Abstract
Purpose
The aim of the study reported here was to compare the improvement of visual acuity (VA) of diabetic and nondiabetic patients after neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser capsulotomy.
Methods
In this prospective cohort study, 50 age- and sex-matched patients, comprising 25 nondiabetics and 25 diabetics (referred to as Group A and B, respectively), with posterior chamber poly(methyl methacrylate) non-foldable intraocular lens implants attending our clinic at Karachi for capsulotomy had pre- and postoperative measures of VA, posterior pole visibility, and grading of posterior capsular opacity as seen on slit-lamp examination. VA was recorded before and after performing standard capsulotomy.
Results
The postoperative (mean) VA in nondiabetics was 0.25, 0.23, and 0.21 logMAR as compared with 0.25, 0.25, and 0.24 logMAR in diabetics at 1 week, 1 month, and 6 months, respectively. P-values of 0.47, 0.47, and 0.24, respectively, were determined, which were not significant. Preoperative VA improvement was recorded in 92% of diabetics in Group B and 96% of nondiabetics in Group A. Two (8%) diabetic patients developed glaucoma and did not participate in the study further.
Conclusion
Remarkable improvement in VA was achieved in both Group A and B, but the Group A nondiabetics showed more improvement in best-corrected VA after Nd:YAG laser capsulotomy.
Background
Posterior capsule opacification (PCO), also referred to as the “after cataract” or “secondary cataract,” is the most common late postoperative complication of cataract intraocular lens (IOL) surgery.Citation1–Citation3 It occurs in up to approximately 50% of patients within 2–3 years of their cataract surgery.Citation4–Citation6 Diabetic patients undergoing cataract surgery are at higher risk of postoperative complications. Diabetic patients have been reported to develop significantly greater PCO after cataract surgery than nondiabetic patients; however, the stage of retinopathy and the systemic status of diabetes did not correlate with the degree of PCO.Citation7
The current treatment of choice for PCO is neodymium-doped yttrium-aluminum-garnet (Nd:YAG) laser capsulotomy, which is an effective, safe, noninvasive procedure that does not require patient hospitalization.Citation8,Citation9 The procedure involves producing a central opening in the opacified posterior capsule, giving instantaneous results.Citation10
There is a paucity of literature prospectively evaluating improvement in the visual acuity (VA) of diabetic and nondiabetic patients after Nd:YAG laser posterior capsulotomy. Therefore, this study was designed to compare the rate and degree of improvement in VA between these two groups of patients.
Patients and methods
Study design
This was a prospective cohort unmasked study performed in a private setting. Study approval was obtained from the Ethics Filter Committee of the University of Ulster.
Patients and data collection
A total of 25 nondiabetic and 25 diabetic age- and sex-matched patients with posterior chamber poly(methyl methacrylate) (PMMA) non-foldable IOL implants were selected from among those attending our clinic using a non-probability convenience sampling technique. Patients included in the study gave their informed consent and were divided into two groups. Group A comprised nondiabetic subjects and was designated the non exposed group (n = 25). GroupB included subjects with a history of diabetes mellitus and was designated the exposed group (n = 25 eyes).
Inclusion criteria for Group B patients were glycosylated hemoglobin levels of ≥6% and use of diabetic treatment (oral hypoglycemic agents, insulin injection, or diet restriction). A week before the procedure, fasting blood glucose analysis was performed on all patients. Methods of treatment, duration of diabetes (for subjects in Group B), and ocular and systemic comorbidities were recorded. The inclusion criterion for patients of both groups regarding PCO was PCO of grade 3 or 4, according to Sellman and Lindstrom grading ().Citation11 Exclusion criteria were opacities in the media other than posterior capsular opacity or not matching the criteria for capsulotomy treatment; that is, corneal scars, irregularities or edema that interfered with target visualization or made the optical breakdown unpredictable, and inadequate stability of the eye or relative contraindications such as glass IOL, known or suspected cystoid macular edema, active intraocular inflammation and high risk for retinal detachment. Prior to capsulotomy, the patient’s visual function was recorded with their pupil in a normal physiological state in terms of best-corrected visual acuity (BCVA) using a Snellen VA chart kept at 6 m (20 ft) from the patient’s eyes.
Table 1 Sellman and Lindstrom posterior capsule opacification (PCO) gradesCitation11
Intraocular pressure (IOP) was measured. Pupil dilation was carried out with topical 1% tropicamide eye drops. The pupillary size was recorded after about 20 minutes using a millimeter scale and PCO was graded according to Sellman and Lindstrom grading (grades 1 to 4; ).Citation11
In case of dense posterior capsule opacity, B-scan ultrasonography was carried out to exclude any posterior segment pathology. Posterior pole assessment was performed with a Volk 90D lens (Volk Optical Inc, Mentor, OH, USA). The Madurai Intraocular Lens Study IV scale was used for grading of optic disc visualization ().Citation12
Table 2 Madurai intraocular lens study IV scale for optic disc visualizationCitation12
Macula visualization was graded subjectively according to the scale used by Aslam and Patton ().Citation13
Table 3 Macula visualization scale used by Aslam and PattonCitation13
Nd:YAG laser capsulotomy
All Nd:YAG laser capsulotomy procedures were performed on a Visulas® YAG II (Carl Zeiss Meditec, Jena, Germany). The wavelength of therapy beam was 1064 nm. Radiation was produced by a Q-switched mode. It was initially set at 1 mJ then subsequently raised to 5 mJ stepwise as necessary to pierce the posterior capsule. Capsulotomy was performed in a cross fashion; size of capsulotomy ranged between 3–4 mm. Once the procedure was completed, one drop of dexamethasone and one drop of levobunolol eye drops were instilled. When higher energy levels (4.5–6.0 mJ) were used, one tablet of acetazolamide (Tablet AZM 250 mg; Ethical Laboratories, Lahore, Pakistan) was also given immediately.
IOP was monitored for 1 hour following the procedure and then the patient was discharged on dexamethasone eye drops 0.1% four times daily and levobunolol eye drops twice daily. Post Nd:YAG laser treatment was continued for 2 weeks. Patients’ visual function was reassessed again, as described earlier, on subsequent visits 1 day, 1 week, 1 month, 3 months, and 6 months after the procedure.
Data analysis
Data were entered into and analyzed with SPSS (v 11.0; IBM Corporation, Armonk, NY, USA). Frequency and percentage were computed for categorical variables like sex. The mean and standard deviation (SD) were estimated for quantitative variables such as post operative VA. For inferential statistics, the chi square test/Fisher exact test was used for the comparison of categorical variables, and for numerical variable t-test was used, such as type of PCO. P-value <0.05 was considered significant.
Results
Fifty patients, comprising 25 nondiabetic and 25 diabetic age- and sex-matched patients of South Asian origin with posterior chamber PMMA non-foldable IOL implants with PCO, of whom 24 were female, were examined and Nd:YAG laser capsulotomy was performed (–). The mean age ± SD was 60.44 ± 5.00 and 60.52 ± 5.00 years for nondiabetics and diabetics, respectively. The mean period between cataract extraction and performing Nd:YAG laser capsulotomy was 16 ± 2 months (). Capsular fibrosis was the predominant type of PCO ().
Figure 1 Sex distribution among nondiabetic patients (n = 25) in the study.
Figure 2 Sex distribution among diabetic patients (n = 25) in the study.
Figure 3 Comparison between nondiabetic (n = 25) and diabetic (n = 25) study groups of time elapsed since cataract surgery.
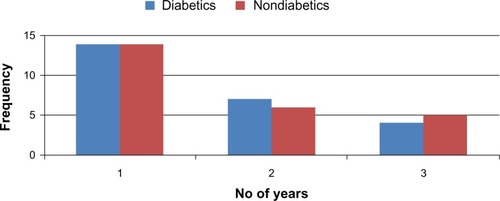
Table 4 Types of posterior capsule opacification (PCO) in diabetics and nondiabetics (N = 50) with P values
Similar ocular comorbid diseases were present in both groups. The most common systemic comorbid disorder found was hypertension. It was less common in nondiabetics (20%) than in diabetics (58%) ().
Table 5 Frequency of comorbid systemic and ocular diseases in patients
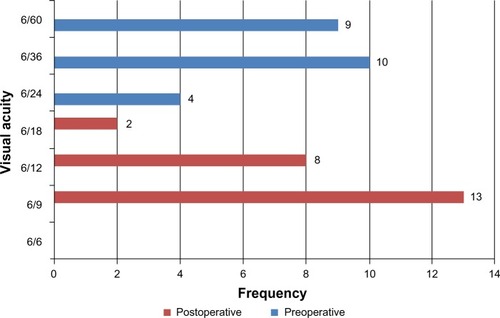
The minimum preoperative BCVA in both groups was not less than 6/60 (20/200) on the Snellen chart. Good VA results were noted more commonly in nondiabetic patients than in diabetic patients. However, this difference was not statistically significant. The mean ± SD postoperative VA in nondiabetics was 0.25 ± 0.09, 0.23 ± 0.09, and 0.21 ± 0.08 logMAR at 1 week, 1 month, and 6 months, respectively (), as compared with 0.27 ± 0.10, 0.24 ± 0.09, and 0.24 ± 0.09, respectively, in diabetics (). In nondiabetics, 96% (24/25) of patients showed a mean ± SD BCVA improvement of 0.21 ± 0.08 logMAR, while 4% (1/25) of patients showed a BCVA of 0.00 logMAR after capsulotomy – that is, full visual recovery – while, for diabetics, the mean visual improvement was 0.24 ± 0.09 logMAR; P=0.24.
Figure 4 Comparison of pre- and postsurgical visual acuity among nondiabetic study participants (n = 25).
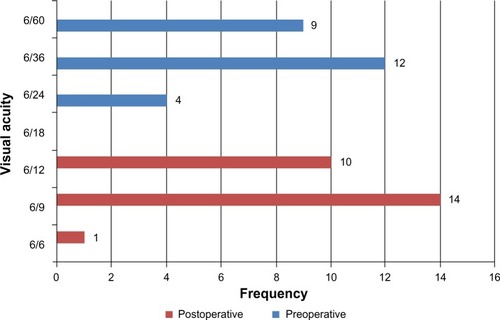
Figure 5 Comparison of pre- and postsurgical visual acuity among diabetic study participants (n = 25).
The (mean) postoperative improvement in VA between diabetic and nondiabetic patients after Nd:YAG was calculated by t-testing at 1 week, 1 month, 3 months, and 6 months following the procedure. The P-value was 0.47 at 1 week and 1 month, and 0.24 at 3 and 6 months, none of which were significant.
No other complications were encountered, except two (8%) patients in the diabetic group (4% of the total study population) developed persistent raised IOP 24 hours after Nd:YAG laser, which finally culminated in glaucoma. These two patients did not participate in the study further. Later, it was established that they had undiagnosed open-angle glaucoma.
The mean postoperative improvement in VA of both groups is shown in .
Table 6 Postoperative visual acuity after Nd:YAG laser capsulotomy (mean ± standard deviation)
Discussion
Nd:YAG laser capsulotomy is indicated for the treatment of opacification of the posterior capsule resulting in decreased VA or visual function, or both.Citation14 The period between cataract extraction and performing Nd:YAG laser capsulotomy was 16 ± 2 months in our study, while it was 3 years in the study by Flach and Dolan.Citation15 The relative incidence of different types of PCO showed that capsular fibrosis was the predominant type of PCO; this finding is in contrast with the findings of Hassan et al, who reported Elschnig’s pearls in pseudophakic eyes and secondary fibrosis in aphakic eyes.Citation16
Hypertension, which was the most common comorbid disease, was found to be more prevalent in the diabetic group (58% vs 20.0%). On applying chi-square test to calculate the P-values for co-morbidities it was found to be 0.02 for hypertension, which is significant, while for other co-morbidities (such as peptic ulcer disease and chronic obstructive airway disease) the P-values were 0.99 and 0.50.
There was spectacular improvement in VA according to Snellen chart testing after Nd:YAG laser capsulotomy. In Group A (nondiabetics), 96% of patients improved from two to five lines on the Snellen chart, while a Snellen chart VA improvement of 2–5 lines was recorded for 92% of Group B (diabetics). It was also noted that there was no further deterioration of VA in any case. In Hassan et al’s study, Snellen chart VA improvement after Nd:YAG laser capsulotomy was 1–3 lines in 42 out of 86 (49%) patients, 4–6 lines in 31 out of 86 (36.04%) patients, and there was no VA improvement in 13 (15.11%) cases due to comorbidities.Citation16
We encountered complications in our study in only two patients from Group B who developed persistent raised IOP 24 hours after Nd:YAG laser capsulotomy. These two patients comprised 8% of the exposed group, which disagrees with Steinert et al, who estimated that the incidence of glaucoma developing after capsulotomy was 1%–6%.Citation17 Thus, incidence of rise in IOP was high in our study, despite all patients having posterior chamber IOL implantation, their being selected with normal IOP, and our use of very low energy levels in the capsulotomy procedure. No evidence of cystoid macular edema, retinal detachment, iritis, or corneal or IOL damage was noted in this series of Nd:YAG posterior capsulotomies. To prevent complications, all factors should be kept in mind, such as the power of the Nd:YAG laser being used, the focusing mechanism of the instrument, separation between posterior capsule and IOL, type of IOL, and the operator’s experience.
Limitations
It is possible that the figures in this study are underestimated because the length of follow-up was short (ie, 6 months) and as the sample size of this study was also small.
Conclusion
Although there was equal chance of BCVA improvement in both groups, as the diabetic subjects had a greater risk of developing complications, improvement in BCVA was less in this group than in the nondiabetic group after Nd:YAG laser capsulotomy.
Acknowledgments
Dr Muhammed Tayyab Awan would like to thank Professors Tara Moore and Antonio Leccisotti, and also Shirley Sharron, of the University of Ulster for their support and guidance throughout the study and the writing of this paper.
Disclosure
All authors were involved in the planning, designing, and executing of the study reported herein, and in the writing of this paper. The authors have no conflicts of interest in this work.
References
- AppleDJInfluence of intraocular lens material and design on postoperative intracapsular cellular reactivityTrans Am Ophthalmol Soc20009825728311190028
- WernerLAppleDJPandeySKPostoperative proliferation of anterior and equatorial lens epithelial cells: a comparison between various foldable IOL designsBurattoLOsherRHMasketSCataract Surgery in Complicated CasesThorofare, NJSlack2000399417
- ZemaitieneRPosterior capsule opacification: incidence and pathogenesisMedicina (Kaunas)2003399830837 Lithuanian14515044
- SpaltonDJPosterior capsular opacification after cataract surgeryEye (Lond)199913Pt 3b48949210627830
- AwasthiNGuoSWagnerBJPosterior capsular opacification: a problem reduced but not yet eradicatedArch Ophthalmol2009127455556219365040
- AppleDJPengQVisessookNEradication of posterior capsule opacification: documentation of a marked decrease in Nd:YAG laser posterior capsulotomy rates noted in an analysis of 5416 pseudophakic human eyes obtained postmortemOphthalmology2001108350551811237905
- HayashiKHayashiHNakaoFHayashiFPosterior capsule opacification after cataract surgery in patients with diabetes mellitusAm J Ophthalmol20021341101612095802
- PolakMZarnowskiTZagórskiZResults of Nd:YAG laser capsulotomy in posterior capsule opacificationAnn Univ Mariae Curie Sklodowska Med200257135736312898944
- BurqMATaquiAMFrequency of retinal detachment and other complications after neodymium:Yag laser capsulotomyJ Pak Med Assoc2008581055055218998307
- SenneFMTemporiniERArietaCEPachecoKDPerception of difficulties with vision-related activities of daily living among patients undergoing unilateral posterior capsulotomyClinics (Sao Paulo)201065545946820535363
- TamiRSellmanTRLindstromRLEffect of a plano-convex posterior chamber lens on capsular opacification from Elschnig pearl formationJ Cataract Refract Surg198814168723339551
- VenkateshNPrajnaNVEllweinLBSelvarajSManjulaKKupferCThe Madurai Intraocular Lens Study IV: posterior capsule opacificationAm J Ophthalmol2000130330430911020409
- AslamTMPattonNMethods of assessment of patients for Nd:YAG laser capsulotomy that correlate with final visual improvementBMC Ophthalmol200441315387889
- SteinertRFNeodymium:yttrium-aluminum-garnet laser posterior capsulotomySteinertRFCataract Surgery3rd edPhiladelphia, PASaunders Elsevier2010617630
- FlachAJDolanBJIncidence of postoperative posterior capsular opacification following treatment with diclofenac 0.1% and ketorolac 0.5% ophthalmic solutions: 3-year randomized, double-masked, prospective clinical investigationTrans Am Ophthalmol Soc20009810110711190013
- HassanKSAdhiMIAzizMNd:YAG laser posterior capsulotomyPak J Ophthalmol19961237
- SteinertRFPuliafitoCAKumarSRDudakSDPatelSCystoid macular edema, retinal detachment, and glaucoma after Nd:YAG laser posterior capsulotomyAm J Ophthalmol199111243733801928237