Abstract
We report a case of successive bilateral retinal vein occlusion in a human immunodeficiency virus (HIV)-positive male with multicentric Castleman’s disease treated successfully with a single injection of intravitreal bevacizumab. Castleman’s disease should be a differential diagnosis of occlusive retinovascular disease and, occasionally, ocular manifestation can lead to systemic diagnosis.
Introduction
Castleman’s disease is a rare lymphoproliferative disease characterized by massive growth of lymphoid tissue, with follicular hyperplasia, vascular proliferation, and plasmacytosis. The gold standard for diagnosis is lymph node biopsy.Citation1 Three distinct histologic subtypes include the hyaline vascular type (usually unicentric and mild), the plasma cell type (often multicentric and aggressive), and the mixed-type. It can be confined to one site or can be multicentric associated with systemic symptomatology. Patients with multicentric Castleman’s disease (MCD) present with multiple lesions, potentially affecting all organs, lymph nodes, liver, and spleen accompanied by constitutional symptoms and hematologic abnormalities. Multicentric Castleman’s disease is the rarest form of disease at all ages but is the most frequent form present in the setting of human immunodeficiency virus (HIV) seropositivity. We herein report a case of retinal vein occlusion during flare of MCD complicated by macular edema that completely resolved after a single intravitreal injection of anti-angiogenic agent.
Case report
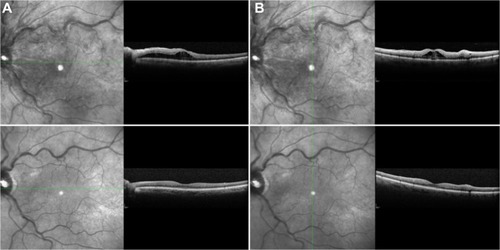
A 63-year-old active male cyclist with HIV (CD4 377/viral load <48 copies/mL) presented with blurred vision and light sensitivity in his left eye for several days while experiencing a flare of MCD disease with fever, tender lymphadenopathy, and profound fatigue. The patient had a history of right eye central retinal vein occlusion with vitreous hemorrhage resulting in significant permanent vision loss 4 years previously. Near that time he initially developed recurrent fevers, he also had cytopenias, hepatosplenomegaly, and tender lymphadenopathy that eventually led to diagnosis of MCD confirmed by lymph node biopsy. The patient declined recommended therapy with rituximab due to share of cost and prolonged remissions between flares. Initiation of valganciclovir 1-year ago resulted in attenuation and reduced frequency of MCD flares. On examination, his visual acuity was 20/200 in the right eye and 20/100 in the left eye. Intraocular pressure in both eyes and blood pressure were normal. Retinal examination in the right eye showed macular atrophy and laser burns after panretinal photocoagulation. The fundus exam of the left eye revealed optic nerve swelling, tortuous veins, cotton-wool spots, and intraretinal hemorrhages, a few of which were white-centered Roth spots (white arrows on ). Fluorescein angiography and spectral-domain optical coherence tomography (SD-OCT) showed delayed perfusion times and macular edema in the left eye, respectively. SD-OCT showed subretinal fluid extending from the optic disc to the fovea (). Hypercoagulability workup demonstrated only mildly increased anti-cardiolipin antibody; there was no evidence of a lupus anticoagulant, prothrombin, or factor V Leiden mutation and the patient had normal antithrombin, protein C, and S. His left eye was treated with intravitreal injection of bevacizumab 1.25 mg in 0.05 mL. After a single injection there was a rapid improvement in visual acuity in his eye. At the last visit 6 months after treatment his visual acuity remained at 20/20 with normal retinal findings (). He also initially received the recommended systemic therapy with rituximab followed by high dose zidovudine with valganciclovir; this resulted in the longest remission to date of systemic MCD flare (>12 months to date).
Figure 1 Color fundus photograph of the left eye of the patient with flare of multicentric Castleman’s disease.
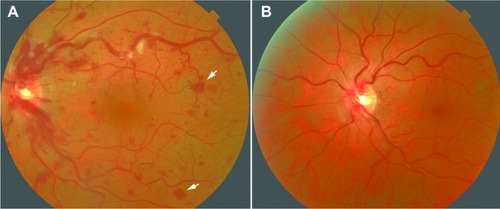
Figure 2 Horizontal (A) and vertical (B) scans of eye at presentation showing subretinal fluid extending from the optic disc to the fovea. Corresponding follow-up scans (lower panels) 5 months after treatment showing complete resolution of subretinal fluid.
Discussion
MCD affects primarily neck, thoracic, and retroperitoneal lymph nodes. Ophthalmic complications in MCD are very rare with most published cases describing intraorbital and optic nerve lesions.Citation2,Citation3 Intraocular involvement is rarer with one published adult case of uveitis,Citation4 two cases of bilateral,Citation5,Citation6 one case of unilateral serous retinal detachment and choroidal effusion,Citation7 one case of hypertensive choroidopathy,Citation8 one case of choroidal infiltrates,Citation7 and one case of optic nerve drusen and peripapillary choroidal neovascularization in a patient with peripheral neuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, skin changes (POEMS) syndrome and associated Castleman’s disease.Citation9 One pediatric case describing venous engorgement and tortuosity, intraretinal hemorrhages, cotton wool spots, and neurosensory detachment of the posterior pole was thought to be due to hyperviscosity syndrome which responded to one session of plasmapheresis.Citation10 Herein, we report a case of an incomplete vein occlusion in an HIV+ adult patient. Central retinal vein occlusion in the other eye triggered medical evaluation leading to diagnosis of MCD. Patients with HIV infection have been reported to have a small risk of retinal vascular occlusionCitation11 but because the occlusion occurred in both eyes during flares of lymphoproliferative disease we attribute this event to MCD. A single injection of an anti-angiogenic agent was sufficient for resolution of subretinal fluid and improvement in vision. Finding Roth spots in the retina in MCD is also unique and to our knowledge not previously reported.
After an automated search in PubMed, this appears to be the first case of successive bilateral retinal vein occlusion in an HIV+ male with MCD treated successfully with a single injection of intravitreal bevacizumab. Castleman’s disease should be on differential diagnosis of occlusive retinovascular disease and, occasionally, ocular manifestation can lead to systemic diagnosis.
Disclosure
The authors report no conflicts of interest in this work.
References
- CastlemanBIversonLMenendezVPLocalized mediastinal lymphnode hyperplasia resembling thymomaCancer19569482283013356266
- KurokawaTSuzukiSKawaguchiKFujisawaNYoshimuraNCastleman disease presenting with ophthalmic signs and symptomsAm J Ophthalmol1999128111411610482111
- InataniMKashiiSNosakaKArimaNOrbital pseudotumor as an initial manifestation of multicentric Castleman’s diseaseJpn J Ophthalmol200549650550816365797
- OshitariTKajitaFTobeARefractory uveitis in patient with castleman disease successfully treated with tocilizumabCase Rep Ophthalmol Med2012201296818023198204
- ParkSHSongSJCastleman’s disease presenting with uveal effusion syndromeKorean J Ophthalmol201024318218520532148
- BarileGRKhatibNLeeSEDhrami-GavaziEIranmaneshRStokesMBExudative retinal detachment in Castleman diseaseRetina Cases and Brief Reports200932200203
- EmersonGGLimLLoriauxMMulticentric Castleman disease associated with ocular involvement. A clinicopathologic case reportRetina Cases and Brief Reports200932197199
- LiuDTShieldsJALiCLNgHKLamDSHypertensive choroidopathy in Castleman’s diseaseGraefes Arch Clin Exp Ophthalmol2011249121901190321678090
- DiduszynJMQuillenDACantoreWAGardnerTWOptic disk drusen, peripapillary choroidal neovascularization, and POEMS syndromeAm J Ophthalmol2002133227527611812439
- JorgeRScottIUOliveiraRCCostaRASiqueiraRCLouzada-JúniorPOcular findings in a patient with Castleman’s disease before and after treatment with immunosuppression and plasmapheresisOphthalmic Surg Lasers Imaging201041 Online
- DunnJPYamashitaAKempenJHJabsDARetinal vascular occlusion in patients infected with human immunodeficiency virusRetina (Philadelphia, Pa)2005256759766