
Abstract
Topical Bimatoprost is a common and popular prostaglandin analog used as an ocular hypotensive agent in the treatment of glaucoma. Side effects include ocular hyperaemia, ocular pruritus, and periocular and iris pigmentary changes. Perioribital lipodystrophy is another well-documented outcome associated with chronic use of topical bimatoprost, which results in periorbital hallowing, upper eyelid sulcus deepening, eyelid retraction and enophthalmos. We report an unusual case of periocular muscle atrophy and weakness from unilateral topical bimatoprost use. Our patient had primary angle closure and experienced a right upper eyelid ptosis 2 months after she started to use topical bimatoprost in that eye. Clinical measurements of her eyelids clearly showed reduction in the function of her right levator muscle, suggesting that effects of topical bimatoprost may not be limited to periorbital fat. She was advised to stop topical bimatoprost and right ptosis correction surgery with levator muscle advancement was performed successfully. Ophthalmologists and patients should be aware of this potential rare side effect of topical bimatoprost, as it may be potentially disfiguring, especially with monocular use. However, its exact mechanism of action needs to be clarified further.
Introduction
Topical bimatoprost is a popular prostaglandin analog used primarily as a powerful ocular hypotensive agent for treatment of glaucoma (approved in 2001). It is also used cosmetically to induce hypertrichosis, approved by the US Food and Drug Administration in 2008 as Latisse (Allergan, Inc, Irvine, CA, USA). However, it may cause complications such as periocular skin hyperpigmentation, intraocular inflammation, and conjunctival hyperemia.Citation1 These mainly affect superficial tissues and, to date, there has been no report on involvement of deeper periocular tissues as far as we are aware. Herein, we report an unusual case of periocular muscle atrophy and weakness secondary to unilateral topical bimatoprost use.
Case report
A 58-year-old Chinese female was referred to the oculoplastics services of National University Hospital, Singapore, for right upper eyelid ptosis of 1.5 years’ duration and difficulty in closing her right eye. She had a history of bilateral primary angle closure diagnosed in 2003, for which bilateral laser peripheral iridotomies were performed. She was started on topical latanoprost 0.005% once every night to the right eye, as intraocular pressure (IOP) was suboptimal. Subsequently, she underwent an uneventful right cataract extraction with intraocular lens implantation that same year. As IOP remained optimal postoperatively, she was taken off topical latanoprost. Her condition remained stable until 2008 when there were progressive defects in her right visual field with increased IOP. Thus, she was started on topical bimatoprost 0.03% (Lumigan, Allergan, Inc) once every night to her right eye.
On review after 3 months, IOP was found to have been controlled adequately. However, she reported an onset of right upper eyelid drooping 2 months after starting treatment. There was no history of trauma or eyelid surgery. The ptosis did not show any diurnal variability or fatigability, and there was no diplopia. A detailed evaluation by the neuro-ophthalmology team revealed no underlying neurological cause. Four months after starting treatment, the treated eye was found to have long eyelashes and ocular pigmentation. Subsequently, the patient reported worsening of her right ptosis after 12 months on treatment and was keen for referral to the oculoplastics team.
By the time the patient was reviewed by the oculoplastics team in 2010, her right upper eyelid ptosis had persisted for 1.5 years. Measurements of the palpebral aperture (PA) of her right and left eye were 6 mm and 8 mm, respectively. Measurements of marginal reflex distance 1 (MRD1) for her right and left eyes were 0.5 mm and 2 mm, respectively. Levator palpebrae function was 8 mm for the right eye and 14 mm for the left eye. Lid creases measured 7 mm and 5 mm for the right and left eye, respectively.
Eventually, the patient underwent a surgical correction of her ptosis with levator muscle advancement in August 2011. Surgery was uncomplicated and postoperative recovery was uneventful. Seven months after the operation, her PA measured 9 mm and 8 mm while MRD1 measured 4 mm and 3 mm for the right and left eye, respectively.
The pre- and postoperative clinical photos of her eyelids are shown in and , respectively. Preoperatively, she had clinically significant right ptosis obscuring her visual axis, and right lagophthalmos with orbicularis oculi muscle weakness.
Figure 1 Preoperative clinical photo of patient’s eyelids.
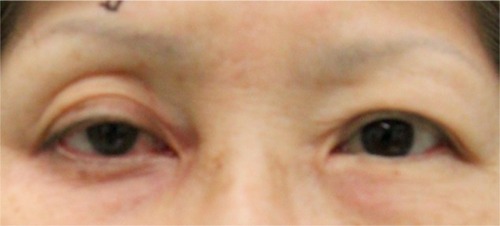
Figure 2 Postoperative clinical photo of patient’s eyelids.

Discussion
Topical bimatoprost is highly efficacious and superior to many other anti-glaucoma eye drops.Citation2,Citation3 However, it commonly causes side effects such as ocular hyperemia, periocular and iris pigmentary changes, although these are mostly reversible with cessation of use.Citation4 Periorbital lipodystrophy resulting in periorbital hollowing, eyelid retraction, and enophthalmos from chronic use of bimatoprost has also been well-documented.Citation5–Citation8 Upper eyelid sulcus deepening has been shown to occur significantly more frequently (objectively and subjectively) with bimatoprost use than with other prostaglandin analogs, namely latanoprost, tafluprost, and unoprostone.Citation9 Aihara et al reported an increased incidence of upper eyelid sulcus deepening in patients who were switched from latanoprost to bimatoprost, suggesting that the latter has a more potent effect on periorbital fat tissue.Citation10 The term “prostaglandin-associated periorbitopathy” (PAP) has been coined to describe the constellation of periorbital soft-tissue changes resulting from the use of topical prostaglandin analogs. The clinical features of PAP include upper eyelid ptosis, deepening of the upper eyelid sulcus, involution of dermatochalasis, orbital fat atrophy, mild enophthalmos, flattening of lower eyelid bags, inferior scleral show, and tight orbits.Citation11 These effects can appear after a period of several weeks to several years, and have been reported to be reversible upon cessation of use.Citation11 Most of the anatomical changes in PAP are thought to be caused by orbital fat atrophy, while dehiscence of levator aponeurosis or Müller muscle may account for the upper lid ptosis.Citation11
It has been postulated that upregulation of prostaglandin F2-α results in significant anti-adipogenic effect.Citation12 Prostaglandin F2-α blocks adipogenesis through the activation of mitogen-activated protein kinase, resulting in the inhibitory phosphorylation of peroxisome proliferator-activated receptor-gamma, a nuclear hormone receptor central to adipocyte differentiation.Citation13,Citation14 Topical prostaglandin analogs have been shown to downregulate the expression of peroxisome proliferator-activated receptor-gamma and inhibit the accumulation of intracytoplasmic lipid droplets.Citation15 The reversal of fat atrophy upon cessation of use may be due to removal of this inhibition, allowing adipogenesis to recommence. Imaging of orbits (computed tomography and magnetic resonance imaging) has ruled out orbital pathology in the fellow eye (resulting in pseudo-enophthalmos) and other disease processes such as cicatrizing changes.Citation5,Citation6 Periorbital changes may be underestimated, as they may be subtle or attributed to age-related volume depletion. Bilateral topical use of prostaglandin analog eye drops in glaucoma may lead to equivocal changes in both eyes, which may be less obvious and thus under-reported. However, in Asians, who tend to have greater upper eyelid fullness, unilateral periorbital fat atrophy may result in more obvious disfigurement.Citation16
To date, as far as we are aware, there has been no report of topical bimatoprost use resulting in periorbital muscle atrophy. Our patient developed ptosis after 2 months of topical bimatoprost use. In , it can also be seen that the patient had deepening of her upper eyelid sulcus and dermatochalasis involution. Clinical eyelid measurements clearly showed reduced function of the right upper eyelid, suggesting that the effects of topical bimatoprost may not be limited to periorbital fat. Reduced levator function and ptosis may be masked by the more common eyelid retraction and deepening of the upper eyelid sulcus. Peplinski and Albiani Smith postulated that Müller muscle (smooth muscle) may be directly affected by prostaglandin-mediated pathways, but whether there is a similar effect on levator muscle (striated muscle) remains unknown.Citation17 Other reasons for the induced right ptosis might have been stretching of the eyelid due to initiation of glaucoma-drop usage, disruption of the Whitnall’s suspensory ligament from the relative enophthalmos, or the patient’s previous cataract surgery, even though there was no fixing of patient’s superior rectus during the surgery. Further studies are warranted. In this case, the patient was advised to stop topical bimatoprost and right ptosis correction surgery was performed successfully. In , it can be seen that the upper eyelid sulcus deepening was much reduced, with a marked improvement in the dermatochalasis involution after the surgery. The patient was happy and satisfied that she did not have ptosis anymore.
It may be worthwhile to note that topical bimatoprost used cosmetically can also cause unwanted side effects such as conjunctival hyperemia and IOP reduction.Citation18 Therefore, while considered generally safe when applied superficially to the base of eyelashes, ocular side effects can still occur with risk of instillation onto the eye surface.
Conclusion
Herein, we report an unusual and previously unreported case of upper eyelid ptosis secondary to levator muscle atrophy as a result of the chronic unilateral use of topical bimatoprost. Clinicians and patients should be aware of this, as it may compromise visual field and be potentially disfiguring, especially when used monocularly. Patients using Latisse should similarly be warned, since the cosmetic and ophthalmic preparations are identical. Patients should be carefully monitored upon initiating treatment. Although this side effect may not be completely reversible with discontinuation of medication, this case shows that it may be successfully corrected with surgical intervention. However, its exact mechanism of action needs to be clarified further.
Disclosure
The authors declare no conflicts of interest in this work. This report received no funding/support.
References
- WirtaDVandenburghAMWengEWhitcupSMKurstjensSBedding-fieldFC3rdLong-term safety evaluation of bimatoprost ophthalmic solution 0.03%: a pooled analysis of six double-masked, randomized, active-controlled clinical trialsClin Ophthalmol2011575976521691584
- LeeAJMcCluskeyPClinical utility and differential effects of prostaglandin analogs in the management of raised intraocular pressure and ocular hypertensionClin Ophthalmol2010474176420689791
- WhitcupSMCantorLBVanDenburghAMChenKA randomised, double masked, multicentre clinical trial comparing bimatoprost and timolol for the treatment of glaucoma and ocular hypertensionBr J Ophthalmol2003871576212488264
- DoshiMEdwardDPOsmanovicSClinical course of bimatoprost-induced periocular skin changes in CaucasiansOphthalmology2006113111961196716935336
- FilippopoulosTPaulaJSTorunNHattonMPPasqualeLRGrosskreutzCLPeriorbital changes associated with topical bimatoprostOphthal Plast Reconstr Surg2008244302307
- JayaprakasamAGhazi-NouriSPeriorbital fat atrophy – an unfamiliar side effect of prostaglandin analoguesOrbit201029635735921158579
- SiraMVerityDHMalhotraRTopical bimatoprost 0.03% and iatrogenic eyelid and orbital lipodystrophyAesthet Surg J201232782282422942109
- NomaKKakizakiHBilateral upper eyelid retraction caused by topical bimatoprost therapyOphthal Plast Reconstr Surg2012282e33e35
- InoueKShiokawaMWakakuraMTomitaGDeepening of the upper eyelid sulcus caused by 5 types of prostaglandin analogsJ Glaucoma201322862663122936280
- AiharaMShiratoSSakataRIncidence of deepening of the upper eyelid sulcus after switching from latanoprost to bimatoprostJpn J Ophthalmol201155660060421953485
- PasqualeLRProstaglandin-associated periorbitopathy: a postmarketing surveillance observationGlaucoma Today20119515258 Available from: http://bmctoday.net/glaucomatoday/pdfs/gt0611_thera_pasquale.pdfAccessed November 29, 2013
- MillerCWCasimirDANtambiJMThe mechanism of inhibition of 3T3-L1 preadipocyte differentiation by prostaglandin F2alphaEndocrinology199613712564156508940395
- LepakNMSerreroGProstaglandin F2 alpha stimulates transforming growth factor-alpha expression in adipocyte precursorsEndocrinoology1995136832223229
- ReginatoMJKrakowSLBaileySTLazarMAProstaglandins promote and block adipogenesis through opposing effects on peroxisome proliferator-activated receptor gammaJ Biol Chem19982734185518589442016
- ChoiHYLeeJELeeJWParkHJJungJHIn vitro study of antiadipogenic profile of latanoprost, travoprost, bimatoprost, and tafluprost in human orbital preadipocytesJ Ocul Pharmacol Ther201228214615222107041
- KikkawaDOKimJWAsian blepharoplastyInt Ophthalmol Clin19973731932049279651
- PeplinskiLSAlbiani SmithKDeepening of lid sulcus from topical bimatoprost therapyOptom Vis Sci200481857457715300114
- WoodwardJAHaggertyCJStinnettSSWilliamsZYBimatoprost 0.03% for cosmetic eyelash growth and enhancementJ Cosmet Dermatol2010929610220618554