
Abstract
Purpose
To report novel application of topographically-customized collagen crosslinking aiming to achieve hyperopic refractive changes. Two approaches were evaluated, one based on epithelium-off and one based on epithelium-on (transepithelial).
Methods
A peripheral annular-shaped topographically customizable design was employed for high-fluence ultraviolet (UV)-A irradiation aiming to achieve hyperopic refractive changes. A total of ten eyes were involved in this study. In group-A (five eyes), a customizable ring pattern was employed to debride the epithelium by excimer laser ablation, while in group-B (also five eyes), the epithelium remained intact. In both groups, specially formulated riboflavin solutions were applied. Visual acuity, cornea clarity, keratometry, topography, and pachymetry with a multitude of modalities, as well as endothelial cell counts were evaluated.
Results
One year postoperatively, the following changes have been noted: in group-A, average uncorrected distance visual acuity changed from 20/63 to 20/40. A mean hyperopic refractive increase of +0.75 D was achieved. There was some mild reduction in the epithelial thickness. In group-B, average uncorrected distance visual acuity changed from 20/70 to 20/50. A mean hyperopic refractive increase of +0.85 D was achieved. Epithelial thickness returned to slightly reduced levels (compared to baseline) in group-A, whereas to slightly increased levels in group-B.
Conclusion
We introduce herein the novel application of a topographically-customizable collagen crosslinking to achieve a hyperopic refractive effect. This novel technique may be applied either with epithelial removal, offering a more stable result or with a non-ablative and non-incisional approach, offering a minimally invasive alternative.
Introduction
Over the past decade, corneal collagen crosslinking (CXL) has become routine for stabilizing corneal ectasia,Citation1,Citation2 as well as in the management of corneal infections.Citation3–Citation5 Laboratory data suggest that the CXL application, consisting of riboflavin injection and ultraviolet (UV)-A irradiation, increases stromal collagen fibril diameter resulting in improved corneal biomechanical strength.Citation6 Several clinical reports indicate that this corneal stiffening results not only in arresting ectasia progression,Citation7,Citation8 but also in reduction of corneal keratometry,Citation9–Citation11 perceived as central corneal flattening.Citation12–Citation15 We have reported on the use of prophylactic, higher fluence CXL as an agent for refractive stabilization in high-myopic and hyperopic LASIK,Citation16–Citation18 and have also recently reported significant refractive changes in astigmatic keratotomy, when “flash” CXL was implemented on the incision margins.Citation19
We present herein a custom application with a novel device, enabling the topographically-customizable administration of very high-fluence CXL, applied in a specifically designed peripheral annular pattern, in order to achieve predictable corneal steepening, rather than flattening, aiming to induce a hyperopic-correction refractive change.
Materials and methods
This study received approval by the Laservision.gr Clinical and Research Eye Institute, Research Ethics Committee, Athens, Greece, and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained by the volunteer subjects at the time of the first study visit.
Patient enrollment
A total of ten eyes were involved in this study. In group-A (five eyes), a customizable ring pattern was employed to debride the epithelium employing excimer laser ablation, while in group-B (also five eyes), the epithelium remained intact.
All eyes involved in the study had not undergone any previous ocular surgery, and did not have any significant (judged by a complete ophthalmological examination) present irritation or abnormality, save for the slight refractive error (hyperopia).
Surgical technique
The patients in the two groups were randomly assigned to be subjected to a different mode of epithelial management and riboflavin instillation, whereas the mode of UV-A administration was identical. Only one eye per patient was subjected to the respective procedure. Specifically, group-A involved customized annular peripheral excimer-laser epithelium debridement for a depth of 50 μm (laser-debridement epithelial removal [PTK]),Citation20 facilitated by the EX500 excimer (Alcon Laboratories, Inc., Fort Worth, TX, USA), restricted between the annular zone defined by an inner diameter of 6 mm and an outer diameter of 9 mm. In group-B, the epithelium remained intact (transepithelial crosslinking).
Because of the different epithelial management, the two groups were subjected to different riboflavin instillation procedures. In group-A, following epithelial removal, riboflavin was applied topically. The Vibex Rapid (Avedro Inc., Waltham, MA, USA), a 0.10%, very slightly hypotonic solution mixed with hydroxypropyl methylcellulose, a replacement for Dextran, aiming not to dehydrate the cornea, was applied every 30 seconds for a total of 10 minutes.
In group-B, the riboflavin penetration through the intact epithelium into the stroma involved a two-step process. In an attempt to increase the effective bioavailability of riboflavin within the anterior stroma with administration through the epithelium we employed as a first step we gently scrubbed the cornea surface with a sterile cotton tip after instillation of one drop of 0.5% proparacaine solution (Alcaine; Alcon, Fort Worth, TX, USA). This step was employed in order to thin the tear layers and especially the mucin layer and potentially “weaken” the superficial epithelial layer and facilitate riboflavin solution penetration. As a second step, slightly hypotonic specially-formulated 0.25% riboflavin solution with 0.02% benzalkonium (ParaCel; Avedro Waltham, MA, USA). This solution is acting as an epithelial “abrasive” agent that improves transfer of the large riboflavin molecule through the basal epithelial hemidesmosomes, this was applied every 30 seconds (four drops total) for a 2 minute duration. The time limitation is due to manufacturer caution against administering ParaCel for over 4 minutes to minimize the risk of epithelial sloughing.
The third step was application of a 0.22% riboflavin isotonic saline solution (VibeX Xtra, Avedro). The choice of this solution was based on our experience with using the standard riboflavin concentration (0.1%) in this step not being as effective. Application time was 6 minutes, with a drop every 30 seconds. With this two-step riboflavin soaking process, the passage to the anterior chamber was achieved in approximately 10 minutes.
In all cases the KXL II (Avedro), a CE (Conformité Européenne)-marked device, was employed for the topographically custom designed annular pattern of UV-A exposure (device illustrated in ). Following alignment and focusing, the pupillary aperture was captured and tracked by the KXL II internal tracking mechanism. As shown in , the specific annular irradiation pattern had a “doughnut” shape, centered on the pupil, extending from 6 mm to 9 mm, with total energy of 12.0 J/cm2 applied for 13 minutes and 20 seconds. The time duration of CXL application was calculated based on the energy that was planned to be delivered, the fluence and the pulsing rate. UV-A power was 30 mW/cm2, delivered with a pulsed mode of 1 second on and 1 second off. During the UV-A irradiation the cornea was moistened every couple of minutes with a drop of balanced salt solution. All patients were postoperatively treated with a combination of antibiotic/corticosteroid drops for 10 days.
Figure 1 The KXL II device (Avedro Inc., Waltham, MA, USA) shown with the customizable annular pattern designed in the main control screen and the steerable ultraviolet-A head unit with the built-in tracker camera image.

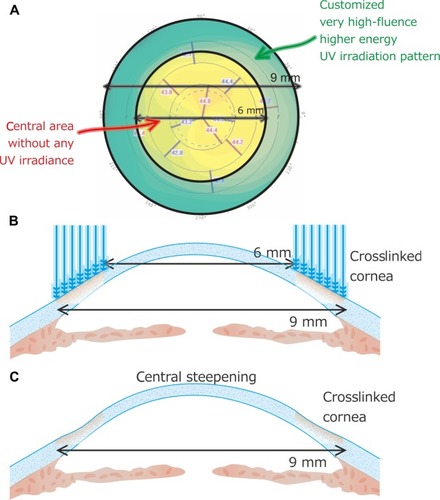
Figure 2 Customized profile employed in the hyperopic treatment.
The patients were examined the first day, the first week, and every month up to 1 year. To evaluate intra- and postoperative pain, we employed a qualitative scale as follows: from no noticeable pain (Grade 0) to severe, consistent pain (Grade 10). During each visit, the cornea was assessed with slit-lamp examination, Placido topography (Topolyzer Vario, WaveLight, Erlangen, Germany) providing curvature maps and simulated keratometry, Scheimpflug imaging (Oculyzer II, WaveLight) providing curvature maps and simulated keratometry, anterior surface irregularity indices and keratoconus classification, autorefraction and keratometry (Nidek AR 1, Nidek Co., Ltd., Tokyo, Japan), anterior-segment optical coherence tomography (OCT)Citation21 (RtVue-100, Optovue Inc., Fremont, CA, USA) providing corneal pachymetry and epithelial pachymetry maps, and endothelial cell counts measurement employing confocal specular microscopy (CellChek XL, Konan Inc., Irvine, CA, USA). Epithelial thickness was monitored qualitatively by means of slit-lamp examination and quantitatively by the anterior-segment OCT device.
Results
The following preoperative average data pertain to the two groups of study: in group-A, the patients (two male and three female) were on average 70±14 (58 to 85) years of age at the time of their operation. Best spectacle corrected distance visual acuity (CDVA) was 20/40, uncorrected distance visual acuity (UDVA) 20/63, average manifest refractive spherical equivalent (MRSE) +2.00±1.00 (+1.00 to +2.75) D, central corneal thickness was 535 μm and minimum corneal thickness 525 μm. The patients in group-B (three male and two female) were on average 68±14 (47 to 82) years of age. Average preoperative values were CDVA 20/32, UDVA 20/70, MRSE +1.75±1.00 (+0.75 to +2.50) D, central corneal thickness 552 μm and minimum corneal thickness 538 μm. These data are also reported in .
Table 1 Average preoperative and 1 year postoperative pachymetry (central corneal thickness and central epithelial thickness, units μm) and keratometry (steep and flat axis simulated K within the 3 mm radius, units D) for the two groups
In regard to operation time, in group-A, the entire operation was completed on average in less than 15 minutes, while in group-B, in 25 minutes. In group-A, the patients reported slight intraoperative pain (average 3.2 on the 0–10 scale), whereas in group-B, patients reported no pain (average 0.5 on the 0–10 scale) and minimal discomfort during the procedure. During the immediate postoperative follow-up visits, the patients also reported no pain. Cornea clarity was not affected, and no postoperative haze or epithelial complications were noted in any treated cornea. In group-A re-epithelialization was completed in an average of 3–4 days.
In both groups endothelial cell counts were stable, from 2,430 cells/mm2 average preoperative to 2,400 6 months postoperatively in group-A, and 1,930 to 1,900 cells/mm2 in group-B, respectively.
One year postoperatively, average UDVA was improved in both groups to 20/40 group-A, and to 20/50 in group-B. Average MRSE was +1.20±1.00 (+0.20 to +1.75) D in group-A and +0.95±1.00 (+0.25 to +1.50) D in group-B. Of the five patients involved in group-A, four gained one Snellen line, while one had no gain. In group-B, three gained one Snellen line, while two had no gain. No patient lost any Snellen line.
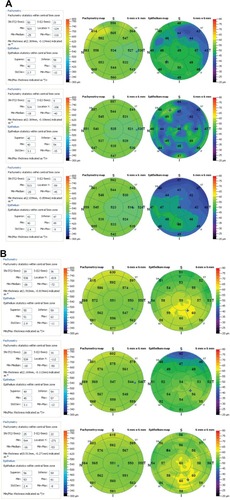
and illustrate examples of Placido disc and Scheimpflug imaging sagittal curvature preoperative, 6 months postoperative, as well as difference maps. In group-A, a noted central hyperopic correction (ie, central keratometric steepening) was noted (on average +0.75 D, reaching up to +2.5 D locally in some cases) as measured by all keratometric modalities employed in the study. In group-B, the central hyperopic correction (keratometric steepening) was on average +0.85 D, reaching up to +1.5 locally in some cases. illustrates examples of OCT-derived corneal and epithelial thickness pachymetry maps preoperatively, 1 month and 6 months postoperatively.
Figure 3 Placido disk topography sagittal curvature maps (diameter 9 mm) depicting hyperopic refractive changes.
Abbreviation: PTK, laser-debridement epithelial removal.
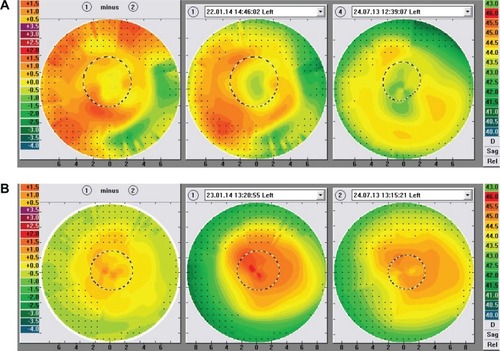
Figure 4 Scheimpflug imaging data showing comparison of 6 months postoperative data (A) versus preoperative (B), as well as the difference A–B (C), indicating the hyperopic refractive changes.
Abbreviation: PTK, laser-debridement epithelial removal.
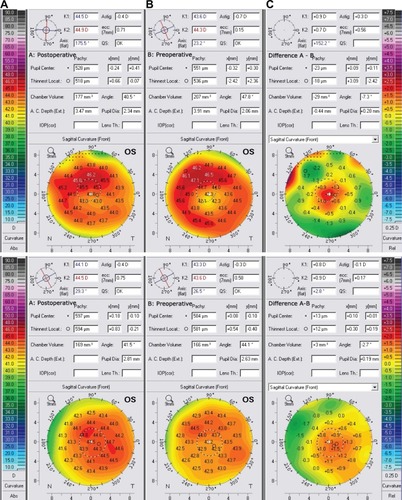
Figure 5 Anterior-segment OCT imaging pachymetry maps for cornea (left) and corneal epithelium (right) covering the center 6 mm diameter area.
Abbreviations: OCT, optical coherence tomography; PTK, laser-debridement epithelial removal.
Discussion
The significant refractive changes induced by the classic CXL,Citation9,Citation10,Citation12–Citation14,Citation22,Citation23 when applying the Dresden protocol (3 mW/cm2 for 30 minutes), as well as higher UV-A fluence,Citation24 and even with riboflavin placed within a femtosecond laser-created pocket or Intrastromal Corneal Ring Segments channels can be established by a number of reports.Citation25,Citation26 We have theorized that this central flattening constitutes a refractive effect resulting from differential crosslinking-induced stiffening effects.
Facilitated by the development of a customizable differential UV delivery system by Avedro and the ability to perform feasibility studies with the KXL II device (Avedro), the current study provides additional evidence for the potential of custom-designed, selected pattern application CXL in the deliberate treatment of refractive error. We have reported previously topographically central cornea flattening effects consistent with a correction of myopia of about 2.5 DCitation27 with central application of customized CXL. The available interim data appear promising with regard to the potential for correcting low myopic refractive errors without tissue removal in an excimer-like fashion or other previously described thermal techniques combined with CXL.Citation28 Such myopic and astigmatic correctionsCitation29 are novel applications that are currently under study with this technology with a procedure called Photorefractive Intrastromal Crosslinking (PiXL).
While customarily, CXL has been applied centrally, the specific annular application demonstrated herein presents a novelty. The peripheral topographically-customized application of crosslinking presented herein was designed to induce a preferential corneal stiffening along the peripheral annulus of 6–9 mm. As shown in , the aim of this stiffening was to induce a corneal steepening (positive) differential within the central 6 mm zone.
Six months postoperatively, a very specific hyperopic correction of +0.8 D (reaching up to +2.5 D at certain loci in group-A, and up to +1.5 D in group-B) was observed ( and and ). These results were stable up until the 1 year examination, too. The fact that these refractive changes were achieved in cases involving relatively elderly patients, and the known “natural” increase of cornea rigidity with age,Citation30 may be suggestive of the increased potential of this application in a younger population.
The corneal thickness epithelial remodeling maps, when compared to normal eyes,Citation31 suggest that there was some modest change in the epithelial distribution. In group-A, the cornea was slightly thinner (average 532 μm from 535 μm preoperatively in group-A and 544 μm from 552 μm preoperatively in group-B). The epithelial thickness remodeling suggested a slightly different progression. Specifically, in group-A (PTK), the epithelium was reduced postoperatively (eg, central epithelial reduction −3.5 μm), while in group-B (transepithelial), the opposite occurred (eg, central epithelial average increase 1.7 μm). These epithelial data, as illustrated in , suggest that the keratometric hyperopic correction (central keratometric steepening) observed in group-A is not masked by epithelial hyperplasia, whereas it is possible that at least part of the observed steepening in group-B may be attributed to epithelial thickness increase. In addition, the epithelial stabilization and even slight thickness reduction in group-A may be suggestive of an increased epithelial stiffening achieved, as reported previously.Citation32 Along the same lines, the epithelial hyperplasia may be an indicator of reduced stiffening in group-B.Citation33
The different observations noted above may be justified by the fact that both applications of UV-A received the same amount of energy. It is known, however, that the epithelial layer contributes to UV-A absorption prior to reaching the stromal lamellaeCitation34 and it is estimated that at least 20%–30%Citation35,Citation36 more energy is required to compensate for this absorption.
Among the relative differences noted between the two methods compared in this work, the intact epithelial procedure (group-B) may be advantageous in the fact that the transepithelial procedure was relatively simple for the patients and surgeon. Because it is essentially performed through the intact epithelium, the procedure required minimal postoperative adjustment of daily activities by the patient and produced essentially no pain or discomfort even within the first few hours after the procedure. The rapid recovery and relative safety of transepithelial CXL may additionally offer the possibility to titrate the effect through two or more treatments over time as needed.
The applications presented in this work may be applied not only for hyperopia correction, but also for presbyopic correction in emmetropic patients. Longer term investigation with a larger and younger population, and further refinement of the treatment patterns, diameter, and centration as well as UV-A dosage is required, and is currently under investigation. Currently these cases have reached 1 year maturity. The refractive, pachymetry, and keratometric data stability has been consistent with that recorded at the 6 months up until the 1 year evaluation.
Conclusion
We herein introduce a novel technique based on customized refractive CXL application on previously untreated corneas as a modest, nevertheless predictable hyperopic treatment option. In the 6 month follow-up time evaluated, a noted cornea steepening was achieved. The PTK application appears to offer improved stability over the transepithelial (intact epithelium) application.
Disclosure
AJK receives partial travel aid from Alcon, Allergan, Avedro, and Keramed. GA has no conflicts of interest to disclose.
References
- DuppsWJJrSpecial section on collagen crosslinking: new hope for more advanced ectatic disease?J Cataract Refract Surg20133981131113223889864
- Sinha RoyARochaKMRandlemanJBStultingRDDuppsWJJrInverse computational analysis of in vivo corneal elastic modulus change after collagen crosslinking for keratoconusExp Eye Res20131139210423664859
- TayapadJBViguillaAQReyesJMCollagen cross-linking and corneal infectionsCurr Opin Ophthalmol201324428829023703462
- Arance-GilAGutiérrez-OrtegaARVilla-CollarCNieto-BonaALopes-FerreiraDGonzález-MéijomeJMCorneal cross-linking for Acanthamoeba keratitis in an orthokeratology patient after swimming in contaminated waterCont Lens Anterior Eye201437322422724355444
- KhanYAKashiwabuchiRTMartinsSARiboflavin and ultraviolet light a therapy as an adjuvant treatment for medically refractive Acanthamoeba keratitis: report of 3 casesOphthalmology2011118232433120884060
- LancharesEdel BueyMACristóbalJALavillaLCalvoBBiomechanical property analysis after corneal collagen cross-linking in relation to ultraviolet A irradiation timeGraefes Arch Clin Exp Ophthalmol201124981223122721494876
- ChanESnibsonGRCurrent status of corneal collagen cross-linking for keratoconus: a reviewClin Exp Optom201396215516423414201
- WollensakGCrosslinking treatment of progressive keratoconus: new hopeCurr Opin Ophthalmol200617435636016900027
- GhanemRCSanthiagoMRBertiTNettoMVGhanemVCTopographic, corneal wavefront, and refractive outcomes 2 years after collagen crosslinking for progressive keratoconusCornea2014331434824162747
- AroraRJainPGoyalJLGuptaDComparative Analysis of Refractive and Topographic Changes in Early and Advanced Keratoconic Eyes Undergoing Corneal Collagen CrosslinkingCornea Epub2013822
- Raiskup-WolfFHoyerASpoerlEPillunatLECollagen crosslinking with riboflavin and ultraviolet-A light in keratoconus: long-term resultsJ Cataract Refract Surg200834579680118471635
- HassanZSzalaiEMódisLJrBertaANémethGAssessment of corneal topography indices after collagen crosslinking for keratoconusEur J Ophthalmol201323563564023483510
- TouboulDTrichetEBinderPSPraudDSeguyCColinJComparison of front-surface corneal topography and Bowman membrane specular topography in keratoconusJ Cataract Refract Surg20123861043104922624904
- PiñeroDPAlioJLKlonowskiPToffahaBVectorial astigmatic changes after corneal collagen crosslinking in keratoconic corneas previously treated with intracorneal ring segments: a preliminary studyEur J Ophthalmol201222Suppl 7S69S8022020986
- HafeziFKanellopoulosJWiltfangRSeilerTCorneal collagen crosslinking with riboflavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusisJ Cataract Refract Surg200733122035204018053900
- KanellopoulosAJPamelGJReview of current indications for combined very high fluence collagen cross-linking and laser in situ keratomileusis surgeryIndian J Ophthalmol201361843043223925331
- KanellopoulosAJKahnJTopography-guided hyperopic LASIK with and without high irradiance collagen cross-linking: initial comparative clinical findings in a contralateral eye study of 34 consecutive patientsJ Refract Surg20122811 SupplS837S84023447898
- KanellopoulosAJLong-term safety and efficacy follow-up of prophylactic higher fluence collagen cross-linking in high myopic laser-assisted in situ keratomileusisClin Ophthalmol201261125113022888210
- KanellopoulosAJVery high fluence collagen cross-linking as a refractive enhancement of a regressed previous astigmatic keratotomyJ Refract Surg201329750450523820234
- KapasiMBaathJMintsioulisGJacksonWBBaigKPhototherapeutic keratectomy versus mechanical epithelial removal followed by corneal collagen crosslinking for keratoconusCan J Ophthalmol201247434434722883842
- KanellopoulosAJAsimellisGComparison of high-resolution Scheimpflug and high-frequency ultrasound biomicroscopy to anterior-segment OCT corneal thickness measurementsClin Ophthalmol201372239224724348011
- GreensteinSAFryKLHershPSCorneal topography indices after corneal collagen crosslinking for keratoconus and corneal ectasia: one-year resultsJ Cataract Refract Surg20113771282129021700105
- KanellopoulosAJPost-LASIK ectasiaOphthalmology20071146123017544782
- KanellopoulosAJLong term results of a prospective randomized bilateral eye comparison trial of higher fluence, shorter duration ultraviolet A radiation, and riboflavin collagen cross linking for progressive keratoconusClin Ophthalmol201269710122275813
- KanellopoulosAJCollagen cross-linking in early keratoconus with riboflavin in a femtosecond laser-created pocket: initial clinical resultsJ Refract Surg200925111034103719731884
- AlióJLToffahaBTPiñeroDPKlonowskiPJavaloyJCross-linking in progressive keratoconus using an epithelial debridement or intrastromal pocket technique after previous corneal ring segment implantationJ Refract Surg2011271073774321751766
- KanellopoulosAJNovel Myopic Refractive Correction with Trans-Epithelial, Very High-fluence Collagen Cross-linking applied in a Customized Pattern: Early Clinical Results in a Feasibility StudyClin Ophthalmol2014869770224741289
- KanellopoulosAJLaboratory evaluation of selective in situ refractive cornea collagen shrinkage with continuous wave infrared laser combined with transepithelial collagen cross-linking: a novel refractive procedureClin Ophthalmol2012664565222570545
- KanellopoulosAJDuppsWJSevenIAsimellisGToric Topographically Customized Trans-Epithelial, Pulsed, Very High-fluence, Higher energy and Higher Riboflavin Concentration Collagen Cross-linking in KeratoconusCase Rep Ophthalmol201418517218025076897
- PallikarisIGKymionisGDGinisHSKounisGATsilimbarisMKOcular rigidity in living human eyesInvest Ophthalmol Vis Sci200546240941415671262
- KanellopoulosAJAsimellisGIn vivo three-dimensional corneal epithelium imaging in normal eyes by anterior-segment optical coherence tomography: a clinical reference studyCornea201332111493149824042485
- KanellopoulosAJAslanidesIMAsimellisGCorrelation between epithelial thickness in normal corneas, untreated ectatic corneas, and ectatic corneas previously treated with CXL; is overall epithelial thickness a very early ectasia prognostic factor?Clin Ophthalmol2012678980022701079
- KanellopoulosAJAsimellisGEpithelial remodeling after femtosecond laser-assisted high myopic LASIK: comparison of stand-alone with LASIK combined with prophylactic high-fluence cross-linkingCornea201433546346924622298
- BottósKMSchorPDreyfussJLNaderHBChamonWEffect of corneal epithelium on ultraviolet-A and riboflavin absorptionArq Bras Oftalmol201174534835122183995
- RaiskupFPinelliRSpoerlERiboflavin osmolar modification for transepithelial corneal cross-linkingCurr Eye Res201237323423822335811
- SamarasKO’BrartDPDoutchJHayesSMarshallJMeekKMEffect of epithelial retention and removal on riboflavin absorption in porcine corneasJ Refract Surg200925977177519772262