
Abstract
Background
Epiphora is a common complaint of nasolacrimal duct obstruction (NLDO) in adults. The precise pathogenesis of NLDO is still unknown, but inflammatory processes are believed to be predisposing factors. Endoscopic dacryocystorhinostomy (EN-DCR) is an effective surgical technique for treating symptomatic NLDO. The purpose of the procedure is to relieve the patient’s symptoms by creating an opening, ie, a rhinostoma, between the lacrimal sac and the nasal cavity. Although the success rates after EN-DCR are high, the procedure sometimes fails due to onset of a fibrotic process at the rhinostomy site. The aim of this prospective comparative study was to investigate inflammation-related gene expression in the nasal mucosa at the rhinostomy site.
Methods
Ten participants were consecutively recruited from eligible adult patients who underwent primary powered EN-DCR (five patients) or septoplasty (five controls). Nasal mucosa specimens were taken from the rhinostomy site at the beginning of surgery for analysis of gene expression. Specimens were taken from the same site on the lateral nasal wall for controls. Quantitative reverse transcription polymerase chain reaction (qRT-PCR) was performed for the inflammatory genes interleukin (IL)-6, IL-1β, and CCL2, and because of a clear trend of increased inflammation in the EN-DCR samples, a wider PCR array was performed to compare inflammation-related gene expression in EN-DCR subjects and corresponding controls.
Results
Our qRT-PCR results revealed a clear trend of increased transcription of IL-6, IL-1β, and CCL2 (P=0.03). The same trend was also evident in the PCR array, which additionally revealed notable differences between EN-DCR subjects and controls with regard to expression of several other inflammation-related mediators. At 6-month follow-up, the success rate after primary EN-DCR was 60%, ie, in three of five patients.
Conclusion
The present study demonstrates that there is an intense inflammation gene expression response in the nasal mucosa of patients undergoing EN-DCR.
Introduction
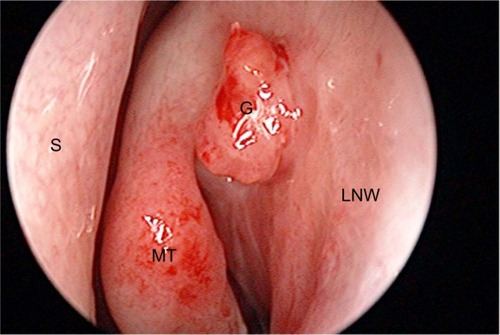
Epiphora, ie, tearing of the eye, is a common complaint, particularly in the elderly, the extent of which can vary from minor inconvenience to significant social embarrassment. The common cause of epiphora and discharge from the eye in adults is nasolacrimal duct obstruction (NLDO). The pathogenesis of NLDO is unknown, but the process is characterized by gradual inflammation and subsequent fibrosis of the nasolacrimal duct, which may lead to obstruction of the lacrimal pathway.Citation1,Citation2 Endoscopic dacryocystorhinostomy (EN-DCR) is an effective and safe surgical technique for treating symptomatic lower lacrimal pathway obstruction and dacryocystitis in cases where there is no response to conservative treatment. The purpose of the procedure is to create a bypass, ie, a rhinostoma, between the lacrimal sac and the nasal cavity. The success of primary EN-DCR has been reported to be high, varying between 74% and 94%.Citation3 However, the procedure sometimes fails, and the most common reason for this is scarring of the rhinostoma.Citation4,Citation5 The granulation tissue and scar formation is thought to be linked to the biology of wound healing in the nasal mucosa ().Citation6 There have been several histopathological studies reporting chronic inflammation and fibrosis in specimens taken from the nasal mucosa during dacryocystorhinostomy,Citation7–Citation9 and various histopathological features related to chronic inflammation may also play a role in the outcome of EN-DCR.Citation9,Citation10 However, inflammatory signaling molecules in the nasal mucosa of patients with NLDO have been poorly investigated. Smirnov et al demonstrated that high expression of heat shock protein 47, a regulator of fibrosis, might predict a poor surgical result after EN-DCR.Citation11 Further, these biological factors are important when investigating potential targets for development of antifibrotic therapy. This is of importance, given that there are no effective antifibrotic drugs available to target fibrogenic factors or to block their receptors.Citation12 The aim of this prospective comparative study was to investigate the inflammatory gene expression profile at the rhinostomy site in patients undergoing EN-DCR.
Figure 1 Excessive granulation formation over the hinostomy site.
Patients and methods
Patients
Five study subjects were consecutively recruited from adult patients who underwent primary EN-DCR due to epiphora or recurrent infection of the lacrimal sac between May and August 2012. Five control subjects were also recruited from eligible patients who underwent septoplasty during the same time period. Patients undergoing septoplasty were selected as controls because their indication for surgery was a septal deformity not associated with any inflammatory or infectious process. All the operations were performed in the Department of Otorhinolaryngology at Kuopio University Hospital, in Kuopio, Finland. Patients were eligible for enrollment if they were adults (age >18 years) and if their American Society of Anesthesiologists physical status score was I–III.Citation13 Exclusion criteria were presacral obstruction, malignancy in the paranasal sinuses, nasal cavity, or lacrimal pathway, mental disability, pregnancy, or breast-feeding. Patients who underwent septoplasty were not eligible for participation as controls when there was a risk of postoperative adhesions due to the presence of a narrow nasal cavity or where there was a history of recurrent or chronic paranasal infections. The patient demographics are shown in . There were no dropouts during the 6-month follow-up period. This study was approved by the research ethics committee at the District Hospital of Northern Savo, Kuopio, Finland. The patients were given oral and written information about the trial protocol, and all provided their written consent.
Table 1 Baseline demographics of the study population, with data shown as the mean (standard deviation) or number of cases
Assessments
At the preoperative visit and 1-week, 2-month, and 6-month postoperative visits, an objective assessment was performed by an otorhinolaryngologist who performed lacrimal irrigation and nasal endoscopy, and the findings in the nasal cavity were evaluated using the Lund–MacKay staging system.Citation14 A subjective assessment was performed using the Nasolacrimal Duct Symptom Score questionnaire.Citation15 The surgical outcome was considered successful if saline solution freely reached the nose during lacrimal irrigation and if there was relief of symptoms.
Operative technique
Standardized general anesthesia was used. Nasal mucosa specimens were taken from over the rhinostomy site at the onset of the surgery for analysis of gene expression. The control specimens were taken from the lateral nasal wall at exactly the same site. The standardized, detailed endoscopic powered instrumentation technique used and the postoperative care have been described elsewhere.Citation16 No stents were used.
Quantitative reverse transcription polymerase chain reaction (qRT-PCR) for inflammatory cytokine genes
Human tissue samples reserved for RNA extraction from five patients undergoing EN-DCR surgery and five control patients were placed immediately into liquid nitrogen and thereafter stored at −70°C. RNA was extracted from tissue samples using an RNeasy® mini kit (74104; Qiagen, Valencia, CA, USA), according to the manufacturer’s instructions.
First, the tissue pieces were ground mechanically using a glass pestle homogenizer, including the kit buffer, and chilling the homogenizer on ice. The procedure also included a separate RNase-free DNase I treatment (79254; Qiagen) in the extraction column, as described in the kit protocol. Quantity and quality control of the extracted RNA was performed by spectrophotometric analysis.
Next, 500 ng of extracted RNA was reverse-transcribed to generate the corresponding DNA using a SuperScript® III first strand synthesis system (Life Technologies, Carlsbad, CA, USA). In brief, the protocol was as follows: 500 ng of purified RNA in 11 μL of RNase-free water was incubated with 50 ng random hexamers and 10 nmol dNTPs (deoxynucleotide triphosphates) for 5 minutes at 65°C; 100 nM DTT (dithiothreitol), 40 U RNAse OUT® (Life Technologies), and 200 U SuperScript® III reverse transcriptase were then added to the reaction, along with the appropriate amount of 5× First Strand Reaction Buffer. The complete reaction was subsequently incubated at 50°C for 50 minutes, after which the enzymes were inactivated at 70°C for 15 minutes. The generated complementary DNA (cDNA) samples were used immediately for analysis by qRT-PCR. SYBR® Green Real-Time PCR Master Mix (Life Technologies) and specific primer pairs for human interleukin (IL)-6, IL-1β, chemokine (C-C motif) ligand 2 (CCL2), and β-actin were used to determine the relative messenger (m) RNA expression in the samples. For IL-6, the primer pairs were forward, 5′-AGT GAG GAA CAA GCC AGA GC-3′ and reverse, 5′-CAG GGG TGG TTA TTG CAT CT-3′; for IL-1β, the primer pairs were forward, 5′-AAA AGC TTG GTG ATG TCT GG-3′ and reverse, 5′-TTT CAA CAC GCA GGA CAG G-3′; for CCL2, the primers were forward, 5′-CTC ATA GCA GCC ACC TTC ATT C-3′ and reverse, 5′-TCA CAG CTT CTT TGG GAC ACT T-3′; and for β-actin, the primers were forward, 5′-GGA TGC AGA AGG AGA TCA CTG-3′ and reverse, 5′-CGA TCC ACA CGG AGT ACT TG-3′. The primers were sourced from Oligomer Oy, Helsinki, Finland. The qRT-PCR reaction was run on an ABI Prism® 7500 Thermocycler (Life Technologies) using standard conditions. The data were analyzed using the ΔΔCt methodCitation17 and normalized using human β-actin expression as an internal control.
PCR array study for inflammatory response gene expression
cDNA for the array analysis was prepared using an RTCitation2 PreAMP cDNA synthesis kit (330451; Qiagen) following the manufacturer’s instructions. For both septoplasty and EN-DCR, five individually extracted RNAs were mixed in equal amounts (1 μg total, 200 ng of each) to provide templates for separate cDNA syntheses. A 96-well RTCitation2 Profiler™ PCR Array for Human Inflammatory Response and Autoimmunity (PAHS-077Z; SABiosciences/Qiagen) was used for the inflammation gene expression analysis, including the wells for control reactions. The SYBR® Green (Life Technologies) fluorescence detection methodology was employed. Thus, two one-plate runs were performed, ie, one for the septoplasty controls and the other for the EN-DCR samples. An Applied Biosystems 7500 Real-Time PCR System (Life Technologies) was used for PCR array amplification. All the quality control requirements stipulated by the manufacturer of the array were fulfilled in both PCR runs (including genomic DNA control, cDNA synthesis control, and positive PCR controls). The data were analyzed using the ΔΔCt methodCitation17 and normalized using human glyceraldehyde phosphate dehydrogenase expression as an internal control.
Results
The overall success rate after primary EN-DCR was 60% (3/5 patients) at the 6-month follow-up. On nasal endoscopy, the two failed patients showed tight fibrous scarring over the rhinostomy site, and one also had severe synechiae. Otherwise, there were no abnormal endoscopic findings according to the Lund–MacKay staging system.Citation14 No other intraoperative or postoperative complications occurred during the study period.
Inflammation-related gene expression profiling using PCR
qRT-PCR showed that gene expression for all inflammatory markers analyzed, ie, IL-6 (P=0.08), IL-1β (P=0.6), and CCL2 (P=0.03), was increased in the EN-DCR samples, but statistical significance was achieved only for CCL2 (). Due to a clear trend of increased inflammation in the EN-DCR samples, we performed a wider PCR array for inflammatory markers. Interestingly, there were notable differences between the groups with regard to inflammatory mediators (). The most significant findings in the EN-DCR samples when compared with controls were increased gene expression of the following: E-selectin (6.33-fold), IL-6 (5.23-fold), CCL16 (5.02-fold), tumor necrosis factor (TNF, 4.51-fold), CCL2 (3.77-fold), and CXCL3 (3.0-fold). On the other hand, notably decreased gene expression in EN-DCR samples over the controls was seen for: nitric oxide synthase 2 (0.17-fold), IL-8 (0.28-fold), CXCL1 (0.29-fold), IL-1 receptor antagonist (0.31-fold), CCR3 (0.32-fold), and FASLG (Fas ligand TNF superfamily member 6) (0.35-fold).
Figure 2 Expression of IL-6, IL-1β, and CCL2 mRNA in tissue samples of subjects undergoing either septoplasty (control) or EN-DCR surgery.
Abbreviations: IL, interleukin; mRNA, messenger RNA; EN-DCR, endoscopic dacryocystorhinostomy; qRT-PCR, quantitative reverse transcription polymerase chain reaction; SEM, standard error of the mean; CCL2, chemokine (C-C motif) ligand 2.
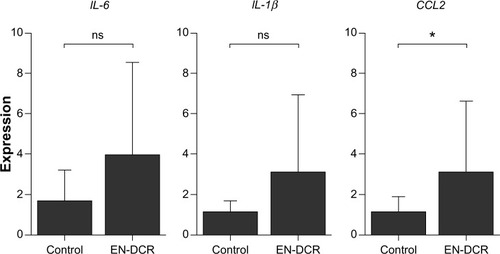
Table 2 Differences in expression of immune response-related genes analyzed by qRT-PCR array
Discussion
Our qRT-PCR results showed a clear trend toward increased transcription of IL-6, IL-1β, and CCL2. This finding was evident also from the PCR array, which additionally revealed notable differences in expression of several other inflammation-related mediators. There was a clearly increased expression of E-selectin mRNA, indicating an endothelial cell response in samples isolated from patients undergoing EN-DCR. By relatively weak carbohydrate interactions, E-selectin stimulates blood leukocytes to slow down and roll along the endothelium before their transmigration through the endothelium into the tissue.Citation18,Citation19 The endothelium can become activated by bacterial lipopolysaccharide, but in the case of NLDO, the activation is more probably mediated by proinflammatory cytokines, such as IL-1 and TNF-α. IL-1β and TNF-α together with a third acute phase protein, IL-6, are pleiotropic cytokines exerting a variety of effects on cellular function. In addition to contributing to acute and chronic inflammation, they have all been associated with the process of fibrosis.Citation20,Citation21 The continuing presence of inflammation and subsequent fibrosis, in turn, are considered to be the ultimate reason for NLDO.Citation1,Citation22
In acute inflammation, neutrophils are the primary leukocytes attracted to the inflammatory site.Citation22 In response to chemokines such as IL-8, neutrophils express their IL-6 receptors which activate endothelial cells to decrease their IL-8 production and to favor production of CCL2, which attracts monocytes in particular.Citation20 The decreased expression of IL-8 mRNA and increased expression of CCL2 in our NLDO samples suggest that the inflammation has passed through its initiation phase. The increased gene expression of CCL16, CXCL3, CCL13, and CCL3 in NLDO samples compared with those in controls also supports the transition toward a mononuclear cell type-dominated response.Citation23–Citation26 Our present results are in line with previous findings that inflammation is involved in the pathogenesis of NLDO.Citation1,Citation2
Nuclear factor kappa B (NF-κB) is a major transcription factor regulating the expression of many inflammation-related genes.Citation27 In addition to the induction of E-selectin,Citation19 NF-κB plays an important role in the expression of other genes, such as CCL2, CCL3, IL-6, IL-1β, and TNF-α, which were also strongly increased in samples from NLDO patients as compared with those from controls. In order to avoid overwhelming inflammation, NF-κB is kept under strict autoregulation.Citation19 The dynamic regulation probably results in no visible increase in expression of mRNA for NF-κB in EN-DCR patients.
In the present study, our success rate for primary EN-DCR was 60%, which is lower than our previously reported rate of 93%.Citation15 This difference may be explained by the small patient population recruited for this study. Although symptomatic relief was achieved in our two failed patients, our strict criteria categorized these patients as failures because irrigation was unsuccessful. The lack of studies examining the inflammation restricts our understanding of the underlying mechanisms causing NLDO. Therefore, we propose that the present study provides new important information. The profile of investigated markers suggests that inflammation has passed from its initiation state, which is in accordance with the previous findings that long-lasting inflammation is present in NLDO. Since the main reason for failure of EN-DCR is scarring over the rhinostomy site,Citation4,Citation5 an antifibrotic drug able to target fibrogenic factors or block their receptors could be beneficial. Therefore, a potential target for therapy to control the progression of fibrosis is currently being sought.Citation11 These potential inflammatory factors are promising candidates for future studies because they can be viewed as potential targets in the development of antifibrotic therapy intended for prevention of excessive scar formation.
Conclusion
The present study shows that expression of various inflammatory response-related genes is upregulated in the nasal mucosa of patients undergoing EN-DCR, but larger study populations are required to understand the details of these inflammatory responses.
Author contributions
Author contributions were as follows: EP, study planning, operations and clinical examination, manuscript writing; JMTH, analysis and interpretation of data, manuscript writing; MH, qRT-PCR measurements; AK, interpretation of data, manuscript writing; GS, study planning, manuscript writing; HT, study planning, manuscript writing; JS, study planning, manuscript writing; JN, manuscript writing; and KK, study planning, manuscript writing, and economic support. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by special government grant to the Kuopio University Hospital, the Finnish Cultural Foundation and its North Savo Fund, the Finnish Eye Foundation, the Finnish Funding Agency for Technology and Innovation, the Health Research Council of the Academy of Finland, and the Päivikki and Sakari Sohlberg Foundation. The study sponsors had no role in the study design, data collection, analysis and interpretation, or writing of the report.
Disclosure
The authors report no conflicts of interest in this work.
References
- BartleyGBAcquired lacrimal drainage obstruction: an etiologic classification system, case reports, and a review of the literature. Part 3Ophthal Plast Reconstr Surg1993911126
- LinbergJVMcCormickSAPrimary acquired nasolacrimal duct obstruction. A clinicopathologic report and biopsy techniqueOphthalmology1986938105510633763155
- LeongSCMacewenCJWhitePSA systematic review of outcomes after dacryocystorhinostomy in adultsAm J Rhinol Allergy2010241819020109333
- JokinenKKarjaJEndonasal dacryocystorhinostomyArch Otolaryngol1974100141444842611
- AllenKMBerlinAJLevineHLIntranasal endoscopic analysis of dacrocystorhinostomy failureOphthal Plast Reconstr Surg198843143145
- GoldbergRAEndonasal dacryocystorhinostomy: is it really less successful?Arch Ophthalmol2004122110811014718306
- MaurielloJAJrPalydowyczSDeLucaJClinicopathologic study of lacrimal sac and nasal mucosa in 44 patients with complete acquired nasolacrimal duct obstructionOphthal Plast Reconstr Surg1992811321
- PaulsenFPThaleABMauneSNew insights into the pathophysiology of primary acquired dacryostenosisOphthalmology2001108122329233611733281
- HeindlLMJunemannAHolbachLMA clinicopathologic study of nasal mucosa in 350 patients with external dacryocystorhinostomyOrbit200928171119229737
- OzerOEskiizmirGUnluHChronic inflammation: a poor prognostic factor for endoscopic dacryocystorhinostomyEur Arch Otorhinolaryngol2012269383984521833563
- SmirnovGPirinenRTuomilehtoHStrong expression of HSP47 in metaplastic nasal mucosa may predict a poor outcome after primary endoscopic dacryocystorhinostomy: a prospective studyActa Ophthalmol2011892e132e13619785638
- TaguchiTRazzaqueMSThe collagen-specific molecular chaperone HSP47: is there a role in fibrosis?Trends Mol Med2007132455317169614
- SakladMGrading of patients for surgical proceduresAnesthesia1941228
- LundVJMackayISStaging in rhinosinusitusRhinology19933141831848140385
- SmirnovGTuomilehtoHKokkiHSymptom score questionnaire for nasolacrimal duct obstruction in adults – a novel tool to assess the outcome after endoscopic dacryocystorhinostomyRhinology201048444645121442083
- SmirnovGTuomilehtoHTerasvirtaMSilicone tubing after endoscopic dacryocystorhinostomy: is it necessary?Am J Rhinol200620660060217181101
- WinerJJungCKShackelIWilliamsPMDevelopment and validation of real-time quantitative reverse transcriptase-polymerase chain reaction for monitoring gene expression in cardiac myocytes in vitroAnal Biochem19992701414910328763
- SawaYTsurugaEThe expression of E-selectin and chemokines in the cultured human lymphatic endothelium with lipopolysaccharidesJ Anat2008212565466318410313
- CollinsTReadMANeishASTranscriptional regulation of endothelial cell adhesion molecules: NF-kappa B and cytokine-inducible enhancersFASEB J19959108999097542214
- BarnesTCAndersonMEMootsRJThe many faces of interleukin-6: the role of IL-6 in inflammation, vasculopathy, and fibrosis in systemic sclerosisInt J Rheumatol2011201172160821941555
- OikonomouNHarokoposVZalevskyJSoluble TNF mediates the transition from pulmonary inflammation to fibrosisPLoS One20061e10817205112
- HaradaASekidoNAkahoshiTEssential involvement of interleukin-8 (IL-8) in acute inflammationJ Leukoc Biol19945655595647964163
- HowardOMDongHFShirakawaAKLEC induces chemotaxis and adhesion by interacting with CCR1 and CCR8Blood200096384084510910894
- SmithDFGalkinaELeyKGRO family chemokines are specialized for monocyte arrest from flowAm J Physiol Heart Circ Physiol20052895H1976H198415937099
- Garcia-ZepedaEACombadiereCRothenbergMEHuman monocyte chemoattractant protein (MCP)-4 is a novel CC chemokine with activities on monocytes, eosinophils, and basophils induced in allergic and nonallergic inflammation that signals through the CC chemokine receptors (CCR)-2 and -3J Immunol199615712561356268955214
- MaurerMvon StebutEMacrophage inflammatory protein-1Int J Biochem Cell Biol200436101882188615203102
- NewtonKDixitVMSignaling in innate immunity and inflammationCold Spring Harb Perspect Biol201243pii:a006049