
Abstract
Purpose
To evaluate the safety and efficacy of switching from dorzolamide 1.0%/timolol maleate 0.5% fixed-combination (DTFC) eye drops to brinzolamide 1.0%/timolol maleate 0.5% fixed-combination (BTFC) eye drops in patients with primary open-angle glaucoma or ocular hypertension.
Methods
A total of 35 eyes of 35 patients with primary open-angle glaucoma or ocular hypertension using DTFC eye drops were included. Participants discontinued DTFC drops and immediately began using BTFC drops. All other eye drops currently being used were continued. Intraocular pressure (IOP) 1 and 3 months after switching medications was compared with baseline IOP. One month after switching medications, participant preference and adherence were evaluated. Adverse reactions were monitored at each study visit.
Results
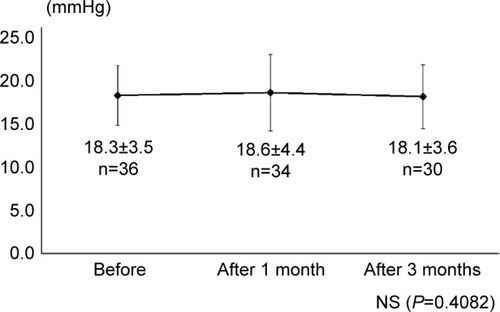
The IOP was 17.9±2.6 mmHg at baseline and 18.3±4.1 mmHg and 17.8±3.4 mmHg 1 month and 3 months after switching medications, respectively (P=0.633). The frequency of missing a dose was not different before (6.1%) and after (6.1%) switching to BTFC. Significantly fewer participants reported stinging after switching to BTFC (15.2%) than while using DTFC (51.5%, P,0.01). Blurred vision was reported with the same frequency before (39.4%) and after (42.4%) switching to BTFC. A total of 33.3% and 27.3% of patients preferred DTFC and BTFC, respectively. Several patients withdrew from the study because of discomfort (n=2, 5.7%), discharge (n=1, 2.9%), dizziness (n=1, 2.9%), or increased IOP (n=2, 5.7%).
Conclusion
Switching from DTFC to BTFC was well tolerated and did not result in IOP changes or a decreased patient adherence. When glaucoma patients complain of stinging with DTFC administration, switching to BTFC is an acceptable treatment option.
Introduction
The ultimate goal of treating glaucoma is to reduce intraocular pressure (IOP) and to preserve the visual field. Initial glaucoma therapies generally consist of prostaglandin analog monotherapy.Citation1,Citation2 However, when inadequate IOP control with a single analog occurs, a different monotherapy agent or an additional medication must be used.Citation3 Multiple medications increase the number of eye drops instilled, which can lead to poor patient adherence. Therefore, a fixed-combination eye drop that contains two different medications is recommended. Several fixed-combination eye drops have been approved for use in Japan and have been available since 2011. These include fixed combinations of a prostaglandin analog and timolol (latanoprost/timolol [Xalacom®, Pfizer, Inc., New York, NY, USA], travoprost/timolol [DuoTrav®, Alcon Laboratories Inc., Fort Worth, TX, USA]) and a fixed combination of a carbonic anhydrase inhibitor and timolol (dorzolamide/timolol [Cosopt®, Merck & Co., Inc., Whitehouse Station, NJ, USA]). In November 2013, a fixed-combination eye drop containing brinzolamide and timolol (Azarga, Alcon Laboratories, Inc.) was approved for use in Japan. This brinzolamide/timolol fixed-combination (BTFC) eye drop was shown to be extremely effective in reducing IOP in Japanese glaucoma patients.Citation4–Citation6 However, dorzolamide/timolol fixed-combination (DTFC) eye drops have been shown to be better for reducing IOP reduction than both latanoprostCitation7 and brimonidine/timolol fixed-combination drops.Citation8 It has been shown that switching patients from a DTFC eye drop to a BTFC eye drop is both safe and effective in reducing IOP,Citation9–Citation11 but this has not been specifically examined in a Japanese population.
Here, we prospectively evaluate IOP reduction, patient comfort, and treatment safety when switching from a DTFC eye drop to a BTFC eyed drop in patients with primary open-angle glaucoma and ocular hypertension. Patients were followed for 3 months following the medication switch.
Materials and methods
A total of 35 eyes of 35 patients (12 men, 23 women) with primary open-angle glaucoma or ocular hypertension who were using DTFC eye drops at Inouye Eye Hospital were enrolled in this study between November 2013 and August 2014. The protocol was approved by the hospital’s ethical committee, and all participants provided written informed consent before any study procedure or examination was performed.
Participants discontinued their twice-daily use of DTFC eye drops (Cosopt®, Merck & Co., Inc.) and immediately switched to a twice-daily use (morning and evening instillation) of BTFC eye drops (Azarga, Alcon Laboratories, Inc.) (twice a day, morning and evening instillation). All other topical medication used remained the same. When participant were using DTFC eye drops in both eyes, the eye with the higher IOP was selected as the study eye. If both eyes had the same IOP, the right eye was selected as the study eye.
The IOP was measured at approximately the same time each visit using a Goldmann tonometer. The magnitude of IOP reduction was defined as the IOP 3 months after switching medication minus the IOP at baseline. One month after switching medications, participant preference and adherence to BTFC therapy use were evaluated (). Participants were also asked about experiencing specific adverse reactions at each study visit. Reasons for participant dropout were also recorded.
Table 1 Questionnaire regarding brinzolamide/timolol fixed-combination eyed drop use
Data analyses
All data are presented as mean ± standard deviation, where applicable. Differences in mean IOP at baseline and at 1 and 3 months were analyzed using paired t-tests. Commercially available statistical software (SPSS, version 22; SPSS, Inc., Chicago, IL, USA) was used to perform all statistical analyses. Statistical significance was defined as P<0.05.
Results
Subject characteristics
Mean subject age at baseline was 67.5±9.0 years (range: 46–84 years). A total of 33 eyes had primary open-angle glaucoma and 2 eyes had ocular hypertension. The number of drops used before switching medications was 3.5±0.6 drops per day, including 19 (54.3%) patients who used 3 drops per day, 14 (40.0%) patients who used 4 drops per day, and 2 (5.7%) patients who used 5 drops per day. The DTFC eye drop counted as 2 drops. Baseline IOP was 17.9±2.6 mmHg (range: 14.0–23.5 mmHg) and Humphrey visual field (30-2 SITA Standard) mean deviation was −8.5±6.5 dB (range: −19.1–1.6 dB).
IOP after switching medications
The IOP 1 and 3 months after switching medications was 18.3±4.1 mmHg (n=33 eyes) and 17.8±3.4 mmHg (n=29 eyes), respectively. These slight differences from baseline (17.9±2.6 mmHg, n=35 eyes) were not statistically significant (P=0.633, ). Three months after switching medication, 10 (34.5%) eyes had a decrease in IOP ≥2 mmHg, 13 (44.8%) eyes had no change in IOP (within 2 mmHg of baseline), and 6 (20.7%) eyes had an increase in IOP ≥2 mmHg.
Figure 1 Intraocular pressure values before and after switching medications.
Abbreviation: NS, not significant.
Subject compliance and comfort
Subject comfort and compliance were evaluated 1 month after switching medications. Two (6.1%) subjects reported missing BTFC drop doses, which was not significantly different than the 2 (6.1%) subjects who missed DTFC drop doses (P=0.999, ).
Table 2 Summary of adverse reactions
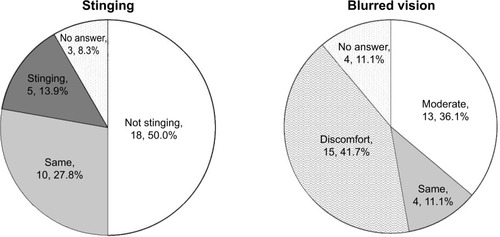
Five (15.2%) subjects reported stinging with BTFC drop use, which was significantly less than the 17 (51.5%) subjects who reported stinging with DTFC drop use (P<0.01). Thirteen (39.4%) subjects reported blurred vision with DTFC drop use, which was not significantly different than the 14 (42.4%) subjects who reported blurred vision with BTFC drop use (P=0.999). summarizes the stinging and blurred vision that subjects experienced during BTFC drop use.
Figure 2 Stinging and blurred vision in subjects using brinzolamide/timolol fixed-combination eye drops.
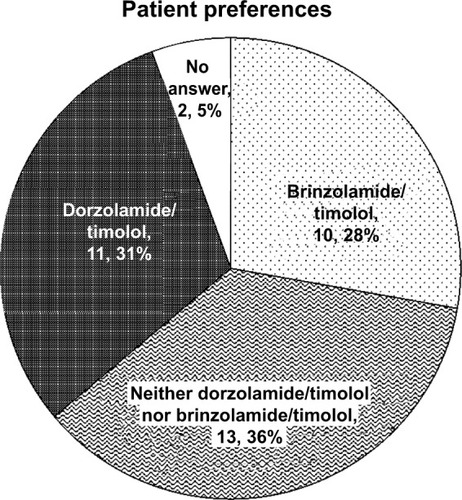
A total of 9 (27.3%) participants preferred to use BTFC drops, 11 (33.3%) participants preferred to use DTFC drops, and 13 (39.4%) participants expressed no preference (). Subjects preferred BTFC drops because they had less stinging (n=5 subjects) and better IOP reduction (n=5 subjects). Subjects preferred DTFC drops because they had less blurred vision (n=7 subjects), less stinging (n=2 subjects), and less discomfort (n=2 subjects).
Figure 3 Patient preferences for each medication examined.
Six (17.1%) participants dropped out of the study before the end of the 3-month study period. Participants withdrew from the study because of increased IOP (n=2 [5.7%] subjects, 1 and 2 months after switching), ocular discomfort (n=2 [5.7%] subjects, ≤1 month after switching), ocular discharge (n=1 [2.9%] subject, 1 month after switching), and dizziness (n=1 [2.9%] subject, 3 days after switching).
Discussion
Several reports on the efficacy of BTFC eye drops in Japanese patients have been published.Citation4–Citation6 Yoshikawa et alCitation4 treated 301 patients with primary open-angle glaucoma or ocular hypertension with timolol for 4 weeks. Patients were then divided into two groups, with one group switched to BTFC drops (150 cases) and the other group continuing on timolol drops (151 cases). Treatment was continued for an additional 8 weeks in both groups. Eight weeks after group differentiation, IOP in the BTFC group was 3.2 mmHg lower (measured 2 hours after drop instillation) than before the switch. Adverse reactions experienced were stinging (5%), blurred vision (1%), and hyperemia (1%). Nagayama et alCitation5 administered timolol therapy to 319 patients with primary open-angle glaucoma or ocular hypertension for 4 weeks. Patients were then divided into two groups, with one group switching to BTFC therapy (158 cases) and the other group switching to brinzolamide and timolol therapy (161 cases). Treatment was continued for an additional 8 weeks in both groups. After 8 weeks, the decrease in IOP was not significantly different between the BTFC group (range: 2.5–3.4 mmHg) and the brinzolamide-added group (range: 2.7–3.3 mmHg). Adverse reactions observed in the BTFC group were punctate keratitis (1%), blurred vision (1%), ocular pruritus (1%), and dysgeusia (1%). Nakajima et alCitation6 administered BTFC eye drops to 126 patients with primary open-angle glaucoma or ocular hypertension for 52 weeks. After the 52-week treatment period, IOP had been reduced between 4.1 mmHg and 5.7 mmHg in each patient. Adverse reactions included, but were not limited to, punctate keratitis (10%), ocular irritation (6%), keratitis (3%), and dysgeusia (3%).
Several studies reporting what happens after switching from DTFC to BTFC therapy have been published.Citation9–Citation11 Lanzl and RaberCitation9 reported what happened after switching from various therapies to BTFC drops. In the 2,937 patients who switched from DTFC drops to BTFC drops, IOP significantly decreased from 18.5±4.1 mmHg to 16.5±3.2 mmHg. Moreover, IOP was significantly lower in 823 patients who switched from a prostaglandin analog plus DTFC drops (18.3±5.0 mmHg) to a prostaglandin analog plus BTFC drops (16.4±3.9 mmHg). Auger et alCitation10 evaluated stinging, blurred vision, eye redness, and abnormal taste in 31 patients who switched from DTFC to BTFC. Patients using DTFC drops experienced more stinging and patients using BTFC drops experienced more blurred vision. There were no differences in eye redness and abnormal taste. Rossi et alCitation11 investigated tear film breakup time, corneal stinging, and glaucoma symptom scale scoreCitation12 in 72 patients switching from DTFC. A significant improvement was reported for all evaluations. Adverse reactions included blurred vision (4.2%) and dysgeusia (2.7%). IOP was not affected by switching medications.
In our study, no patients used DTFC drops concomitantly with an analog. We observed no changes in IOP that resulted from switching to a prostaglandin analog plus BTFC drops (n=18 cases). These results differed from those reported by Lanzl and Raber.Citation9 However, IOP decreased or increased by ≥2 mmHg in 55.2% of subjects. Therefore, we conclude that changes in IOP vary between patients.
Our observed efficacy in reducing IOP was not significantly different from a previous report comparing dorzolamide 2.0%/timolol fixed-combination drops with BTFC drops.Citation13 However, this previous study reported that participants withdrew from the study because of adverse reactions, including discomfort, discharge, and dizziness. In our study, 14.3% and 40% of participants reported stinging and blurred vision, respectively. This was not significantly different than that reported in a previous study (stinging in 42%, blurred vision in 55%).Citation10 Moreover, we observed no severe adverse reactions, which is in agreement with past reports.Citation4–Citation6,Citation9–Citation11,Citation13,Citation14 Also in agreement with past reports,Citation10,Citation13,Citation14 less stinging was reported in the BTFC group than in the DTFC group. We believe that less stinging occurred because of pH differences between medications (dorzolamide/timolol pH =5.6, brinzolamide/timolol pH =7.2). The frequency of blurred vision in the DTFC group was not significantly different from that observed in the BTFC group. This is in agreement with one previous study,Citation13 but two other studiesCitation10,Citation14 found that BTFC drops caused blurred vision more often than DTFC drops. BTFC drops are a liquid suspension, which is known to cause blurred vision. In a previous study, 79.2% of patients preferred BTFC drops over DTFC drops.Citation14 Likewise, Lanzl and RaberCitation9 reported that patients preferred BTFC drop (82.0%) significantly more often than they preferred DTFC drops (8.8%). We found that 33.3% of our participants preferred using DTFC drops and that 27.3% of our participants preferred using BTFC drops. The reason cited for preferring DTFC was less vision blurring. Participants preferred BTFC drops because they caused less stinging. Consequently, we considered the importance of sensation in determining patient preference.
In conclusion, we found no significant difference in IOP, subject compliance, or blurred vision in participants who switched from DTFC drops to BTFC drops. However, stinging was reported more frequently during treatment with DTFC drops. Therefore, in patients who experience stinging with the administration of DTFC drops, switching to BTFC drops is an acceptable glaucoma treatment option.
Disclosure
No author has any conflicts of interest to declare that is relevant to the subject of this article.
References
- Collaborative Normal-Tension Glaucoma Study GroupThe effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucomaAm J Ophthalmol199812644985059780094
- The AGIS InvestigatorsThe Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deteriorationAm J Ophthalmol2000130442944011024415
- DjafariFLeskMRHarasymowyczPJDesjardinsDLachaineJDeterminants of adherence to glaucoma medical therapy in a long-term patient populationJ Glaucoma200918323824319295380
- YoshikawaKKozakiJMaedaHEfficacy and safety of brinzolamide/timolol fixed combination compared with timolol in Japanese patients with open-angle glaucoma or ocular hypertensionClin Ophthalmol2014838939924550667
- NagayamaMNakajimaTOnoJSafety and efficacy of a fixed versus unfixed brinzolamide/timolol combination in Japanese patients with open-angle glaucoma or ocular hypertensionClin Ophthalmol2014821922824531757
- NakajimaMIwasakiNAdachiMPhase III safety and efficacy study of long-term brinzolamide/timolol fixed combination in Japanese patients with open-angle glaucoma or ocular hypertensionClin Ophthalmol2014814915624403818
- QuarantaLMigliorSFlorianiIPizzolanteTKonstasAGEffects of the timolol-dorzolamide fixed combination and latanoprost on circadian diastolic ocular perfusion pressure in glaucomaInvest Ophthalmol Vis Sci200849104226423118502991
- KonstasAGQuarantaLYanDBTwenty-four hour efficacy with the dorzolamide/timolol-fixed combination compared with the brimonidine/timolol-fixed combination in primary open-angle glaucomaEye2012261808721960068
- LanzlIRaberTEfficacy and tolerability of the fixed combination of brinzolamide 1% and timolol 0.5% in daily practiceClin Ophthalmol2011529129821468336
- AugerGARaynorMLongstaffSPatient perspectives when switching from Cosopt® (dorzolamidetimolol) to Azarga™ (brinzolamide-timolol) for glaucoma requiring multiple drug therapyClin Ophthalmol201262059206223271886
- RossiGCPasinettiGMSandoloFBordinMBianchiPEFrom dorzolamide 2%/timolol 0.5% to brinzolamide 1%/timolol 0.5% fixed combination: a 6-month, multicenter, open-label tolerability switch studyExpert Opin Pharmacother201112162425243121679090
- LeeBLGutierrezPGordonMThe glaucoma symptom scale. A brief index of glaucoma-specific symptomsArch Ophthalmol199811678618669682698
- ManniGDenisPChewPThe safety and efficacy of brinzolamide 1%/timolol 0.5% fixed combination versus dorzolamide 2%/timolol 0.5% in patients with open-angle glaucoma or ocular hypertensionJ Glaucoma200918429330019365194
- MundorfTKRauchmanSHWilliamsRDNotivolRBrinzolamide/Timolol Preference Study GroupA patient preference comparison of Azarga™ (brinzolamide/timolol fixed combination) vs Cosopt® (dorzolamide/timolol fixed combination) in patients with open-angle glaucoma or ocular hypertensionClin Ophthalmol20082362362819668763