
Abstract
Purpose
To determine the prevalence of plateau iris in Japanese patients with primary angle closure (PAC) and primary angle closure glaucoma (PACG) and analyze the biometric parameters in patients with plateau iris using ultrasound biomicroscopy (UBM).
Methods
In this cross-sectional observational study, subjects aged >50 years with PAC and PACG who had previously undergone a patent laser peripheral iridotomy underwent UBM in one eye. UBM images were qualitatively analyzed using standardized criteria. Plateau iris in a quadrant was defined by anteriorly directed ciliary body, absent ciliary sulcus, steep iris root from its point of insertion followed by a downward angulation, flat iris plane, and irido-angle contact. At least two quadrants had to fulfill these UBM criteria for an eye to be classified as having plateau iris. A-scan biometry was used to measure anterior segment parameters.
Results
Ninety-one subjects with PAC (58 subjects) or PACG (33 subjects) and 68 normal controls were recruited. The mean (standard deviation) ages of PAC and PACG patients and normal controls were 73.5 (6.2) and 72.6 (7.3), respectively. Based on UBM criteria, plateau iris was found in 16 eyes (17.6%) of 91 eyes. In these 16 eyes, quadrant-wise analysis showed ten eyes (62.5%) had plateau iris in two quadrants; four eyes (25%) had plateau iris in three quadrants; and two eyes (12.5%) had plateau iris in four quadrants. Anterior chamber depth, lens thickness, axial length, lens position, and relative lens position were not statistically significant between the group having plateau iris and that not having plateau iris, respectively.
Conclusion
Approximately 20% of Japanese subjects with PAC and PACG with a patent laser peripheral iridotomy were found to have plateau iris on UBM. No morphological difference was noted in the anterior segment of the eye between those with or without plateau iris.
Introduction
Glaucoma is a major cause of visual loss worldwide, with primary angle closure glaucoma (PACG) representing an important cause of glaucoma blindness.Citation1,Citation2 Many patients with PACG are asymptomatic, and the progression to PACG with glaucomatous optic neuropathy may be rapid. The prevalence of PACG and primary angle closure (PAC) is significantly greater in Asian ethnic groups.Citation1–Citation5 Laser peripheral iridotomy (LPI) is the accepted first-line treatment in the management of eyes with PACG. However, there is a report of Asian eyes with PACG in which LPI alone was not able to prevent a clinically significant rise in intraocular pressure (IOP) from developing in most eyes during follow-up.Citation6 This might be because LPI only relieves pupil block. Recent evidence has shown that non-pupil block mechanisms, such as plateau iris, may play a more important role in the PACG than previously thought.Citation7,Citation8 Irido-angle contact with plateau iris after LPI is thought to be one of the causes for progression of the angle closure disease.Citation9–Citation11 There are some reports that 30% of PAC suspects (PACS) from SingaporeCitation8 and 60% of PACS from the People’s Republic of China were found to have plateau iris configuration.Citation12
Plateau iris has been defined as an occludable angle on gonioscopy, with a flat iris plane and a relatively deeper central anterior chamber depth (ACD). The development of ultrasound biomicroscopy (UBM) has permitted high-resolution images of the anterior segment and has allowed refinement of the definitions of the angle closure mechanisms. A recent study has shown that the anterior chamber associated with plateau iris syndrome is significantly shallower than in normal eyes and those with pupil block alone.Citation13 The shallower anterior chamber in plateau iris may be explained by the fact that the anterior position of the ciliary processes produces an anterior position of lens. However, an anterior lens position (LP) is also the same condition that leads to pupillary block, and it is likely that these two conditions frequently coexist.Citation13
The aim of this study was to determine the prevalence of plateau iris and to compare the anterior segment parameters in having plateau iris and not having plateau iris in Japanese patients with PAC and PACG, and to determine associations between these parameters and angle closure between the two groups.
Methods
This was a prospective study of Japanese subjects with PAC and PACG recruited from Mizoguchi Eye Clinic, Sasebo, Japan and Ozaki Eye Clinic, Miyazaki, Japan, who visited at these two clinics between October 2010 and September 2012. Written informed consent was obtained from all subjects and the study had the approval of the Institutional Review Board of the clinics and was performed in accordance with the tenets of the Declaration of Helsinki.
This cross-sectional study included subjects aged >50 years. PAC was defined as eyes in which the posterior trabecular meshwork was not seen for at least 270° on gonioscopy in the primary position with peripheral anterior synechiae and/or raised IOP (defined as an IOP ≥21 mmHg) but without glaucomatous optic neuropathy or visual field loss. PACG was defined as eyes with PAC associated with glaucomatous optic neuropathy (defined as loss of neuroretinal rim, a vertical cup:disc ratio of 0.7 or an inter-eye asymmetry of 0.2, and/or notching attributable to glaucoma). Patients diagnosed with secondary angle closure (such as neovascular glaucoma or uveitic glaucoma); patients who had corneal abnormalities that would affect imaging, prior history or evidence of acute PAC in the study eye, and previous laser iridoplasty or history of intraocular surgery; and patients on miotic therapy were excluded. All subjects with PAC and PACG had previously undergone LPI.
All subjects underwent a standardized eye examination that included visual acuity measurement, slit-lamp examination (model BQ 900; Haag-Streit, Bern, Switzerland), stereoscopic optic-disc examination with a 78-diopter lens (Volk Optical Inc, Mentor, OH, USA). IOP measurement by Goldmann applanation tonometry (Haar-Streit, Bern, Switzerland), and gonioscopy, were performed in the dark using a Goldmann two-mirror lens at magnification 16×. Indentation gonioscopy with a Sussman four-mirror lens was used to establish the presence or absence of peripheral anterior synechiae. A-scan biometry (model US-800; Nidek Co LTD, Nagoya, Japan) was used to measure axial length (AL), central ACD, and lens thickness (LT). These results were used to calculate LP, defined as ACD +1/2LT, and relative LP (RLP), defined as LP/AL.
UBM
UBM (UD 6000; TOMEY Co., Nagoya, Japan) was performed in dark room conditions. Patients were examined in the supine position, and fixation and accommodation were held constant throughout. Radial scans were performed in the inferior, temporal, superior, and nasal quadrants for one eye. The probe was held perpendicular to the ocular surface, such that the scleral spur and ciliary body and angle were visualized.
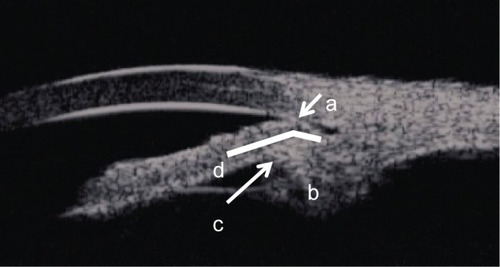
UBM images were graded qualitatively in all four quadrants by a single glaucoma specialist (TM) without clinical information. Based on UBM images, plateau iris was defined in a quadrant if all the following criteria were fulfilled ():Citation7,Citation8
The ciliary process was anteriorly directed, supporting the peripheral iris so that it was parallel to the trabecular meshwork.
The iris root had a steep rise from its point of insertion, followed by a downward angulation from the corneoscleral wall.
Presence of a central flat iris plane.
An absent ciliary sulcus.
Irido-angle contact (above the level of the scleral spur) in the same quadrant.
Figure 1 Ultrasound biomicroscopy image of a quadrant of a primary angle closure glaucoma eye with plateau iris.
At least two quadrants had to fulfill all the above criteria for an eye to be classified as having plateau iris (plateau iris group). No plateau iris group was defined as an eye to be classified as having less than one quadrant.
Statistical analysis
Statistical analysis was performed using SPSS version 15 for Windows (SPSS Inc., Chicago, IL, USA). Differences in mean values of parametric data among eyes of different subjects were examined using independent samples Student’s t-test and Fisher’s exact test. The anterior segment parameters of the plateau iris group, the no-plateau iris group, and the normal controls were compared by a one-way repeated-measures analysis of variance test. A P-value less than 0.05 was considered statistically significant.
Results
A total of 91 Japanese angle closure subjects (consisting of 58 PAC and 33 PACG subjects) and 68 normal controls were recruited. There were significant differences between the two groups for refractive errors (P=0.03), gender (P=0.006), ACD (P<0.0000), LT (P<0.0000), AL (P<0.0000), LP (P<0.0000), and RLP (P=0.005). However, no difference was found for age (P=0.38) ().
Table 1 Comparison of biometric parameters between angle closure and NC groups
On quadrant-wise analysis, 18 of 91 eyes (19.8%) were found to have plateau iris in one quadrant, ten of 91 eyes (11.0%) in two quadrants, four of 91 eyes (4.4%) in three qua drants, and two of 91 eyes (2.2%) in all four quadrants. In 57 of 91 eyes (62.6%), plateau iris was not found in any quadrant (). Plateau iris was found in the superior quadrant in 16 eyes, inferior quadrant in eight eyes, nasal quadrant in 19 eyes, and temporal quadrant in 15 eyes (). Sixteen of 91 (17.6%) eyes fulfilled all the criteria for plateau iris on UBM. There were no cases of plateau iris in the controls.
Table 2 Detection of eyes with plateau iris by ultrasound bio-microscopy
Table 3 Detection of plateau iris in each quadrant by ultrasound biomicroscopy
To determine the effect of plateau iris on the ocular biometrics, we divided the angle closure group into two groups (plateau iris group and no-plateau iris group) and compared them (). No significant differences were noted for age (P=0.60), gender (P=0.93), refractive error (P=0.48), ACD (P=0.41), LT (P=0.15), AL (P=0.75), LP (P=0.81), and RLP (P=0.98). (). The ACDs (mean ± standard deviation) of the plateau iris group, no-plateau iris group, and normal controls were 2.52±0.43 mm, 2.43±0.34 mm, and 3.14±0.34 mm, respectively (analysis of variance; P=8.3×10−4). The ACDs of the plateau iris group and no-plateau iris group were significantly shallower than those of normal controls, respectively (P=0.01). There was no statistically significant difference in the prevalence of plateau iris between PAC and PACG (P=0.91) ().
Table 4 Comparison of biometric parameters between plateau iris group and no-plateau iris group
Table 5 The prevalence of plateau iris between PAC and PACG
Discussion
Mechanisms other than pupil block were suggested to be involved in the pathogenesis of angle closure glaucoma in Japanese patients.Citation14 In this study, using UBM, plateau iris was observed in 17.6% of the Japanese patients with PAC or PACG who had undergone LPI. The frequency of plateau iris in Asian patients with PACG has been reported to be 30% in Singapore,Citation7,Citation8 36.9% in Thailand,Citation7 and 30% in India,Citation15 being about two times higher than in Japan. The prevalence of PACG in Asians has been reported to be 1.0% in Singaporeans,Citation5 1.58% in Indians,Citation16 and 0.9% in Thailand,Citation17 being about two times higher than the 0.6% in Japanese patients.Citation18 This correlation between the prevalence rates of plateau iris and PACG is of interest, and plateau iris is considered to be an important factor in angle closure glaucoma after relieving pupil block in Asians.
Conventionally, plateau iris has been diagnosed on the basis of angle findings in patients who have undergone laser iridotomy as narrowing of the peripheral angle in those with a relatively deep central anterior chamber. However, Kumar et al reported that plateau iris was observed by UBM in about 30% of patients who are PACS or have PACG, and the ACD was shallow in these patients.Citation7,Citation8,Citation15 In this study, involving Japanese patients with PAC or PACG, plateau iris was noted in patients with an ACD significantly shallower than that in the normal controls. Mandell et al reported that a plateau iris group showed an ACD significantly shallower than that of the normal control group and the pupil block group.Citation13 They suggested forward shift of the lens due to anterior displacement of the ciliary body, causing shallowing of the ACD, as a reason for these findings in the plateau iris group. However, an anterior LP is also a condition that leads to pupil block, and it is likely that these conditions frequently coexist. A shallow ACD, thick lens, and short AL have been considered risk factors of angle closure glaucoma.Citation19–Citation21 No significant difference was observed in these parameters between the plateau iris group and no-plateau iris group in this study. Our results contradict the general view that the ACD is normal or deep in patients with plateau iris and the report of Mandell et al.Citation13 According to Mochizuki et alCitation22 plateau iris was noted frequently (34.6%) in Japanese patients with chronic angle closure glaucoma. Surprisingly, it was also noted in 19.2% of those with open angle glaucoma. Yeung et alCitation23 and Sakata et alCitation24 reported that abnormal positioning of the ciliary body was found in normal controls. Thus, eyes with open angle might have also a higher rate of plateau iris than expected in the Japanese patients. This is the reason why there was no statistical difference between the plateau iris group and no-plateau iris group.
Progression from PAC to PACG was reported to occur in approximately 20% of patients who underwent LPI.Citation6 Therefore, PAC does not necessarily progress to PACG, and PAC at high risk for angle closure is considered more likely to develop to PACG. However, no significant difference was noted in the frequency of plateau iris between the PAC and PACG groups in this study. A recent study using anterior segment optical coherence tomography showed that the progression of angle closure is affected by the iris thickness, area, and volume.Citation25,Citation26 Embryologically, the ciliary body and iris root in week 24 of intrauterine life and mature as different organs.Citation27 Therefore, abnormalities occurring in this period may cause morphological abnormalities in both structures. The thickness of the iris root affects the angle width. Therefore, a thicker peripheral iris is likely to contribute to angle closure as the peripheral iris would be in closer proximity to the angle. This may be especially important in eyes with shallow and crowded anterior chambers. Plateau iris and a thick peripheral iris are likely to co-occur, further increasing the risk of angle closure. Continued evaluation involving a larger number of patients is necessary.
This study has several limitations. First, we did not look at the association of the lens parameters with cataract status. Since the ACD has been reported to shallow with cataract progression,Citation28,Citation29 it is important to exclude the effect of cataract when comparing the ACD. However, in our data, there were no significant difference of LT and ACD between the plateau iris group and no-plateau iris group. From this point, we think that the cataract status might have been equal in these two groups. Second, factors such as accommodation and lighting, which may induce changes in lens parameters, were not evaluated. Third, this study was carried out at two separate facilities, and UBM was performed by different investigators. This may have resulted in bias in measurements. Fourth, UBM scan and grading of the images were performed by the same investigator (TM), so the judgments may have been biased.
Conclusion
Plateau iris was observed by UBM in approximately 20% of the Japanese patients who had previously undergone LPI for PAC or PACG and highlight the significance of non-pupil block mechanisms for angle closure in the Japanese angle closure patients. However, no morphological difference was noted in the anterior segment of the eye between those with and without plateau iris.
Disclosure
The authors report no conflicts of interest in this work.
References
- QuigleyHABromanATThe number of people with glaucoma worldwide in 2010 and 2020Br J Ophthalmol20069026226716488940
- FosterPJJohnsonGLGlaucoma in China: how big is the problem?Br J Ophthalmol2001851277128211673287
- BengtssonBThe prevalence of glaucomaBr J Ophthalmol19816546496969603
- HeMFosterPJGeJPrevalence and clinical characteristics of glaucoma in adult Chinese: a population-based study in Liwan District, GuangzhouInvest Ophthalmol Vis Sci2006472782278816799014
- FosterPJOenFTSMachinDThe prevalence of glaucoma in Chinese residents of Singapore: a cross-sectional population survey of the Tanjong Pagar districtArch Ophthalmol20001181105111110922206
- AlsagoffZAungTAngLPChewPTLong-term clinical course of primary angle-closure glaucoma in an Asian populationOphthalmology20001072300230411097612
- KumarRSTantiseviVWongMHPlateau iris in Asian subjects with primary angle closure glaucomaArch Ophthalmol20091271269127219822841
- KumarRSBaskaranMChewPTPrevalence of plateau iris in primary angle closure suspects an ultrasound biomicroscopy studyOphthalmology200811543043417900691
- BhargavaSKLeightonDAPhillipsCIEarly angle-closure glaucoma. Distribution of iridotrabecular contact and response to pilocarpineArch Ophthalmol1973893693724697211
- KunimatsuSTomidokoroAMishimaKPrevalence of appositional angle closure determined by ultrasonic biomicroscopy in eyes with shallow anterior chambersOphthalmology200511240741215745766
- KongXFosterPJHuangQAppositional closure identified by ultrasound biomicroscopy in population-based primary angle-closure glaucoma suspects: the Liwan eye studyInvest Ophthalmol Vis Sci2011523970397521357394
- HeMFriedmanDSGeJLaser peripheral iridotomy in eyes with narrow drainage angles: ultrasound biomicroscopy outcomes. The Liwan Eye StudyOphthalmology20071141513151917462739
- MandellMAPavlinCJWeisbrodDJSimpsonERAnterior chamber depth in plateau iris syndrome and pupillary block as measured by ultrasound biomicroscopyAm J Ophthalmol200313690090314597043
- OzakiMNongpiurMEAungTHeMMizoguchiTIncreased lens vault as a risk factor for angle closure: confirmation in a Japanese populationGraefes Arch Clin Exp Ophthalmol20122501863186822527316
- KumarGBaliSJPandaASobtiADadaTPrevalence of plateau iris configuration in primary angle closure glaucoma using ultrasound biomicroscopy in the Indian populationIndian J Ophthalmol20126017517822569376
- VijayaLGeorgeRArvindHPrevalence of angle-closure disease in a rural southern Indian populationArch Ophthalmol200612440340916534061
- BourneRRSukudomPFosterPJPrevalence of glaucoma in Thailand: a population based survey in Rom Klao District, BangkokBr J Ophthalmol2003871069107412928267
- YamamotoTIwaseAAraieMTajimi Study Group, Japan Glaucoma SocietyThe Tajimi Study report 2: prevalence of primary angle closure and secondary glaucoma in a Japanese populationOphthalmology20051121661166916111758
- AungTNolanWPMachinDAnterior chamber depth and the risk of primary angle closure in 2 East Asian populationsArch Ophthalmol200512352753215824227
- LavanyaRWongTYFriedmanDSDeterminants of angle closure in older SingaporeansArch Ophthalmol200812668669118474780
- WojciechowskiRCongdonNAnningerWTeo BromanAAge, gender, biometry, refractive error, and the anterior chamber angle among Alaskan EskimosOphthalmology200311036537512578783
- MochizukiHTakenakaJSugimotoYTakamatsuMKiuchiYComparison of the prevalence of plateau iris configurations between angle-closure glaucoma and open-angle glaucoma using ultrasound biomicroscopyJ Glaucoma20112031531820577108
- YeungBYNgPWChiuTYPrevalence and mechanism of appositional angle closure in acute primary angle closure after iridotomyClin Experiment Ophthalmol20053347848216181272
- SakataLMSakataKSusannaRJrLong ciliary processes with no ciliary sulcus and appositional angle closure assessed by ultrasound biomicroscopyJ Glaucoma20061537137916988598
- WangBSakataLMFriedmanDSQuantitative iris parameters and association with narrow anglesOphthalmology2010117111719815290
- WangBSNarayanaswamyAAmerasingheNIncreased iris thickness and association with primary angle closure glaucomaBr J Ophthalmol201195465020530187
- ReméCd’EpinaySLPeriods of development of the normal human chamber angleDoc Ophthalmol1981512412687285772
- OkabeITaniguchiTYamamotoTKitazawaYAge-related changes of the anterior chamber widthJ Glaucoma19921100107
- FontanaSTBrubakerRFVolume and depth of the anterior chamber in the normal aging human eyeArch Ophthalmol198098180318087425907