
Abstract
The objective of this study was to evaluate the relations among electroretinogram (ERG) parameters (cone a-wave, cone b-wave, and 30 Hz flicker), retinal thickness, and retinal volume in 16 patients with central retinal vein occlusion and macular edema. The amplitude and implicit time of the ERG parameters were extracted from the ERG traces. Retinal thickness and volume were measured by optical coherence tomography in nine macular subfields. Then the correlations among ERG parameters and morphological parameters were analyzed. The cone b-wave and 30 Hz flicker implicit time were correlated with retinal thickness and volume in seven out of nine subfields, excluding the temporal subfields. In addition, the amplitude of the cone b-wave was correlated with retinal thickness and volume in the nasal inner and nasal outer subfields. These findings suggest that retinal thickness and volume may be associated with outer and inner retinal function in central retinal vein occlusion patients.
Introduction
Central retinal vein occlusion (CRVO) often leads to macular edema, which is the most frequent cause of visual impairment in CRVO patients. Optical coherence tomography (OCT) is used to assess retinal thickness and morphology in CRVO patients with macular edema, but it has been reported that a decrease of macular thickness was not associated with a corresponding improvement of vision, indicating that there is a discrepancy between OCT findings and the visual prognosis.Citation1,Citation2 Accordingly, an objective and reproducible measure of retinal function is needed to allow accurate assessment of the efficacy of treatment. Investigation of the correlation between functional and anatomic parameters could help to determine which parameters are relevant in this context, indicating that it is important to investigate the relation between retinal function and morphologic changes in CRVO patients with macular edema.
The electroretinogram (ERG) is an objective measure of retinal function, but there is controversy regarding which ERG parameter is most useful for monitoring patients with retinal vein occlusion.Citation3,Citation4 In patients with CRVO, many studies have shown that the full-field ERG, particularly the b-wave implicit time of the 30 Hz flicker ERG, is a good predictor of the development of neovascular glaucoma.Citation5,Citation6 The cone a-wave, cone b-wave, and 30 Hz flicker of the ERG not only reflect macular function, but also retinal function.Citation7 In animal models of branch retinal vein occlusion (BRVO), ERG studies have demonstrated moderate to severe functional deficits of the photoreceptor, bipolar, amacrine, and ganglion cells.Citation8 However, the relation between ERG parameters and retinal morphology in CRVO patients with macular edema remains unclear, and limited information is available about the value of the ERG for assessing the macular area affected by CRVO.
In the present study, we measured ERG and anatomical parameters in CRVO patients with macular edema. Then we evaluated the relations among ERG parameters (cone a-wave, cone b-wave, and 30 Hz flicker) and the retinal thickness and retinal volume measured by OCT.
Materials and methods
Patients
Sixteen patients with a mean age of 69.9±11.9 years (eleven women and five men) and unilateral CRVO were included in this prospective, uncontrolled study that was conducted at the Department of Ophthalmology at Tokyo Women’s Medical University (). The mean duration of CRVO was 4.8±3.3 months (range: 1–12 months).
Table 1 Clinical and demographic data of the CRVO patients
Each patient underwent baseline screening that included slit-lamp examination and ophthalmoscopy, fluorescein angiography, ERG, and measurement of retinal thickness and retinal volume by OCT.
A masked grader independently assessed ischemic retinal vascular occlusion by examination of fluorescein angiograms. The ischemic region of the retina was measured using the public domain Scion Image program (Scion Corporation, Frederick, MD, USA).Citation9 In brief, the optic disc was outlined with a cursor on digital photographs of the fundus and its area was measured, after which the same was done for the nonperfused area of the retina. Then the nonperfused area was divided by the disc area to calculate an index of the severity of retinal ischemia.
The unaffected contralateral eyes of the 16 CRVO patients were used as the controls. Hypertension was diagnosed if a patient had a systolic blood pressure ≥140 mmHg, a diastolic blood pressure ≥90 mmHg, or a systolic pressure ≥140 mmHg at one reading and a diastolic pressure ≥90 mmHg at a different reading, or was already taking antihypertensive medication. A diagnosis of hyperlipidemia was based on a serum total cholesterol level ≥240 mg/dL, triglycerides ≥160 mg/dL, or low-density lipoprotein cholesterol ≥130 mg/dL, or on current use of lipid-lowering medication.
The exclusion criteria were 1) intraocular surgery (including cataract extraction) within 6 months before enrollment, 2) diabetes mellitus/diabetic retinopathy, 3) previous laser photocoagulation of the macular region, 4) intravitreal injection of triamcinolone acetonide or antivascular endothelial growth factor (anti-VEGF) agents, 5) prior ocular inflammation, 6) retinal degeneration, 7) marked retinal hemorrhage (including macular bleeding into the intrafoveal or subfoveal spaces), and 8) retinal neovascularization or rubeosis.
Informed consent was obtained from each participant. This study was performed in accordance with the Helsinki Declaration of 1975 (1983 revision), and was approved by the ethics committee of Tokyo Women’s Medical University.
OCT
OCT was performed with a Zeiss Time Domain Stratus OCT3 apparatus (Carl Zeiss Meditec, Dublin, CA, USA), and it revealed that all patients had cystoid macular edema of ≥250 μm involving the central fovea. A retinal thickness map and retinal volume map were obtained by scanning the macula in 6 × 6 mm (20° × 20°) areas. The two retinal maps were each divided into the following nine subfields: 1) fovea, 2) superior inner macula, 3) nasal inner macula, 4) inferior inner macula, 5) temporal inner macula, 6) superior outer macula, 7) nasal outer macula, 8) inferior outer macula, and 9) temporal outer macula.Citation10 The diameter of the center, inner, and outer rings was 1, 3, and 6 mm, respectively. In each of the nine regions, measurement of retinal thickness and retinal volume was automatically performed by computer analysis. Then the correlations between retinal thickness or retinal volume and ERG parameters were analyzed in each of the nine subfields.
ERG recording
After OCT had been completed the photopic ERG was recorded in both eyes of each patient using a Portable LE2000 ERG system (Tomey Co, Ltd Nagoya, Japan). The recording electrode was a contact lens electrode carrying light emitting diodes (EW-102; Mayo, Inazawa, Japan), which provided the white stimuli and background light and had the same effect as a Ganzfeld dome system. Before recording, the patient’s pupils were maximally dilated. After the contact lens recording electrodes were positioned the patient underwent light adaptation for 10 minutes before recording of the ERG. The reference electrode was placed on the forehead and the ground electrode was placed on one earlobe. After waiting another 10 minutes, the photopic ERG was elicited by 3-ms white stimuli of 3.0 cd/m2 and the Light Adapted 3.0 Flicker ERG was elicited by 3.0 log cd/m2 stimuli. Both cone stimuli were presented on a white background of 30 cd/m2 according to the recommendations of the International Society of Clinical Electrophysiology of Vision.Citation11 Data from both eyes were analyzed.
Statistical analysis
All analyses were performed with SAS System 9.1 software (SAS Institute Inc, Cary, NC, USA). Results are presented as the mean ± standard deviation or as frequencies. Student’s t-test was employed to compare normally distributed unpaired continuous variables between the groups. To examine the correlations between retinal thickness or retinal volume and ERG parameters, Pearson’s correlation coefficients were calculated. Correlations between ERG parameters and the nonperfused area of the retina were also determined by Pearson’s correlation coefficient analysis. In all analyses, two-tailed P-values of less than 0.05 were considered to indicate statistical significance.
Results
Best-corrected visual acuity ranged from 20/2,000 to 20/33.3 (median 20/100). The mean values of the cone a-wave, cone b-wave, and 30 Hz flicker are shown in . The amplitudes of the cone b-wave and 30 Hz flicker wave were significantly smaller in the eyes with CRVO and macular edema than in the unaffected contralateral eyes (P=0.003 and P=0.004, respectively) (). The implicit times of the cone a-wave, cone b-wave, and 30 Hz flicker were significantly longer in the eyes with CRVO and macular edema than in the unaffected contralateral eyes (P=0.011, P<0.001, and P<0.001, respectively) (). shows the mean retinal thickness and retinal volume for each of the nine subfields. displays a representative fundus color photograph, along with measurement of retinal thickness by OCT and an ERG from the same patient.
Figure 1 Representative fundus color photograph, measurement of retinal thickness by OCT, and an ERG for the same eye.
Abbreviations: CRVO, central retinal vein occlusion; ERG, electroretinogram; OCT, optical coherence tomography.
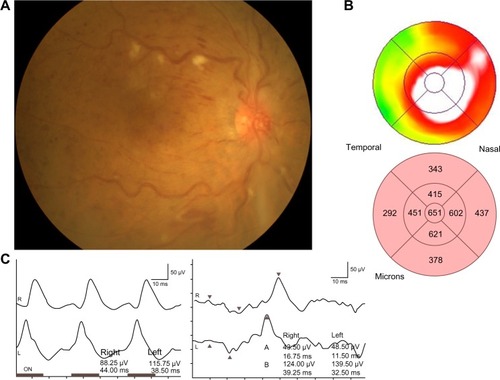
Table 2 Comparison of ERG parameters between the affected eyes and unaffected contralateral eyes of the CRVO patients
Table 3 Anatomic measurements in the CRVO patients with macular edema
The association between ERG parameters and retinal morphologic parameters (retinal thickness and retinal volume) in each of the nine subfields is shown in and . The cone a-wave (amplitude and implicit time) and 30 Hz flicker (amplitude) were not correlated with the retinal thickness in any of the subfields. However, the amplitude of the cone b-wave was correlated with retinal thickness in the nasal inner and nasal outer subfields (). In addition, the cone b-wave and 30 Hz flicker implicit time were correlated with retinal thickness for seven out of nine subfields, excluding the temporal subfields ().
Table 4 Association between ERG parameters and retinal thickness in the nine macular subfields
Table 5 Association between ERG parameters and retinal volume in the nine macular subfields
The cone a-wave (amplitude and implicit time) and 30 Hz flicker (amplitude) were not correlated with the retinal volume in any of the subfields, but the amplitude of the cone b-wave was correlated with retinal volume in the nasal inner and nasal outer subfields (). Also, the cone b-wave and 30 Hz flicker implicit time were correlated with retinal volume for seven out of nine subfields, excluding the temporal subfields ().
The implicit times of the cone b-wave (ρ=0.62, P=0.011) and 30 Hz flicker (ρ=0.54, P=0.031) were significantly correlated with the nonperfused area of the retina (). However, the amplitude of the cone a-wave (ρ=−0.28, P=0.287), cone b-wave (ρ=−0.41, P=0.115), and 30 Hz flicker (ρ=−0.25, P=0.350), as well as the implicit time of the cone a-wave (ρ=0.28, P=0.290), were not significantly correlated with the nonperfused area ().
Table 6 Correlations between ERG parameters and the nonperfused area of the retina
Discussion
The present study demonstrated that the implicit times of the cone b-wave and 30 Hz flicker were correlated with both retinal thickness and volume in seven out of nine macular subfields, excluding the temporal subfields. These findings suggest that both macular thickness and macular volume were related to the implicit times of the cone b-wave and 30 Hz flicker in our CRVO patients. Both the cone b-waveCitation7,Citation12 and the 30 Hz flickerCitation6,Citation7,Citation13,Citation14 have been reported to reflect inner retinal function. Therefore, our findings indicate that data obtained from macular subfields (excluding the temporal subfields) may be associated with outer and inner retinal function in CRVO patients with macular edema. Thus, morphological changes of the non-temporal subfields may influence macular function, so that measuring ERG parameters (especially the cone b-wave and 30 Hz flicker implicit time) of these subfields might be useful for estimating macular function and the response to treatment such as anti-VEGF therapy.
We also found that the amplitude of the cone b-wave was correlated with both retinal thickness and retinal volume in only two subfields (the nasal inner and nasal outer subfields). Interestingly, these results were the opposite to those obtained in BRVO patients, in whom ERG parameters showed a stronger correlation with morphological parameters in the temporal subfield than in other subfields.Citation10 It is possible that pathological changes induced by CRVO (such as bleeding) are more likely to affect the region extending from the optic nerve to the nasal part of the macula, since it contains the papillomacular bundle with a high axon density and an abundance of retinal ganglion cells, parasol cells, and dendrites that form part of the postreceptoral cone pathway.Citation15 Therefore, the difference of macular thickness and volume between the nasal region of the macula and the temporal region would probably be greater in CRVO compared with BRVO, leading to a stronger correlation with ERG parameters (cone b-wave amplitude and the cone b-wave and 30 Hz flicker implicit times). However, further investigations will be needed to clarify the relations between ERG parameters and retinal morphology in CRVO patients.
The present study demonstrated that the implicit times of cone b-wave and 30 Hz flicker were significantly correlated with the nonperfused area of the retina. Because retinal photoreceptor cells are damaged by ischemia, functional impairment may become more severe as the ischemic region becomes larger. Ischemic retinal cells react slowly, as demonstrated by ERG recording in cats after photothrombosis.Citation16 This has also been demonstrated by full-field ERG studies of patients with widespread retinal ischemia, since the implicit time of the 30 Hz flicker ERG reflected the ischemic status of the retina and predicted development of neovascular complications in CRVO patients.Citation5,Citation14,Citation17,Citation18 In addition, Hvarfner et alCitation19 studied the multifocal ERG (mfERG) and reported that the implicit time was significantly longer in eyes with macular ischemia than in eyes without macular ischemia, and the mfERG amplitudes were lower in ischemic eyes with retinal vein occlusion. A correlation between prolongation of the implicit time and retinal ischemia was also suggested by Greenstein et al.Citation20 They found that macular edema in diabetic retinopathy was related to a prolonged implicit time, but the retinal area with an altered implicit time was much larger than the area of edema, and they proposed ischemia as a possible explanation. We recently reported that increased intraocular levels of VEGF and soluble intercellular adhesion molecule 1, as well as a decrease of pigment epithelium-derived factor, were associated with increased retinal vascular permeability and with the severity of retinal ischemia in CRVO patients.Citation21,Citation22 Thus, as retinal ischemia becomes more severe, changes of these factors result in progression of macular edema that also worsens ischemia, with the result that macular function may be impaired. This hypothesis is supported by the report that the implicit times of the cone b-wave and 30 Hz flicker were significantly correlated with the VEGF concentration of the aqueous humor in patients with macular edema secondary to CRVO.Citation23
The mfERG provides more localized data about retinal function than the full field ERG. Previous studies have demonstrated that mfERG abnormalities are generally well correlated with local changes in patients with retinal vein occlusion.Citation24 Dolan et alCitation25 found that retinal injury due to hemiretinal vein occlusion leads to significant prolongation of the implicit time on both ERG and mfERG, suggesting that these two modalities may have a role in the management of this type of retinal vein occlusion. In the present study, we evaluated the correlation of Ganzfeld ERG parameters with OCT parameters because we did not have access to mfERG. Moschos and MoschosCitation26 used mfERG and OCT to show that intravitreal injection of bevacizumab can lead to anatomical and functional improvement of the macular region in CRVO patients with macular edema. Thus, the assessment of structural and functional changes by mfERG and OCT might be useful for monitoring the response to anti-VEGF therapy in CRVO patients with macular edema. However, further investigations will be needed to clarify how useful ERG parameters are for correlating morphology and retinal function in CRVO with macular edema.
In conclusion, the amplitude of the cone b-wave was correlated with both retinal thickness and retinal volume in the nasal inner and nasal outer macular subfields, while the cone b-wave and 30 Hz flicker implicit time were correlated with both retinal thickness and retinal volume for seven out of nine subfields, excluding the temporal subfields. Our findings suggest that ERG parameters may be associated with outer and inner retinal function in CRVO patients with macular edema. Changes in ERG parameters may be related to morphological changes that influence macular function, so that measuring ERG parameters (especially the cone b-wave and 30 Hz flicker implicit time) might be useful for estimating macular function and the response to treatment in CRVO.
Disclosure
The authors report no conflicts of interest in this work.
References
- Martínez-JardónCSMeza-de RegilADalma-WeiszhauszJRadial optic neurotomy for ischaemic central vein occlusionBr J Ophthalmol200589555856115834084
- KumagaiKFurukawaMOginoNUemuraALarsonELong-term outcomes of vitrectomy with or without arteriovenous sheathotomy in branch retinal vein occlusionRetina2007271495417218915
- HayrehSSKlugmanMRPodhajskyPKolderHEElectroretinography in central retinal vein occlusion. Correlation of electroretinographic changes with pupillary abnormalitiesGraefes Arch Clin Exp Ophthalmol198922765495612483144
- WilliamsonTHKeatingDBradnamMElectroretinography of central retinal vein occlusion under scotopic and photopic conditions: what to measure?Acta Ophthalmol Scand199775148539088401
- LarssonJAndreassonSBauerBCone b-wave implicit time as an early predictor of rubeosis in central retinal vein occlusionAm J Ophthalmol199812522472499467454
- LarssonJBauerBAndréassonSThe 30-Hz flicker cone ERG for monitoring the early course of central retinal vein occlusionActa Ophthalmol Scand200078218719010794254
- MustafiDEngelAHPalczewskiKStructure of cone photoreceptorsProg Retin Eye Res200928428930219501669
- ZhangYFortuneBAtchaneeyasakulLONatural history and histology in a rat model of laser-induced photothrombotic retinal vein occlusionCurr Eye Res200833436537618398711
- NomaHFunatsuHYamasakiMPathogenesis of macular edema with branch retinal vein occlusion and intraocular levels of vascular endothelial growth factor and interleukin-6Am J Ophthalmol2005140225626116086947
- NomaHFunatsuHHarinoSSugawaraTMimuraTShimadaKAssociation of electroretinogram and morphological findings in branch retinal vein occlusion with macular edemaDoc Ophthalmol20111232839121805173
- MarmorMFFultonABHolderGEMiyakeYBrigellMBachMInternational Society for Clinical Electrophysiology of VisionISCEV Standard for full-field clinical electroretinography (2008 update)Doc Ophthalmol20091181697719030905
- SievingPAPhotopic ON- and OFF-pathway abnormalities in retinal dystrophiesTrans Am Ophthalmol Soc1993917017738140708
- BushRASievingPAInner retinal contributions to the primate photopic fast flicker electroretinogramJ Opt Soc Am A Opt Image Sci Vis19961335575658627412
- LarssonJAndréassonSPhotopic 30 Hz flicker ERG as a predictor for rubeosis in central retinal vein occlusionBr J Ophthalmol200185668368511371488
- PavlidisMStuppTHummekeMThanosSMorphometric examination of human and monkey retinal ganglion cells within the papillomacular areaRetina200626444545316603965
- IkedaHHankinsMWAsaiTDawesEAElectrophysiological properties of neurones following mild and acute retinal ischaemiaExp Eye Res19925534354421426075
- BretonMEQuinnGEKeeneSSDahmenJCBruckerAJElectroretinogram parameters at presentation as predictors of rubeosis in central retinal vein occlusion patientsOphthalmology1989969134313522476699
- SevernsMLJohnsonMAPredicting outcome in central retinal vein occlusion using the flicker electroretinogramArch Ophthalmol19931118112311307688951
- HvarfnerCAndréassonSLarssonJMultifocal electroretinography and fluorescein angiography in retinal vein occlusionRetina200626329229616508429
- GreensteinVCHolopigianKHoodDCSeipleWCarrREThe nature and extent of retinal dysfunction associated with diabetic macular edemaInvest Ophthalmol Vis Sci200041113643365411006263
- NomaHFunatsuHMimuraTEguchiSShimadaKHoriSVitreous levels of pigment epithelium-derived factor and vascular endothelial growth factor in macular edema with central retinal vein occlusionCurr Eye Res201136525626321275514
- NomaHFunatsuHHarinoSMimuraTEguchiSHoriSVitreous inflammatory factors in macular edema with central retinal vein occlusionJpn J Ophthalmol201155324825521538003
- YasudaSKachiSKondoMSignificant correlation between electroretinogram parameters and ocular vascular endothelial growth factor concentration in central retinal vein occlusion eyesInvest Ophthalmol Vis Sci20115285737574221642626
- HasegawaSOhshimaAHayakawaYTakagiMAbeHMultifocal electroretinograms in patients with branch retinal artery occlusionInvest Ophthalmol Vis Sci200142129830411133882
- DolanFMParksSKeatingDDuttonGNWide field multifocal and standard full field electroretinographic features of hemi retinal vein occlusionDoc Ophthalmol20061121435216633725
- MoschosMMMoschosMIntraocular bevacizumab for macular edema due to CRVO. A multifocal-ERG and OCT studyDoc Ophthalmol2008116214715218189152