1; (B) OCT after 1 month, the CMT is 250 µm; (C) OCT after 3 months, the CMT is 226 µm; (D) OCT after 6 months, the CMT is 194µm; (E) OCT after 9 months, the CMT is 192 µm; (F) OCT after 12 months, the CMT is 186 µm, the BCVA (log MAR) improved to 0.4.
presents significant positive correlation between the number of injections, baseline CMT (µm), baseline BCVA (log MAR) and IS/OS disruption with the final CMT (µm) with p values (0.02, 0.02. 0.04 and 0.02) respectively denoting that an increased number of injections, higher baseline CMT, worse baseline BCVA and the presence of IS/OS disruption were associated with worse final CMT. In addition, significant positive correlation was reported between age, HbA1C level, number of injections, baseline CMT (µm), baseline BCVA (log MAR) and IS/OS disruption with the final BCVA (log MAR) with p <0.001; this reflected that more advanced age, higher levels of HbA1C, increased frequency of injections, worse baseline CMT, worse baseline BCVA together with the presence of IS/OS disruption were associated with worse final BCVA.
Table 3 Correlation Between Sociodemographic and Clinical Variables with the Final CMT (µm) and the Final BCVA (Log MAR)
highlights the predictors of the final CMT and the final BCVA after injection, it was reported that the presence of IS/OS disruption was the only significant predictor of the final CMT with p value of 0.009; however, the number of injections, the presence of IS/OS disruption, baseline BCVA and the HbA1C level were significant predictors of the final BCVA after injection with p values of 0.02, <0.001, <0.001 and <0.001 respectively.
Table 4 Multivariable Linear Regression Analysis of Independent Predictors of the Final CMT (µm) and the Final BCVA (Log MAR)
No cases of uveitis, endophthalmitis, suprachoroidal hemorrhage, vitreous hemorrhage, retinal break or retinal detachment were reported throughout the study period.
Discussion
Suprachoroidal (SC) space is a new drug delivery method that allows the drug to reach the retina and the choroid with limited anterior segment concentration and many studies have reported circumferential flow of the drug to the posterior pole after suprachoroidal injection.Citation25–27 This raised the interest of the researchers to use SCTA for the treatment of many retinal diseases.Citation19–22,Citation28 Different forms of microneedles were modified in length for safe and effective delivery of TA to the suprachoroidal space. The present study assessed the efficacy of SCTA in treating diabetic macular edema following pars plana vitrectomy using a cheap modified hand-made microneedle. Similarly, previous studies applied the same microneedle for SCTA in branch retinal vein occlusion and diabetic macular edema patients.Citation21,Citation22 Moreover, Oli and Waikar manufactured a similar microneedle for SCTA in pseudophakic cystoid macular edema patients using a 26 G needle and sleeve of intracath.Citation29
The rationale of using steroids in treating diabetic macular edema in vitrectomized patients is well established. Boyer et al detected significant visual gain following dexamethasone implant in post-PPV diabetic macular edema cases,Citation12 but the high cost was the main disadvantage of this implant in low-income countries, besides due to the absence of the vitreous, retinal injury may occur due to the high speed of the dexamethasone implant during injection.Citation30
The present study detected significant reduction of the CMT with significant improvement of the BCVA after 12 months of SCTA with an acceptable safety profile. This is quite similar to a previous study that applied single SCTA on 11 eyes of 10 vitrectomized patients presenting with diabetic macular edema, where the BCVA (log MAR) improved from 0.75 at the baseline to 0.4 after treatment and the CMT was reduced from 456.45 ± 113.42 µm at baseline to 247.63 ± 53.40 µm following injection. No cases of ocular hypertension were reported during 8 weeks of follow up.Citation31
Multiple studies evaluated the efficacy of SCTA in nonvitrectomized diabetic macular edema patients refractory to previous anti-VEGF agents. Nawar detected significant decline of the CMT from 478.7 ± 170.2 µm to 230.2 ± 47.4 µm after SCTA with significant visual improvement from 1.193 ± 0.2 to 0.76 ± 0.3 after 12 months of SCTA. The IOP rose significantly after 1 month and then declined to its normal value at the third month which is different from the current study in which IOP reached its maximum value 3 months after SCTA and then returned to its normal value after 6 months.Citation22
The present study confirmed the safety of SCTA regarding IOP; this is coincident with a previous study that compared the efficacy of SCTA with intravitreal injection of TA (IVTA) in patients with resistant diabetic macular edema on top of epiretinal membrane, and it was documented that both SCTA and IVTA detected no significant differences regarding reduction of the CMT and BCVA improvement, but IVTA achieved greater macular edema recurrence rate and more rise in IOP compared to SCTA.Citation32 Furthermore, Özdemir et al studied the effectiveness of dexamethasone implant in 17 eyes of 17 patients with diabetic macular edema after PPV for tractional retinal detachment; the mean BCVA (log MAR) was significantly improved from 0.77 before injection to 0.64, 0.68 and 0.66 after 1, 3 and 6 months respectively with significant decline of the CMT from 452 µm prior to injection to 310, 368 ± 34 and 375 µm after 1, 3 and 6 months respectively. Regarding IOP, it was elevated significantly from 16 ± 1.2 mmHg before injection to 18.2, 18.8 and 18.5 mmHg after 1, 3, and 6 months respectively. In addition, 2 eyes showed marked IOP elevation (IOP ≥ 25 mmHg) that required topical anti-glaucoma medication, and this illustrates the safety of SCTA over dexamethasone implant regarding IOP.Citation33
In our cohort, 20eyes needed single SCTA and 27 eyes needed two SCTA during the 12 months of follow up. This emphasizes the long-term efficacy of SCTA, and is in the same line with other studies which stated that the efficacy of SCTA can persist up to 6 months.Citation22,Citation29,Citation33
The present study detected significant positive correlation between HbA1C level and the final BCVA (log MAR) denoting worse final BCVA with higher baseline HbA1C level, and this correlation lies in the same line with a previous study that reported poorer response to intravitreal injection of ziv-aflibercept in patients with diabetic macular edema with poorer glycemic control.Citation34 In addition, our cohort reported significant positive correlation between the baseline CMT and the final BCVA (log MAR), and this agrees with multiple previous studies that confirmed that the reduction of the retinal thickness can improve retinal function.Citation35–39 Besides, in another study, BCVA improvement by ≥10 letters was associated with decrease in CMT by ≥20%; however, decline in CMT by <20% resulted in limited visual gain.Citation40
According to the current study, the integrity of the IS/OS segment is a strong predictor of the final CMT and the final BCVA; this may be explained by the fact that chronic macular edema is usually associated with macular ischemia with subsequent photoreceptor damage,Citation41 and is quite similar to Barthelmes et al who detected that IS/OS segment and external limiting membrane (ELM) integrity are the third important factor in predicting the functional outcomes after 3 monthly conbercept injections;Citation42 moreover, other studies postulated that switching to steroids can improve IS/OS disruption and disorganization of the outer retinal layers and hence improves vision.Citation43,Citation44 Furthermore, the present study reported that worse baseline BCVA was associated with worse final BCVA, and this agrees with previous studies that revealed that the baseline BCVA was a strong predictor of the final BCVA.Citation45–47
The main limitations of this study include the small sample size, short follow-up duration, along with lack of comparison with intravitreal injection of anti-VEGF agents and steroids. Hence, a larger cohort with longer follow-up period and comparison with other agents and routes of injection are needed to validate our findings.
Conclusions
Suprachoroidal injection of TA using this custom hand-made microneedle resulted in significant anatomical and functional improvement in previously vitrectomized diabetic macular edema patients with no recorded ocular or systemic adverse events. Inner segment/outer segment (IS/OS) disruption was the only significant predictor of the final CMT; however, the number of injections, IS/OS disruption, baseline BCVA and HbA1C level were significant predictors of the final BCVA.
Ethical Approval and Consent to Participate
The study was approved by the Institutional review board of the Faculty of Medicine, Tanta University, Egypt (approval code 35625/8/22). All procedures were performed under 1964 Helsinki Declaration rules. Written informed consent was obtained from all participants of the study.
Disclosure
The authors have no financial or nonfinancial interests to disclose for this work.
Acknowledgments
The authors would like to show their great gratitude to all staff members of Ophthalmology Department, Tanta University, Egypt for their great advice and support.
Data Sharing Statement
Clinical data and figures of all participants are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Sarao V, Veritti D, Boscia F, Lanzetta P. Intravitreal steroids for the treatment of retinal diseases. Sci World J. 2014;2014:1–14. doi:10.1155/2014/989501
- Daruich A, Matet A, Moulin A, et al.. Mechanisms of macular edema: beyond the surface. Prog Retin Eye. research. 2018;63:20–68. doi:10.1016/j.preteyeres.2017.10.006
- Sacconi R, Giuffrè C, Corbelli E, Borrelli E, Querques G, Bandello F. Emerging therapies in the management of macular edema: a review. F1000Res. 2019;12(8):F1000 Faculty Rev–1413. doi:10.12688/f1000research.19198.1
- Gupta V, Arevalo JF. Surgical management of diabetic retinopathy. Middle East Afr J Ophthalmol. 2013;20(4):283. doi:10.4103/0974-9233.120003
- Todorich B, Mahmoud TH. Vitrectomy for diabetic macular edema. Curr Ophthalmol Rep. 2014;2:167–174. doi:10.1007/s40135-014-0052-6
- White NH, Sun W, Cleary PA, Tamborlane WV, Danis RP, Dp& H. DCCT-EDIC Research Group. Effect of prior intensive therapy in type 1 diabetes on 10-year progression of retinopathy in the DCCT/EDIC: comparison of adults and adolescents. Diabetes. 2010;59(5):1244–1253. doi:10.2337/db09-1216
- Frisina R, Pinackatt SJ, Sartore M, et al. Cystoid macular edema after pars plana vitrectomy for idiopathic epiretinal membrane. Graefes Arch Clin Exp Ophthalmol. 2015;253:47–56. doi:10.1007/s00417-014-2655-x
- de Smet MD. Insights into the physiopathology of inflammatory macular edema. Dev Ophthalmol. 2017;58:168–177. doi:10.1159/000455279
- Heier JS, Korobelnik JF, Brown DM, et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the Vista and VIVID studies. Ophthalmology. 2016;123(11):2376–2385. doi:10.1016/j.ophtha.2016.07.032
- Crim N, Velez-Montoya R, Morales-Canton V. Surgical Versus Medical Treatment for Diabetic Macular Edema: a Review. Med Hypothesis Discov Innov Ophthalmol. 2017;6(4):136–142. PMID: 29560368; PMCID: PMC5847309.
- Yanyali A, Aytug B, Horozoglu F, Nohutcu AF. Bevacizumab (Avastin) for diabetic macular edema in previously vitrectomized eyes. A J. ophthalmology. 2007;144(1):124–126. doi:10.1016/j.ajo.2007.02.048
- Boyer DS, Faber D, Gupta S, Patel SS, Tabandeh H, Ozurdex CHAMPLAIN Study Group LXY&. Dexamethasone intravitreal implant for treatment of diabetic macular edema in vitrectomized patients. Retina. 2011;31(5):915–923. doi:10.1097/IAE.0b013e318206d18c
- Comyn O, Lightman SL, Hykin PG. Corticosteroid intravitreal implants vs. ranibizumab for the treatment of vitreoretinal disease. Curr Opin Ophthalmol. 2013;24(3):248–254. doi:10.1097/ICU.0b013e32835fab27
- Arcinue CA, Ceron OM, Foster CS. A comparison between the fluocinolone acetonide (retisert) and dexamethasone (ozurdex) intravitreal implants in uveitis. J Ocul Pharmacol Ther. 2013;29(5):501–507. doi:10.1089/jop.2012.0180
- Naftali Ben Haim L, Moisseiev E. Drug delivery via the suprachoroidal space for the treatment of retinal diseases. Pharmaceutics. 2021;13(7):967. doi:10.3390/pharmaceutics13070967
- Hartman RR, Kompella UB. Intravitreal, subretinal, and suprachoroidal injections: evolution of microneedles for drug delivery. J Ocul Pharmacol Ther. 2018;34(1–2):141–153. doi:10.1089/jop.2017.0121
- Patel SR, Berezovsky DE, McCarey BE, Zarnitsyn V, Edelhauser HF, Prausnitz MR. Targeted administration into the suprachoroidal space using a microneedle for drug delivery to the posterior segment of the eye. Invest Ophthalmol Vis Sci. 2012;53(8):4433–4441. doi:10.1167/iovs.12-9872
- Hancock SE, Wan CR, Fisher NE, Andino RV, Ciulla TA. Biomechanics of suprachoroidal drug delivery: from benchtop to clinical investigation in ocular therapies. Expert Opin Drug Deliv. 2021;18(6):777–788. doi:10.1080/17425247.2021.1867532
- Goldstein DA, Do D, Noronha G, Kissner JM, Srivastava SK, Nguyen QD. Suprachoroidal corticosteroid administration: a novel route for local treatment of noninfectious uveitis. Transl Vis Sci Technol. 2016;5(6):14. doi:10.1167/tvst.5.6.14
- Campochiaro PA, Wykoff CC, Brown DM, et al. Suprachoroidal triamcinolone acetonide for retinal vein occlusion: results of the tanzanite study. Ophthalmol Retina. 2018;2(4):320–328. doi:10.1016/j.oret.2017.07.013
- Nawar AE. Modified microneedle for suprachoroidal injection of triamcinolone acetonide combined with intravitreal injection of ranibizumab in branch retinal vein occlusion patients. Clin Ophthalmol. 2022;1139–1151. doi:10.2147/OPTH.S361636
- Nawar AE. Effectiveness of suprachoroidal injection of triamcinolone acetonide in resistant diabetic macular edema using a modified microneedle. Clin Ophthalmol. 2022;3821–3831. doi:10.2147/OPTH.S391319
- Zhang DD, Che DY, Zhu DQ. A simple technique for suprachoroidal space injection of triamcinolone acetonide in treatment of macular edema. Int J Ophthalmol. 2022;15(12):2017. doi:10.18240/ijo.2022.12.18
- Templeton GF. A two-step approach for transforming continuous variables to normal: implications and recommendations for IS research. Commun Assoc Inf Syst. 2011;28(1):4. doi:10.17705/1CAIS.02804
- Chiang B, Jung JH, Prausnitz MR. The suprachoroidal space as a route of administration to the posterior segment of the eye. Adv Drug Deliv Rev. 2018;126:58–66. doi:10.1016/j.addr.2018.03.001
- Habot-Wilner Z, Noronha G, Wykoff CC. Suprachoroidally injected pharmacological agents for the treatment of chorio-retinal diseases: a targeted approach. Acta Ophthalmol. 2019;97(5):460–472. doi:10.1111/aos.14042
- Abarca BC, EM SJH, Patel S, Patel S. Treatment of acute posterior uveitis in a porcine model by injection of triamcinolone acetonide into the suprachoroidal space using microneedles. Invest Ophthalmol Vis Sci. 2013;54(4):2483–2492. doi:10.1167/iovs.13-11747
- Price KW, Albini TA, Yeh S. Suprachoroidal injection of triamcinolone- Review of a novel treatment for macular edema caused by noninfectious uveitis. US Ophthalmic Rev. 2020;13(2):76–79. doi:10.17925/usor.2020.13.2.76
- Oli A, Waikar S. Modified inexpensive needle for suprachoroidal triamcinolone acetonide injections in pseudophakic cystoid macular edema. Indian J Ophthalmol. 2021;69(3):765. doi:10.4103/ijo.IJO_1464_20
- Jung SM, JW PSW, Lee JE, Byon IS, Byon IS. Retinal injury following intravitreal injection of a dexamethasone implant in a vitrectomized eye. Int J Ophthalmol. 2017;10(6):1019–1020. doi:10.18240/ijo.2017.06.31
- Marashi A, Zazo A. Suprachoroidal injection of triamcinolone acetonide using a custom-made needle to treat diabetic macular edema post pars plana vitrectomy: a case series. J Int Med Res. 2022;50(4). doi:10.1177/03000605221089807
- Abdelshafy Tabl A, Tawfik Soliman T, Anany Elsayed M, Abdelshafy Tabl M, Meduri A. A randomized trial comparing suprachoroidal and intravitreal injection of triamcinolone acetonide in refractory diabetic macular edema due to epiretinal membrane. J Ophthalmol. 2022. doi:10.1155/2022/7947710
- Özdemir HB, Hasanreisoğlu M, Yüksel M, Ertop M, Gürelik G, Özdek Ş. Effectiveness of intravitreal dexamethasone implant treatment for diabetic macular edema in vitrectomized eyes. Turk J Ophthalmol. 2019;49(6):323. doi:10.4274/tjo.galenos.2019.95226
- Nawar AE, Wasfy T, Shafik HM. Switching to ziv-aflibercept in resistant diabetic macular edema non responsive to ranibizumab injection. BMC Ophthalmol. 2022;22(1):1–10. doi:10.1186/s12886-022-02503-x
- Mastropasqua R, Toto L, Borrelli E, et al. Morphology and function over a one-year follow up period after intravitreal dexamethasone implant (Ozurdex) in patients with diabetic macular edema. PLoS One. 2015;10(12):e0145663. doi:10.1371/journal.pone.0145663
- Karttunen T, Nummelin L, Kaarniranta K, Kinnunen K. Real life experience of dexamethasone implant in refractory diabetic macular oedema. Clin Ophthalmol. 2019;13:2583–2590. doi:10.2147/OPTH.S232549
- Cao J, You K, Jin K, et al. Prediction of response to anti-vascular endothelial growth factor treatment in diabetic macular oedema using an optical coherence tomography-based machine learning method. Acta Ophthalmol. 2020;99(1):e19–e27. doi:10.1111/aos.14514
- Meduri A, Oliverio GW, Trombetta L, Giordano M, Inferrera L, Trombetta CJ. Optical coherence tomography predictors of favorable functional response in naïve diabetic macular edema eyes treated with dexamethasone implants as a first-line agent. J Ophthalmol. 2021;2021:1–5. doi:10.1155/2021/6639418
- Wu L, Chawan-Saad J, Wu M, Wu A. Corticosteroids for diabetic macular edema. Taiwan J Ophthalmol. 2019;9(4):233–242. doi:10.4103/tjo.tjo_68_19
- Early Treatment Diabetic Retinopathy Study Research Group Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early treatment diabetic retinopathy study report number 2. Ophthalmology. 1987;94(7):761–774. doi:10.1016/S0161-6420(87)33527-4.
- Hatz K, Ebneter A, Tuerksever C, Pruente C, Zinkernagel M. Repeated dexamethasone intravitreal implant for the treatment of diabetic macular oedema unresponsive to anti-VEGF Therapy: Outcome and Predictive SD-OCT Features. Ophthalmologica. 2018;239(4):205–214. doi:10.1159/000485852
- Barthelmes D, Sutter FK, Gillies MC. Differential optical densities of intraretinal spaces. Investig Ophthalmol Vis Sci. 2008;49(8):3529–3534. doi:10.1167/iovs.07-1320
- Muftuoglu IK, Mendoza N, Gaber R, Alam M, You QS, Freeman WR. Integrity of outer retinal layers after resolution of central involved diabetic macular edema. Retina. 2017;37(11):2015–2024. doi:10.1097/IAE.0000000000001459
- Rangaraju L, Jiang X, McAnany JJ, et al. Association between visual acuity and retinal layer metrics in diabetics with and without macular edema. J Ophthalmol. 2018;2018:1–8. doi:10.1155/2018/1089043
- Channa R, Sophie R, Khwaja AA, et al. Factors affecting visual outcomes in patients with diabetic macular edema treated with ranibizumab. Eye (Lond). 2014;28(3):269–278. doi:10.1038/eye.2013.245
- Eski Yucel O, Birinci H, Sullu Y. Outcome and predictors for 2-year visual acuity in eyes with diabetic macular edema treated with Ranibizumab. J Ocul Pharmacol Ther. 2019;35(4):229–234. doi:10.1089/jop.2018.0082
- Sophie R, Lu N, Campochiaro PA. Predictors of functional and anatomic outcomes in patients with diabetic macular edema treated with Ranibizumab. Ophthalmology. 2015;122(7):1395–1401. doi:10.1016/j.ophtha.2015.02.036