
Abstract
Background
As a method of treatment for a dropped lens nucleus, which occurred during cataract surgery, the dropped lens nucleus was removed through the corneal wound without using pars plana vitrectomy (PPV). After vitrectomy, the dropped lens nucleus was floated on the perfluorocarbon liquid (PFCL). The floating lens nucleus was then phacoemulsified and aspirated. During surgery, irrigation from the anterior chamber was performed. This method was very effective for treatment of a dropped hard nucleus.
Case report
During cataract surgery on the left eye of an 80-year-old woman, a posterior capsule rupture occurred. As a result, the lens nucleus dropped into the vitreous cavity. Irrigation to the anterior chamber was performed, with an anterior chamber maintainer inserted through a newly created side port at the corneal limbus. A vitreous cutter and a light guide were inserted in order to perform vitrectomy through the corneal incisions that were created for the cataract surgery. After vitrectomy, the dropped lens nucleus was floated using PFCL. The floating lens nucleus was removed by a bimanual phacoemulsification technique, with the anterior chamber irrigation continuing. The separation of the irrigation port and the aspiration port allowed for effective treatment of the dropped nucleus that was floating on the PFCL, even using a phacoemulsification machine with a peristaltic pump system. Safe and effective vitrectomy, similar to a PPV, could be performed with this method using three corneal ports.
Conclusion
This technique may allow safer and more effective treatment for a dropped lens nucleus compared with conventional PPV. With this technique, corneal distortion due to surgical manipulation can lead to reduced visibility of the posterior eye.
Introduction
If the posterior capsule ruptures during cataract surgery, the lens nucleus may drop into the vitreous cavity. To retrieve a dropped lens nucleus, pars planar vitrectomy (PPV) is usually performed.Citation1,Citation2 For treatment in the vitreous cavity, a vitreous cutter is often used, along with a fragmatome if the nucleus is hard.
A decade has passed since 25 G transconjunctival microincisional vitreous surgery (MIVS) was first reported in 2002,Citation3 and the use of MIVS has since expanded in Japan.
Therefore, MIVS is now being performed in cases of a dropped lens nucleus that may occur as a complication of cataract surgery.Citation4 However, problems may occur when trying to retrieve a dropped lens using a technique similar to the conventional 20 G PPV. A new scleral incision and trocar placement are necessary in PPV by MIVS. In many facilities, because a fragmatome is 20 G for, for a hard lens nucleus, the dropped lens nucleus is floated on perfluorocarbon liquid (PFCL) and phacoemulsification is often performed as a treatment.Citation5,Citation6
This case report demonstrates favorable results that were obtained using transcorneal vitrectomy and anterior chamber irrigation for a patient with dislocation of the lens nucleus into the vitreous cavity during cataract surgery.
Case report
The patient was an 80-year-old woman with a progressive cataract in the left eye (Emery–Little classification: grade 4 nucleus). In the left eye, the corrected distance visual acuity (CDVA) was +1.6 logMAR and corneal astigmatism was −1.75 D. The preoperative number of corneal endothelial cells was 2,571 cells/mm2 in the right eye and 2,653 cells/mm2 in the left eye. The patient’s past medical history was unremarkable.
During cataract surgery for the left eye, posterior capsule rupture occurred. As a result, part of the lens nucleus dropped into the vitreous cavity. Anterior vitrectomy and removal of residual cortex from the lens capsule for lens dislocation with posterior capsule rupture were performed by two-way divided irrigation and aspiration using a corneal side port.
Transcorneal vitrectomy
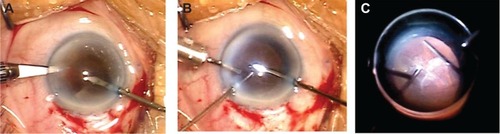
Irrigation to the anterior chamber was then performed with an anterior chamber (23 G) maintainer inserted through a newly created side port at the corneal limbus (). A vitreous cutter (23 G) and light guide (23 G) were inserted to perform vitrectomy through the corneal incisions created for cataract surgery ().
Figure 1 Transcorneal vitrectomy.
Phacoemulsification of dropped lens floated on PFCL
After vitrectomy, the dropped lens nucleus was floated on PFCL (). The floating lens nucleus was removed using a bimanual phacoemulsification technique while anterior chamber irrigation continued (). Due to the convex shape of the PFCL interface (), the lens fragment was unable to be visualized below the iris. However, it was able to be located by changing the direction of the infusion port and the fluid stream into the eye ().
Figure 2 Phacoemulsification of dropped lens floated on perfluorocarbon liquid (PFCL).
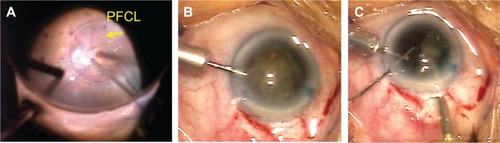
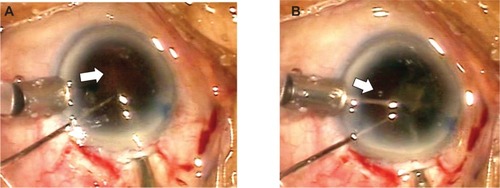
Figure 3 Phacoemulsification of the dropped lens floated on perfluorocarbon liquid (PFCL). The direction of the infusion is indicated by the arrows.
The PFCL was removed, peripheral vitrectomy with scleral depression was performed, and the lens cortex entangled in the peripheral vitreous was removed. The intraocular lens was secured in the ciliary sulcus and the wound was closed. Mydriasis was maintained throughout the surgery.
Postoperative course
At 1 month postoperative, the CDVA was +0.3 logMAR with −2.75 –2.25 D ×120 and the intraocular pressure (IOP) was 14 mmHg. At 2 months postoperative, the CDVA was +0.1 logMAR with −2.00 –2.00 D ×120 and the IOP was 14 mmHg. Further, the cornea was maintained as compared with preoperative, with a corneal endothelial cell number of 2,604/mm2 and corneal astigmatism of −1.75 D.
Discussion
MIVS with 23 G and 25 G vitrectomy systems is increasingly being performed for vitreoretinal diseases. If a lens nuclear fragment drops into the vitreous cavity due to posterior capsule rupture as a complication of cataract surgery, MIVS can be performed to retrieve the fragment.Citation4 To retrieve a dropped nuclear fragment by PPV with MIVS, a new scleral incision and trocar placement are necessary. However, when a cataract surgery incision is enlarged to treat posterior capsule rupture, trocar placement may be difficult due to ocular hypotension or incision leakage during trocar/cannula insertion. In addition, vitreous incarceration in the scleral incision can lead to postoperative complications. Wang et alCitation7 reported insertion of a 20 G vitreous cutter and light pipe through the corneal layer to remove a dropped lens nuclear fragment in the vitreous cavity, as a complication of cataract surgery. They reported that when the dropped nuclear fragment comprises less than half of the lens, even if the lens is hard, it can be crushed with a light pipe and vitreous cutter. Nakasato et alCitation8 reported on a method of removing dislocated nuclear fragments, smaller than one-quarter of the size of the lens nucleus, through the sclerocorneal incision made for the cataract surgery. An anterior vitreous cutter with a 27 G chandelier endoilluminator tied to its sleeve was inserted into the eye through the incision made for cataract surgery and used for core vitrectomy. A fragmatome with another 27 G chandelier endoilluminator fiber was used to grasp and move the larger dislocated nuclear fragments into the anterior chamber, where they were divided and removed.
When a nuclear fragment with grade 4 hardness (Emery– Little classification) drops into the vitreous cavity, removal using a 25 G vitreous cutter alone is difficult. In 20 G vitrectomy, a 20 G fragmatome can be inserted into the vitreous cavity through a scleral incision, and the nucleus in the vitreous cavity can be removed using ultrasound.Citation1,Citation2 However, fragmatomes that can be inserted from 23 G and 25 G cannulas are not yet widely available. Removing the nuclear fragments in the vitreous cavity by ultrasound, is thus not always possible. Therefore, to retrieve a hard nuclear fragment, PFCL must be injected into the vitreous cavity after vitrectomy, the nuclear fragment floated up to the iris, and the nuclear fragment on the PFCL removed using a phacoemulsification handpiece.
The shape of the interface between the PFCL and aqueous is convex, so nuclear fragments floated on the PFCL may be hidden by the iris. Because the space above the PFCL is wider compared with the lens capsule, freedom of movement of nuclear fragments is greater than with phacoemulsification in the capsule. This makes collection on the phacoemulsification of the tip more difficult. By creating a fluid stream with irrigation and aspiration, nuclear fragments can be efficiently collected on the phacoemulsification of the tip. The fluid stream can be changed by divided irrigation and aspiration (bimanual phacoemulsification).Citation9 By changing the fluid stream, nuclear fragments hidden by the iris can be identified.
Implementing vitreous treatment from the corneal incision, with transcorneal vitrectomy, vitreous incarceration into the corneal incision can easily be recognized, and port problems can be prevented.Citation7 The incision is the same for cataract surgery or anterior vitrectomy, so surgical invasiveness can be reduced. If an incision is enlarged when a lens dislocation occurs, the IOP cannot be maintained and a trocar puncture may be difficult. The procedure reported in this case study does not require a trocar and is effective in cases of lens dislocation. If a vitreous cutter and light pipe are compressed by a floating lens and irrigating hand-held lens system, corneal distortion can lead to reduced visibility.
Conclusion
In conclusion, transcorneal vitrectomy and bimanual phacoemulsification are useful for a dropped lens floated on PFCL, when the nucleus is hard and cannot be treated using a vitreous cutter.
Disclosure
The authors report no conflicts of interest in this work.
References
- RofaghaSBhisitkulRBManagement of retained lens fragments in complicated cataract surgeryCurr Opin Ophthalmol201122213714021191293
- HoLYDoftBHWangLBunkerCHClinical predictors and outcomes of pars plana vitrectomy for retained lens material after cataract extractionAm J Ophthalmol2009147458759419195636
- FujiiGYDe JuanEJrHumayunMSA new 25-gauge instrument system for transconjunctival sutureless vitrectomy surgeryOphthalmology2002109101807181212359598
- BakerPSSpirnMJChiangA23-Gauge transconjunctival pars plana vitrectomy for removal of retained lens fragmentsAm J Ophthalmol2011152462462721726843
- JangHDLeeSJParkJMPhacoemulsification with perfluorocarbon liquid using a 23-gauge transconjunctival sutureless vitrectomy for the management of dislocated crystalline lensesGraefes Arch Clin Exp Ophthalmol201325151267127223052719
- LeeSJKimIGParkJMManagement of posteriorly dislocated crystalline lens with perfluorocarbon liquid and fibrin glue-assisted scleral-fixated intraocular lens implantationJ Cataract Refract Surg201339333433823506917
- WangZYZhaoKLiJKBiswalMZhaoPQImmediate corneal vitrectomy for posteriorly dislocated lens fragments during cataract surgeryRetina20133381715171923807182
- NakasatoHUemotoRKawagoeTOkadaEMizukiNImmediate removal of posteriorly dislocated lens fragments through sclerocorneal incision during cataract surgeryBr J Ophthalmol20129681058106222504837
- TsuneokaHShibaTTakahashiYFeasibility of ultrasound cataract surgery with a 1.4 mm incisionJ Cataract Refract Surg200127693494011408144