
Abstract
Background
This study evaluated the effect of intravitreal injection of bevacizumab (IVB) on macular edema associated with diabetic retinopathy (DME) or branch retinal vein occlusion (BRVOME) using laser speckle flowgraphy.
Methods
A comparative interventional study of 25 eyes from 22 patients with macular edema (DME group: 12 eyes; BRVOME group: 13 eyes) who underwent IVB. Mean blur rate (MBR) was measured in the retinal artery, retinal vein, optic nerve head (ONH), and choroid before and after IVB.
Results
In the BRVOME group, there was no significant change in MBR in the retinal artery, retinal vein or ONH, but choroidal MBR decreased significantly (P=0.04). In the DME group, the MBR in the retinal artery, retinal vein, ONH, and choroid decreased significantly (P=0.02, P=0.04, P<0.001, and P=0.04, respectively). In the DME group, pre-IVB MBR in the ONH was significantly correlated with post-IVB foveal thickness (R= −0.71, P=0.002). There was no such correlation in the BRVOME group in the ONH.
Conclusion
IVB had a suppressive effect on circulation in eyes with DME but not in those with BRVOME. This suggests that this noninvasive and objective biomarker may be a useful part of pre-IVB evaluations and decision-making in DME.
Introduction
Macular edema is one of the main causes of reduced vision in various retinal diseases, including diabetic retinopathy (DR) and branch retinal vein occlusion (BRVO).Citation1–Citation4 This condition is difficult to treat successfully, even for experienced ophthalmologists. Currently, intravitreal injection of bevacizumab (IVB), an anti-vascular endothelial growth factor (VEGF) antibody, is one of the most accepted treatments.Citation5–Citation8 It can improve vision by temporarily blocking VEGF action and subsequently reducing macular edema. However, in cases of DR- or BRVO-associated macular edema (DME and BRVOME, respectively), the effect of IVB is often insufficient, requiring the treatment to be repeated many times.Citation8–Citation11 It is not known why the effectiveness of the treatment is poor in these cases, as the underlying mechanism of IVB’s ability to reduce macular edema is still not well understood. Furthermore, the effect of IVB on retinal circulation is also unknown, although there are a few reports that IVB causes a decrease in intraocular and systemic circulation.Citation12,Citation13 Particularly, IVB can adversely affect the visual prognosis of patients with central retinal vein occlusion and underlying systemic diseases such as diabetes, or ischemic heart or cerebrovascular diseases.Citation14,Citation15
Ischemic change after any medical intervention is ordinarily evaluated with fluorescein angiography, but this technique is invasive, can cause severe complications, including anaphylactic shock, and its results can be affected by time-dependent changes after injection. Recent innovations in an alternative technique, laser speckle flowgraphy (LSFG), have allowed us to quickly and easily monitor changes in tissue circulation over time.Citation16,Citation17 The main measurement parameter of LSFG, mean blur rate (MBR), is an automatically calculated index of ocular blood flow derived from the scatter pattern produced when the ocular fundus is irradiated with laser light. MBR represents the velocity of the blurring in the speckle pattern that is caused by blood flow. Measured values of MBR correlate well with absolute blood flow values measured with the hydrogen gas clearance and microsphere methods.Citation18,Citation19 Previous reports have shown that despite being a relative value, MBR can be considered an accurate representation of both ocular blood flow and velocity.Citation20,Citation21 The quality of LSFG measurements mainly relies on the clarity of the ocular media, but LSFG has already contributed to many recent findings in glaucoma research, and is especially useful in examining the relationship between glaucoma and ocular circulation.Citation16,Citation22–Citation25
In this study, we hypothesized that IVB had a different effect on ocular blood circulation in DME and BRVOME. We evaluated the association between MBR and clinical findings in post-IVB eyes in order to reveal the different pathogenesis of DME and BRVOME, and to find new biomarkers of post-IVB visual prognosis. Thus, our purpose was to evaluate the effect of IVB in DME and BRVOME patients by examining the association of MBR and clinical findings related to the structure and function of the retina.
Materials and methods
Setting and design
This was an institutional, prospective, nonrandomized, interventional case series. Subjects were recruited from patients referred to the Retina Service of Tohoku University Hospital. Intravitreal intervention and follow-up were both performed at this clinic.
Patients
The study comprised 25 eyes of 22 patients (eleven men and eleven women, mean age: 67.5 years) with retinal disease (DR group: 12 eyes of nine patients with DR; BRVO group: 13 eyes of 13 patients with BRVO) and macular edema.
Each patient provided informed consent for their participation in this study as well as for the treatments they received. The study was approved by the institutional review board of Tohoku University Graduate School of Medicine (Protocol No 2013-164; May 17, 2013). The research was conducted according to the provisions of the Declaration of Helsinki, 1995 (as revised in Edinburgh, 2000).Citation26,Citation27
Intervention
In all eyes, after instillation of topical anesthetic (0.4% oxybuprocaine hydrochloride; Benoxil), sterilization of the eyelid (10% povidone-iodine Swabstick), and instillation of 1.25% povidone-iodine (Isodine), 1.25 mg/0.05 mL of bevacizumab (Avastin) was injected into the vitreous cavity with a standard pars plana approach (3.5 mm posterior to the limbus) using a 30-gauge needle.
Measurement of clinical findings
We measured best-corrected visual acuity (BCVA) before, 1 week after, and 1 month after IVB. Similarly, we measured foveal thickness (FT) before, 1 week after, and 1 month after IVB. BCVA was measured with a logMAR chart (5 m) (LVC-10; NEITZ Instruments, Tokyo, Japan), and retinal thickness was measured with optical coherence tomography (OCT) (OCT3000; Carl Zeiss Meditec AG, Jena, Germany). The retinal thickness of the central fovea was defined as the distance between the inner limiting membrane and the retinal pigment epithelium, and was automatically calculated by the OCT3000 software. A macular thickness map was made with the OCT retinal mapping program from six radial scans intersecting at the fovea. The mean retinal thickness was calculated in nine regions: the 1,000 μm central area and the four quadrants of the inner and outer rings. FT was defined as the value of the 1,000 μm central area. Blood pressure and intraocular pressure (IOP) were measured after 10 minutes of rest.
Measurement using laser speckle flowgraphy
We measured MBR with the LSFG NAVI system (Softcare Co., Ltd., Fukutsu, Japan) before, 1 week after, and 1 month after IVB. The measurement conditions were kept constant as follows: angle of view, 21°; number of pixels measured, 750×360; and laser power, 1.37 mW Determination of MBR was made with LSFG Analyzer software (version 3.0.47.0; Softcare Co., Fukutsu, Japan). We measured four regions: a selected retinal artery, a selected retinal vein, the optic nerve head (ONH), and the choroid. Measurements for the retinal artery and the retinal vein were taken from sites near the ONH (within 1.5 papilla diameters). In patients with BRVOME, blood vessels in the quadrant containing the obstruction were not selected in order to avoid the influence of the hemorrhage. The mean number of samples was 1,013, 1,482.3, and 47,785.2 in the retinal artery, the retinal vein, and the ONH, respectively. Measurement of the choroid was performed in a square area (150×150 pixels; 19,479 samples) not containing retinal blood vessels, in a temporal location located one papilla diameter away from the ONH. Only a single measurement of each region was performed.
Statistical analysis
Analysis was done with Ekuseru-Toukei 2006 software (Social Survey Research Information Co., Ltd., Tokyo, Japan). The data are presented as mean ± standard deviation. The significance of the difference between pre- and post-IVB data was assessed with the Friedman test and Scheffe’s paired comparison. We also used the Mann–Whitney U test to compare characteristics other than sex and optic media and clinical findings before and after IVB in the BRVO and DR groups. Sex and optic media were compared with Fisher’s exact test. The Spearman correlation coefficient was used to determine the relationship between MBR and FT in the ONH. A P-value of less than 0.05 was considered to be statistically significant.
Results
A comparison of characteristics and findings before and after IVB in the BRVOME and DME groups is shown in . Before IVB, there were no significant differences in age, optic media, IOP, or FT between the two groups, but there were significant differences in sex distribution and visual acuity. After IVB, there was no difference in IOP between the two groups, but there was a significant difference in FT. FT in the BRVOME group was significantly lower than in the DME group 1 month post-IVB.
Table 1 Comparison of characteristics and findings before and after intravitreal injection of bevacizumab in groups with branch retinal vein occlusion and diabetic retinopathy
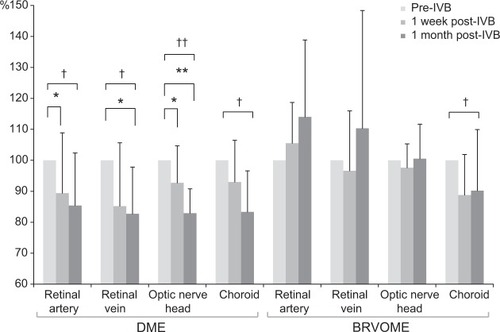
BCVA and FT before and after IVB are shown in and , respectively. MBR in the retinal artery, retinal vein, ONH, and choroid before and after IVB is shown in . In the DME group, MBR changed significantly in all regions 1 week and 1 month after IVB (retinal artery, P=0.02; retinal vein, P=0.04; ONH, P<0.001; and choroid, P=0.04). In the BRVOME group, MBR did not change significantly 1 week or 1 month after IVB in any of the measured regions (retinal artery, P=0.09; retinal vein, P=0.33; ONH, P=0.50), except the choroid (P=0.04).
Figure 1 Best-corrected visual acuity before and after intravitreal injection of bevacizumab.
Abbreviations: BCVA, best-corrected visual acuity; BRVOME, branch retinal vein occlusion-associated macular edema; DME, diabetic macular edema; IVB, intravitreal bevacizumab; logMAR, logarithm of the minimum angle resolution.
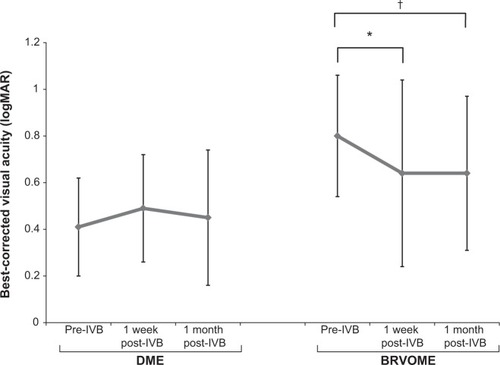
Figure 2 Foveal thickness before and after intravitreal injection of bevacizumab.
Abbreviations: BRVOME, branch retinal vein occlusion-associated macular edema; DME, diabetic macular edema; FT, foveal thickness; IVB, intravitreal bevacizumab.
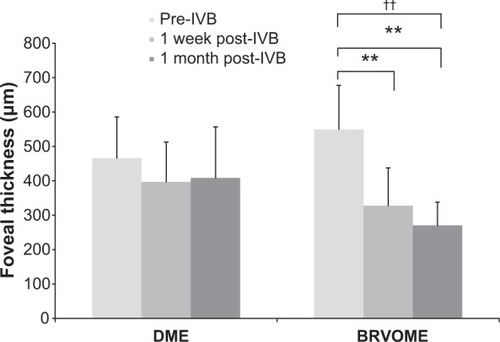
Figure 3 Mean blur rate in the retinal artery, retinal vein, optic nerve head, and choroid before and after intravitreal injection of bevacizumab.
Abbreviations: BRVOME, branch retinal vein occlusion-associated macular edema; DME, diabetic macular edema; IVB, intravitreal bevacizumab; MBR, mean blur rate; ONH, optic nerve head.
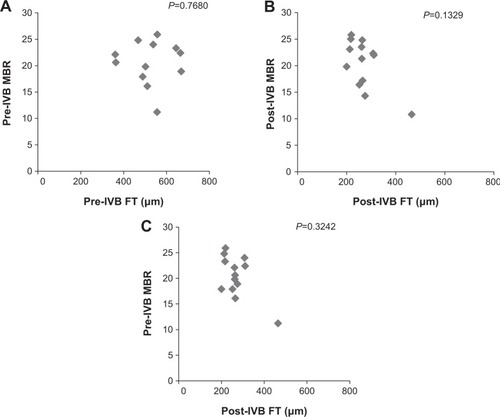
The relationship between FT and MBR in the ONH of the DME group is shown in . Pre-IVB MBR in the ONH was not correlated with pre-IVB FT (P=0.33), but post-IVB MBR in the ONH was correlated with post-IVB FT (R= −0.80, P=0.009). Furthermore, pre-IVB MBR in the ONH was correlated with post-IVB FT (R= −0.71, P=0.002). The relationship between FT and MBR in the ONH of the BRVOME group is shown in . There were no equivalent correlations in the ONH of the BRVOME group.
Figure 4 Relationship between foveal thickness and mean blur rate in eyes with diabetic macular edema.
Abbreviations: FT, foveal thickness; IVB, intravitreal bevacizumab; MBR, mean blur rate.
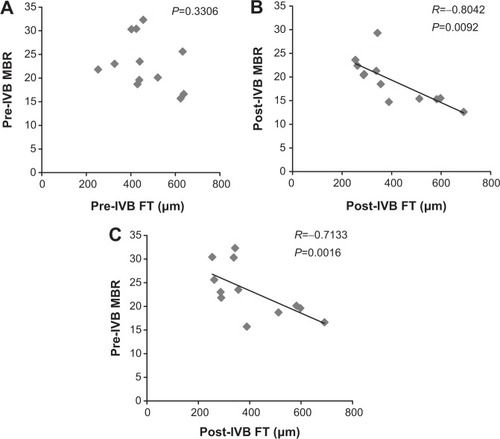
Figure 5 Relationship between foveal thickness and mean blur rate in eyes with branch retinal vein occlusion-associated macular edema.
Abbreviations: FT, foveal thickness; IVB, intravitreal bevacizumab; MBR, mean blur rate.
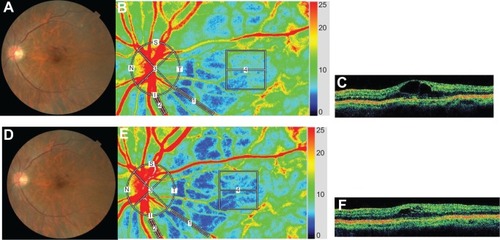
Representative eyes with DME and BRVOME are shown in and , respectively.
Figure 6 Representative eye with diabetic macular edema.
Abbreviations: DME, diabetic macular edema; FT, foveal thickness; IVB, intravitreal bevacizumab; LSFG, laser speckle flowgraphy; MBR, mean blur rate; OCT, optical coherence tomography.
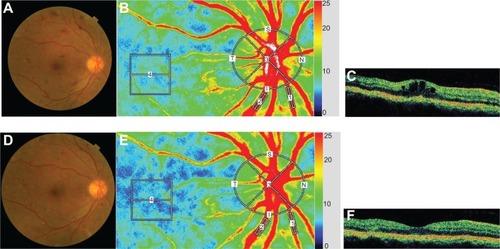
Figure 7 Representative eye with branch retinal vein occlusion-associated macular edema.
Abbreviations: BRVOME, branch retinal vein occlusion-associated macular edema; FT, foveal thickness; IVB, intravitreal bevacizumab; LSFG, laser speckle flowgraphy; MBR, mean blur rate; OCT, optical coherence tomography.
Complications arising from IVB, such as endophthalmitis, ocular hypertension, retinal detachment, and vitreous hemorrhage, did not occur in any of the patients in this study.
Discussion
We set out to investigate the effect of IVB on the retina in DME and BRVOME patients, in particular its effect on ocular blood flow. We found that in BRVOME patients, there was no significant change in MBR in any of the areas measured in this study, with the exception of a significant decrease in the choroid. In the group of patients with DME, there was a significant decrease in MBR in all measured areas. Interestingly, however, we observed that pre-IVB MBR in the DME patients was significantly correlated with post-IVB FT; specifically, higher MBR before IVB was correlated with lower FT after IVB.
There are no reports on the influence of IVB on intraocular microcirculation predating the current study. Our study, in which we analyzed the results of only a single injection, broadly agrees with existing reports showing that IVB leads to a significant improvement in FT and BCVA in patients with BRVOME.Citation5,Citation9 Some earlier papers also found a similar improvement in patients with DME,Citation28–Citation30 but our study contradicts such findings. The exact reason for this discrepancy is unclear, but it may be related to differences in injection times and follow-up periods, pre-IVB BCVA, differences in the demographics of the DME patients, or the small number of participants in this study. One of the most interesting findings of this study, that IVB reduces MBR in all regions of the eye in patients with DME, has not been previously reported. Previous reports on post-IVB ocular circulation used color Doppler imaging (CDI) and found that blood flow decreased after IVB in the ophthalmic artery, the posterior ciliary artery, and the central retinal artery.Citation12,Citation31 These studies were unable to report on blood flow within the eye itself, however, as the intraocular vessels are too small to allow CDI to function. Access to LSFG was therefore a major advantage of this study since it allowed us to directly measure MBR in the retinal vessel, ONH, and choroid and confirm the reduction of ocular blood flow in eyes with DME. We also observed a decrease in choroidal MBR in the BRVOME group, most likely because, as shown in previous reports,Citation32,Citation33 the choroid lacks an autoregulation system and is easily affected by exercise. Our findings for the choroid were based on measurements taken of the MBR in retinal regions lacking large vessels, in accord with established practice for LSFG measurement of the choroid.Citation34
Another interesting finding of our study was that the lack of structural improvement in the DME patients may have been related to the decrease in MBR in the ONH observed before IVB and 1 month after IVB. We observed no such association in the BRVO group. This is an interesting discrepancy that may be related to the pathogenesis of each type of macular edema. However, it should be noted that the characteristics of the two groups in our study did not match perfectly, differing in sex distribution and pre-IVB BCVA. From these results, however, we believe that it is fair to speculate that the effect of bevacizumab on intraocular tissues changes in the presence of systemic diseases such as diabetes. In our study, the eyes with DME probably experienced the effects of excessive VEGF over the entire retina, while the effects were limited to the obstructed retinal vein and its surrounding tissues in the eyes with BRVOME. The eyes with BRVOME even showed an increase in MBR after IVB, particularly in the artery, although we could not confirm the significance of the difference statistically. If such an increase occurs, it is likely to be part of retinal autoregulation, as a compensatory increase in arterial flow rate to maintain retinal circulation. We believe that this is because in eyes with BRVOME, the retinal vessels are less damaged than in eyes with DME. Most studies of DR have noted upregulation of inducible nitric oxide synthase,Citation35,Citation36 with subsequent capillary degeneration, pericyte loss and permeability.Citation37,Citation38 Though the status of ocular blood flow in DR is still the subject of debate,Citation39,Citation40 CDI and laser Doppler flowmetry have revealed that the velocity of blood flow in the ophthalmic artery and choroidal blood flow both decrease in eyes with DR.Citation41,Citation42 We believe that retinal autoregulation may be impaired in patients with DR and, furthermore, that the additional decrease in retinal circulation caused by IVB leads to an acceleration of the original chronic ischemia in eyes with DR, explaining the appearance of macular ischemia after IVB in patients with underlying diseases such as diabetes.Citation14,Citation15 Caution is therefore indicated when administering anti-VEGF antibodies, including bevacizumab, to DR patients. Even in eyes with BRVOME, although IVB can lead to a temporary reduction of the condition, we cannot exclude the possibility that IVB may also cause an adverse reduction in ocular circulation, particularly in the choroid. Thus, follow-up care in patients undergoing IVB should include LSFG examinations of ocular blood circulation, in addition to standard examinations of retinal structure and function.
It is difficult to make a prognosis on the structure and function of eyes with macular edema after IVB, especially for eyes with DME. Several biochemical mechanisms may contribute to the vascular disruptions that characterize DR and DME.Citation43 The pathogenesis of DME is still unclear but is thought to have several clinical aspects, including inflammation, disruption of the capillary barrier, and dysfunction of the retinal pigment epithelium. In our study, pre-IVB MBR in the ONH was significantly correlated with post-IVB FT of eyes with DME, a result indicating that IVB is not effective for patients with DME and low MBR. We believe that MBR of the ONH can be regarded as a clinically reliable preinterventional parameter, and that the predictive value of pre-IVB MBR may prove to be of importance, especially because LSFG measurements of MBR in the ONH have been reported to be highly reproducible.Citation44 In fact, IVB is not always fully effective in reducing DME, and the pathogenesis of DME may include an IVB-sensitive mechanism related to vascular hyperpermeability (elevated MBR) and a non-IVB-sensitive mechanism, possibly related to impairment of the retinal pigment epithelium. Thus, we believe that the pathogenesis of DME may depend not only on VEGF, but also on other mechanisms suppressed by corticosteroids, as intravitreal injection of triamcinolone acetonide showed better results than IVB in reducing DME and improving BCVA.Citation45 There are also reports showing that BRVOME is closely related to intraocular levels of cytokines such as macrophage inflammatory protein-1β and interleukin-6 but not of VEGF.Citation46,Citation47
Our study was limited by a small sample size, the exclusion of types of macular edema besides BRVOME and DME, the restriction of the data to 1 month after IVB, and by the fact that characteristics were not matched between the two groups. We were also not able to find more than a weak connection between visual acuity and MBR. Nevertheless, we believe our results show that in eyes with BRVOME, IVB is currently a good choice to aid in recovery of FT and visual acuity, without a concomitant decrease in retinal blood flow, at least until such time as other antibodies are ready for clinical use. Furthermore, we are the first to report that pre-IVB MBR is significantly correlated with post-IVB FT in patients with DME, indicating the possible existence of VEGF- and MBR-dependent DME.
In conclusion, we found that in patients with BRVOME, there was no significant change in MBR in the retinal artery, retinal vein, or ONH. In patients with DME, MBR in all measured areas decreased significantly. Furthermore, pre-IVB MBR was significantly correlated with post-IVB FT in patients with DME, but there was no such correlation in patients with BRVOME. Higher pre-IVB MBR in these patients was an indicator of lower post-IVB FT. Measuring MBR with LSFG, therefore, has the potential to serve as a noninvasive and objective biomarker to help clinicians determine the value of IVB treatments for patients with DME. The focus of further investigation should be a determination of MBR relationship to the mechanism behind IVB-induced reduction of DME and BRVOME.
Author contributions
HK and TN were responsible for the design and conduct of the study. FN, HK, NA, KO, YS, and MY were responsible for the collection, management, analysis, and interpretation of the data. HK and TN were responsible for the preparation, review, and approval of the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
This paper was partially presented at the 27th Annual Meeting of the Japanese Society for Ocular Circulation, Kobe, Japan, 2010. This paper was supported in part by JST grant, JSPS KAKENHI Grant-in-Aid for Scientific Research (B) (T.N. 26293372), for Scientific Research (C) (H.K. 26462629), and for Exploratory Research (T.N. 26670751). The authors report no conflicts of interest in this work.
References
- Argon laser photocoagulation for macular edema in branch vein occlusionThe Branch Vein Occlusion Study GroupAm J Ophthalmol19849832712826383055
- FerrisFL3rdPatzAMacular edema: a major complication of diabetic retinopathyTrans New Orleans Acad Ophthalmol1983313073166623578
- GutmanFAZegarraHMacular edema secondary to occlusion of the retinal veinsSurv Ophthalmol198428Suppl4624706540483
- SigelmanJDiabetic macular edema in juvenile- and adult-onset diabetesAm J Ophthalmol19809032872966158868
- YilmazTCordero-ComaMUse of bevacizumab for macular edema secondary to branch retinal vein occlusion: a systematic reviewGraefes Arch Clin Exp Ophthalmol2012250678779322539192
- KangHMChungEJKimYMKohHJSpectral-domain optical coherence tomography (SD-OCT) patterns and response to intravitreal bevacizumab therapy in macular edema associated with branch retinal vein occlusionGraefes Arch Clin Exp Ophthalmol2013251250150822653439
- ShimuraMYasudaKYasudaMNakazawaTVisual outcome after intravitreal bevacizumab depends on the optical coherence tomographic patterns of patients with diffuse diabetic macular edemaRetina201333474074723222391
- SolaimanKADiabMMDabourSARepeated intravitreal bevacizumab injection with and without macular grid photocoagulation for treatment of diffuse diabetic macular edemaRetina20133381623162923538584
- SiegelRADreznikAMimouniKBorEWeinbergerDBourlaDHIntravitreal bevacizumab treatment for macular edema due to branch retinal vein occlusion in a clinical settingCurr Eye Res201237982382922668201
- HanadaNIijimaHSakuradaYImasawaMRecurrence of macular edema associated with branch retinal vein occlusion after intravitreal bevacizumabJpn J Ophthalmol201256216517422183139
- GulkilikGTaskapiliMKocaboraSMuftuogluGDemirciGIntravitreal bevacizumab for persistent macular edema with proliferative diabetic retinopathyInt Ophthalmol201030669770220936526
- HosseiniHLotfiMEsfahaniMHEffect of intravitreal bevacizumab on retrobulbar blood flow in injected and uninjected fellow eyes of patients with neovascular age-related macular degenerationRetina201232596797122146127
- MatsuyamaKOgataNMatsuokaMWadaMTakahashiKNishimuraTPlasma levels of vascular endothelial growth factor and pigment epithelium-derived factor before and after intravitreal injection of bevacizumabBr J Ophthalmol20109491215121820538658
- ShimuraMYasudaKMacular ischaemia after intravitreal bevacizumab injection in patients with central retinal vein occlusion and a history of diabetes and vascular diseaseBr J Ophthalmol201094338138320215378
- HuangZLLinKHLeeYCSheuMMTsaiRKAcute vision loss after intravitreal injection of bevacizumab (avastin) associated with ocular ischemic syndromeOphthalmologica20102242868919707032
- YoshidaYSugiyamaTUtsunomiyaKOguraYIkedaTA pilot study for the effects of donepezil therapy on cerebral and optic nerve head blood flow, visual field defect in normal-tension glaucomaJ Ocul Pharmacol Ther201026218719220415624
- SugiyamaTKojimaSIshidaOIkedaTChanges in optic nerve head blood flow induced by the combined therapy of latanoprost and beta blockersActa Ophthalmol200987779780019053956
- TakahashiHSugiyamaTTokushigeHComparison of CCD-equipped laser speckle flowgraphy with hydrogen gas clearance method in the measurement of optic nerve head microcirculation in rabbitsExp Eye Res2013108101523262066
- WangLCullGAPiperCBurgoyneCFFortuneBAnterior and posterior optic nerve head blood flow in nonhuman primate experimental glaucoma model measured by laser speckle imaging technique and microsphere methodInvest Ophthalmol Vis Sci201253138303830923169886
- NagaharaMTamakiYAraieMFujiiHReal-time blood velocity measurements in human retinal vein using the laser speckle phenomenonJpn J Ophthalmol199943318619510413252
- NagaharaMTamakiYTomidokoroAAraieMIn vivo measurement of blood velocity in human major retinal vessels using the laser speckle methodInvest Ophthalmol Vis Sci2011521879220702824
- AizawaNKunikataHYokoyamaYNakazawaTCorrelation between optic disc microcirculation in glaucoma measured with laser speckle flowgraphy and fluorescein angiography, and the correlation with mean deviationClin Experiment Ophthalmol201442329329423601712
- YokoyamaYAizawaNChibaNSignificant correlations between optic nerve head microcirculation and visual field defects and nerve fiber layer loss in glaucoma patients with myopic glaucomatous diskClin Ophthalmol201151721172722205831
- ChibaNOmodakaKYokoyamaYAssociation between optic nerve blood flow and objective examinations in glaucoma patients with generalized enlargement disc typeClin Ophthalmol201151549155622125400
- SugiyamaTAraieMRivaCESchmettererLOrgulSUse of laser speckle flowgraphy in ocular blood flow researchActa Ophthalmol201088772372919725814
- FabickMMEthical considerations for research on human subjectsPlast Surg Nurs19951542252272318710975
- EnserinkMBioethics. Helsinki’s new clinical rules: fewer placebos, more disclosureScience2000290549141841911183748
- ForteRCennamoGLFinelliMIntravitreal bevacizumab vs intravitreal triamcinolone combined with macular laser grid for diffuse diabetic macular oedemaEye (Lond)20102481325133020300127
- ArevaloJFSanchezJGWuLPan-American Collaborative Retina Study GroupPrimary intravitreal bevacizumab for diffuse diabetic macular edema: the Pan-American Collaborative Retina Study Group at 24 monthsOphthalmology20091168148814971497.e119545900
- PaccolaLCostaRAFolgosaMSBarbosaJCScottIUJorgeRIntravitreal triamcinolone versus bevacizumab for treatment of refractory diabetic macular oedema (IBEME study)Br J Ophthalmol2008921768017965109
- BonninPPournarasJALazrakZUltrasound assessment of short-term ocular vascular effects of intravitreal injection of bevacizumab (Avastin®) in neovascular age-related macular degenerationActa Ophthalmol201088664164519563370
- OkunoTSugiyamaTKohyamaMKojimaSOkuHIkedaTOcular blood flow changes after dynamic exercise in humansEye (Lond)200620779680016021186
- ShigaYShimuraMAsanoTTsudaSYokoyamaYAizawaNOmodakaKThe influence of posture change on ocular blood flow in normal subjects, measured by laser speckle flowgraphyCurr Eye Res201338669169823654357
- IsonoHKishiSKimuraYHagiwaraNKonishiNFujiiHObservation of choroidal circulation using index of erythrocytic velocityArch Ophthalmol2003121222523112583789
- CarmoACunha-VazJGCarvalhoAPLopesMCNitric oxide synthase activity in retinas from non-insulin-dependent diabetic Goto-Kakizaki rats: correlation with blood-retinal barrier permeabilityNitric Oxide20004659059611139367
- Abu El-AsrarAMDesmetSMeersschaertADralandsLMissottenLGeboesKExpression of the inducible isoform of nitric oxide synthase in the retinas of human subjects with diabetes mellitusAm J Ophthalmol2001132455155611589878
- ZhengLDuYMillerCCritical role of inducible nitric oxide synthase in degeneration of retinal capillaries in mice with streptozotocin-induced diabetesDiabetologia20075091987199617583794
- LealECManivannanAHosoyaKInducible nitric oxide synthase isoform is a key mediator of leukostasis and blood-retinal barrier breakdown in diabetic retinopathyInvest Ophthalmol Vis Sci200748115257526517962481
- GrunwaldJEBruckerAJGrunwaldSERivaCERetinal hemodynamics in proliferative diabetic retinopathy. A laser Doppler velocimetry studyInvest Ophthalmol Vis Sci199334166718425842
- PatelVRassamSNewsomRWiekJKohnerERetinal blood flow in diabetic retinopathyBMJ199230568556786831393111
- GracnerTOcular blood flow velocity determined by color Doppler imaging in diabetic retinopathyOphthalmologica2004218423724215258411
- NagaokaTKitayaNSugawaraRAlteration of choroidal circulation in the foveal region in patients with type 2 diabetesBr J Ophthalmol20048881060106315258025
- CiullaTAAmadorAGZinmanBDiabetic retinopathy and diabetic macular edema: pathophysiology, screening, and novel therapiesDiabetes Care20032692653266412941734
- AizawaNYokoyamaYChibaNReproducibility of retinal circulation measurements obtained using laser speckle flowgraphy-NAVI in patients with glaucomaClin Ophthalmol201151171117621887100
- ShimuraMNakazawaTYasudaKComparative therapy evaluation of intravitreal bevacizumab and triamcinolone acetonide on persistent diffuse diabetic macular edemaAm J Ophthalmol2008145585486118328456
- ShimuraMNakazawaTYasudaKKunikataHShionoTNishidaKVisual prognosis and vitreous cytokine levels after arteriovenous sheathotomy in branch retinal vein occlusion associated with macular oedemaActa Ophthalmol200886437738418039346
- KunikataHShimuraMNakazawaTChemokines in aqueous humour before and after intravitreal triamcinolone acetonide in eyes with macular oedema associated with branch retinal vein occlusionActa Ophthalmol201290216216720456252