
Abstract
Background
While loteprednol etabonate ophthalmic gel 0.5% (LE gel) is approved for treatment of postoperative ocular inflammation and pain, there have been no reported studies in patients undergoing laser-assisted in situ keratomileusis (LASIK) or photorefractive keratectomy (PRK).
Methods
This was a retrospective chart review conducted at five refractive surgical centers in the USA. Data were collected from primary LASIK or PRK surgery cases in which LE gel was used postoperatively as the clinician’s routine standard of care and in which patients were followed-up for up to 6 months. Data extracted from charts included patient demographics, surgical details, LE gel dosing regimen, pre- and postsurgical refractive characteristics, intraocular pressure (IOP) measurements, and visual acuity. Primary outcomes included postoperative IOP elevations, adverse events, and early discontinuations.
Results
Data were collected on 189 LASIK eyes (96 patients) and 209 PRK eyes (108 patients). Mean (standard deviation [SD]) years of age at surgery was 36.0 (11.7) and 33.9 (11.3) in LASIK and PRK patients. LE gel was prescribed most often four times daily during the first postoperative week, regardless of procedure; the most common treatment duration was 7–14 days in LASIK and ≥30 days in PRK patients. No unusual corneal findings or healing abnormalities were reported. Mean postoperative uncorrected distance visual acuity was 20/24 in LASIK and 20/30 in PRK eyes. Mild/trace corneal haze was reported in 20% of PRK patients; two PRK patients with moderate/severe corneal haze were switched to another corticosteroid. Mean postoperative IOP did not increase over time in either LASIK or PRK eyes (P≥0.331); clinically significant elevations from baseline in IOP (≥10 mmHg) were noted in only three eyes of two PRK patients.
Conclusion
LE gel appears to have a high level of safety and tolerability when used for the management of postoperative pain and inflammation following LASIK and PRK surgery.
Introduction
Refractive surgeries utilizing excimer laser technology are widely used to alter corneal curvature and correct vision.Citation1 Photorefractive keratectomy (PRK) and laser-assisted in situ keratomileusis (LASIK), in particular, have a long track record of safety and efficacy. They have each been performed for more than 20 years and have different advantages and disadvantages. Surface ablation methods such as PRK allow for greater preservation of residual posterior stromal tissue and avoid complications related to flap creation and healing. PRK may also have a lower risk of keratectasia.Citation2,Citation3 However, compared with LASIK, PRK typically has a lengthier and less comfortable recovery process.Citation1,Citation4 Corneal haze formation and infectious keratitis are other possible complications of PRK that can potentially be vision-threatening.Citation5–Citation10
Topical ophthalmic corticosteroids are often utilized for the management of PRK and LASIK patients to minimize postoperative pain and inflammation.Citation1 In PRK, ophthalmic corticosteroids may have an added benefit of minimizing haze formation, a phenomenon that has been demonstrated in clinical studies,Citation11,Citation12 although there exist contrary data suggesting no significant benefit in this regard.Citation13,Citation14 Despite the postoperative benefits of ophthalmic corticosteroids, potential risks associated with their use include intraocular pressure (IOP) elevation, formation of cataracts, infection, and delayed corneal epithelial healing.Citation15
Loteprednol etabonate (LE) is a C-20 ester corticosteroid designed at a molecular level to have an improved therapeutic index over traditional corticosteroids. Due to the replacement of the C-20 ketone group present in all other corticosteroids with a chloromethyl ester group, LE molecules that are not bound to glucocorticoid receptors are quickly de-esterified into inactive metabolites, reducing the potential for unwanted side effects.Citation16–Citation18 The safety and efficacy of LE suspension and ointment formulations have been studied in patients undergoing ocular procedures including cataract surgery,Citation19–Citation21 LASIK,Citation22–Citation25 and PRK.Citation26,Citation27 These and other investigations have confirmed a minimal risk of IOP elevation in patients treated with LE, including individuals who are known steroid responders.Citation28,Citation29
A non-settling gel formulation of LE became available in 2013, which provides consistent, uniform dosing while eliminating the need for shaking prior to administration.Citation30 The gel formulation is thought to provide increased contact time with the ocular surface.Citation30 In addition, the gel formulation has a pH more similar to that of human tears and a 70% lower preservative concentration than the suspension formulation.Citation30 The safety and efficacy of LE ophthalmic gel 0.5% (LE gel) were evaluated in two Phase III randomized vehicle-controlled clinical trials in subjects with postoperative pain and inflammation following cataract surgery.Citation31,Citation32 In these studies, only 0.5% of subjects experienced transient, clinically significant IOP elevations (≥10 mmHg) over baseline during the 2-week treatment period. While LE gel is approved for the treatment of inflammation and pain following ocular surgery, there have been no published studies evaluating the safety of this new formulation in patients undergoing either LASIK or PRK. The purpose of this retrospective study was to assess prescribing behaviors and safety outcomes associated with the use of LE gel for these procedures.
Patients and methods
Study design
This was a medical chart review study conducted at five US refractive surgery sites. Retrospective data were collected on eligible patients at each study site, reflecting the routine care and follow-up of patients who were prescribed LE gel 0.5% in association with LASIK or PRK surgery. The study protocol was approved by the Chesapeake Institutional Review Board (Columbia, MD, USA), which granted a waiver for informed consent given the retrospective nature of the data collection. All subject data were de-identified and kept confidential in accordance with the International Conference on Harmonization Guidelines for Good Clinical Practice.Citation33
Patients aged 18 years or older who had undergone LASIK or PRK surgery prior to March, 2014, and whose perioperative management included LE gel were eligible for inclusion. The surgical procedure must have been the primary surgery, not an enhancement or reoperation. The eligibility cutoff date ensured a minimum time interval of 6 months between surgery and data collection. Reasons for exclusion included use of LE gel for surgical procedures other than LASIK or PRK, and use of ocular steroids other than LE gel for the current LASIK/PRK procedure. Charts of all cases meeting eligibility criteria were identified by personnel at each study site. Information was hand-recorded onto case report forms on-site and then entered electronically into a centralized database.
Data extracted from the medical charts included the following: patient demographics; surgical details; LE gel dosing, frequency, and duration; pre- and postsurgical ocular characteristics including sphere, cylinder, axis, and uncorrected visual acuity (UCVA); pre- and postsurgical IOP measurements; concomitant medications; adverse events (AEs); and early discontinuations. The primary outcomes evaluated included IOP change from baseline, other AEs, any abnormal corneal findings, and early treatment discontinuations.
Data analysis
A minimum sample size of 150 LASIK eyes and 150 PRK eyes was planned. Eyes from patients undergoing bilateral LASIK or PRK were considered separately. IOP findings were evaluated as pre- and postoperative means for the LASIK and PRK groups, separately. A one-way analysis of variance (ANOVA) was used to evaluate any changes in mean IOP by postoperative period (0–30, 31–60, 61–90, and >90 days). The ANOVA was performed using Statistix 10 (Analytical Software, Tallahassee, FL, USA), and a P-value <0.05 was considered significant. Observed increases of IOP ≥10 mmHg over baseline, considered clinically significant, and observed increases of IOP ≥5 mmHg over baseline, considered clinically relevant, were summarized categorically. All other outcomes were analyzed descriptively.
Results
Data were collected on 189 LASIK eyes (96 patients) and 209 PRK eyes (108 patients) from five clinical sites. The LASIK group had a higher female representation and was slightly older on average compared with the PRK group (). Mean (± standard deviation [SD]) baseline IOP was 15.5 (2.2) mmHg in LASIK eyes and 14.6 (2.7) mmHg in PRK eyes. All IOP measurements were performed using applanation tonometry. Other preoperative ocular measurements and UCVA findings are presented in . Baseline UCVA appeared slightly worse in the PRK eyes compared with the LASIK eyes.
Table 1 Demographic characteristics and preoperative IOP of surgical groups
Table 2 Pre- and postoperativeTable Footnote* ocular characteristics
In the LASIK group, 81 (42.9%) of flaps were created with a femtosecond laser, and 106 (56.1%) with a microkeratome; flap technique was not recorded for two (1.1%) eyes. Mean (SD) calculated/intended flap thickness in the LASIK group was 112.5 (44.5) µm. Mean (SD) ablation depth was 59.1 (30.5) µm in the LASIK group and 65.8 (32.7) µm in the PRK group. Per PRK standard operating procedures, all surgeons applied mitomycin C 0.2%–0.25% either as a drop to the ablation area or a soaked cellulose sponge applied to the central corneal surface, either immediately following ablation or at the conclusion of the procedure for a minimum of 10 seconds to a maximum of 25 seconds depending on surgeon preference.
Treatment regimens
Preoperative application of LE gel was noted in ten (5.3%) LASIK eyes and 24 (11.5%) PRK eyes. Administration of LE gel in postoperative recovery and throughout the balance of the day of surgery was more commonly reported with LASIK than PRK (). There were no instances noted of LE gel being applied intraoperatively to the stromal bed or directly to the flap following closure during LASIK procedures, or before or immediately following placement of a bandage contact lens in PRK procedures.
Table 3 LE gel administration on day of surgery
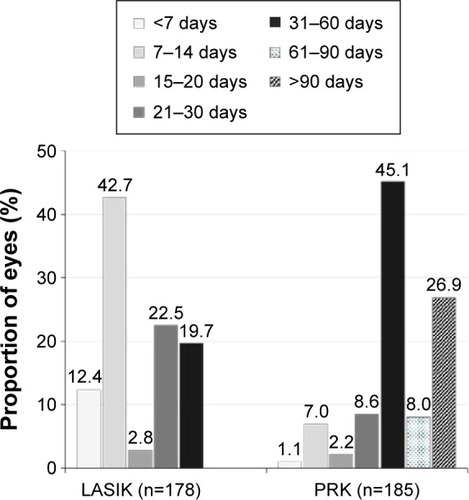
During the first postoperative week, LE gel was prescribed most frequently as one drop QID (four times daily), regardless of type of surgery (). The most common duration of postoperative LE gel therapy was 7–14 days for LASIK cases and 30 days or longer in PRK cases (). Duration of LE gel therapy was 60 days or shorter in all LASIK cases. Among PRK cases, more than one-third (34.9%) of eyes were treated with LE gel longer than 60 days, and 26.9% of eyes were treated with LE gel for more than 90 days. Standard operating procedures at each study site typically dictated a tapering of LE gel dosing frequency beyond the first week of treatment.
Figure 1 LE gel dosing frequency during first postoperative week.
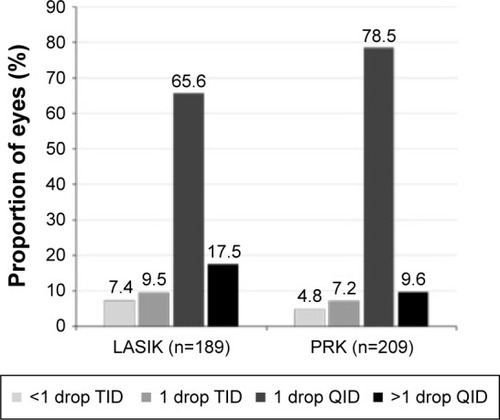
Figure 2 Postoperative duration of LE gel treatment.
Postoperatively, the most frequently reported concomitant antibacterials in the LASIK group were moxifloxacin 0.5% (53.1% of patients) and besifloxacin 0.6% (39.6%), and in the PRK group, moxifloxacin 0.5% (56.5%) and gatifloxacin 0.5% (31.5%). The most common non-corticosteroid anti-inflammatory agents used postoperatively were cyclosporine A 0.05% (42.7%) post-LASIK and bromfenac 0.09% or 0.07% (36.1%) post-PRK. All patients were prescribed lubricants/artificial tear products postoperatively.
Surgical outcomes and safety findings
summarizes pre- and postoperative outcomes. Mean (SD) postoperative sphere and cylinder were −0.04 (0.49) and −0.28 (0.45) diopters in LASIK eyes and −0.09 (0.77) and −0.50 (0.45) diopters in PRK eyes. Mean postoperative UCVA was 20/24 in LASIK eyes and 20/30 in PRK eyes.
There were no reports of abnormal corneal morphology, corneal edema, wound healing/integrity, infection, or reports of corneal infiltrates or any unexpected findings noted in the charts including flap dislocation (LASIK). Among PRK cases, corneal haze was noted in 40 (19.1%) eyes in 22 (20%) patients postoperatively. These were all characterized as “mild” or “trace” (or simply recorded as “yes”) with the following exceptions (three eyes in two patients): corneal haze was characterized as “severe” in both eyes of a 21-year-old female patient treated with LE gel, one drop QID, and which led to LE gel treatment discontinuation. Briefly, the procedure involved chemical alcohol epithelial removal with a resulting epithelial wound size of 8.5 mm. No haze was reported for this patient on postoperative day 4 when the bandage contact lens (BCL) was removed. However, trace corneal haze was reported in both eyes on postoperative day 13, progressing to moderate corneal haze on day 48, and severe corneal haze on day 83 and day 118. On the day 118 visit, therapy was switched from LE gel to prednisolone 1% one drop QID. The haze failed to resolve and additional treatment was planned including topical mitomycin C. The second case, also performed using chemical alcohol epithelial removal, occurred in a 32-year-old male patient treated postoperatively with LE gel, one drop QID, who was first noted to have trace corneal haze in one eye on postoperative day 20 and moderate corneal haze on day 41. Topical steroid therapy was switched to difluprednate, but no further follow-up was available. Both these patients (as well as all other PRK cases) were treated with mitomycin C during the primary keratorefractive procedure. No other patients were noted to have stopped LE gel prematurely or switched to a different topical corticosteroid.
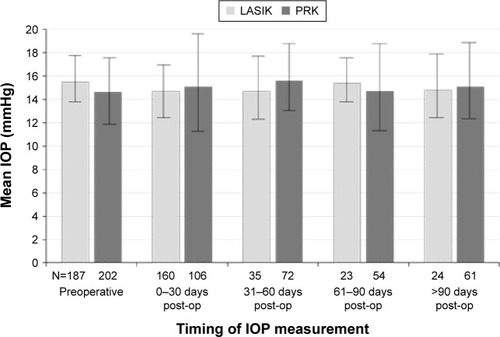
shows the mean (± SD) preoperative and postoperative IOP over time in LASIK and PRK eyes. Postoperative IOP measurements ranged from 9 to 21 mmHg in LASIK eyes and from 7 to 29 mmHg in PRK eyes. Postoperative mean IOP did not increase over time in either LASIK eyes (F=1.17, P=0.3311) or PRK eyes (F=0.98, P=0.407). As indicated earlier, LASIK patients received postoperative LE gel therapy most often for 7–14 days, whereas PRK patients received postoperative LE gel therapy most often for 31–60 days. Mean (SD) IOP over these time frames was 14.68 (2.28) mmHg and 15.60 (2.91) mmHg for LASIK and PRK patients, respectively, ranging from 9 to 21 mmHg in LASIK eyes and 10 to 23 mmHg in PRK eyes.
Figure 3 Mean (SD) IOP measurements over time.
Abbreviations: IOP, intraocular pressure; LASIK, laser-assisted in situ keratomileusis; post-op, postoperative; PRK, photorefractive keratectomy; SD, standard deviation.
shows IOP elevations ≥5 mmHg above baseline and ≥10 mmHg above baseline. Clinically significant elevations from baseline in IOP (≥10 mmHg) were noted in only two patients (three eyes), both in the PRK group. A 28-year-old male patient (baseline IOPs, 17 and 19 mmHg) had an IOP measurement of 29 mmHg in both eyes on postoperative day 18 while using LE gel one drop QID. LE gel dosage was decreased to one drop BID, and IOP measured 3 days later was 18 mmHg in both eyes, and 19 mmHg in both eyes after another 14 days. A 20-year-old female PRK patient (baseline IOPs, 14 mmHg OD, 13 mmHg OS) was prescribed LE gel one drop QID. On postoperative day 41, IOP was 19 mmHg OD and 23 mmHg OS. LE gel dosage was decreased to one drop three times daily. No further IOP measurements or other follow-up were available on this patient. Less significant/marked IOP elevations ≥5 mmHg were noted in one (0.6%) LASIK eye in the first postoperative month and one (4.2%) LASIK eye with follow-up >90 days (noted during a separate course of LE gel for dry eye approximately 6 months post-LASIK; see footnote in ). In contrast, among PRK eyes, IOP elevations of ≥5 mmHg occurred in 12 (11.5%) eyes within the first postoperative month, 12 (16.7%) eyes during the second postoperative month, six (11.1%) eyes with follow-up during the third postoperative month, and two (3.3%) eyes with follow-up extending longer than 90 days.
Table 4 IOP elevations, categorical changes from baseline
Discussion
The data gathered in this review of real-world use of LE gel in nearly 400 post-LASIK and post-PRK eyes indicate a high level of safety with this topical corticosteroid in both surgical procedures. There were no unexpected findings, and no patient was noted to have discontinued therapy prematurely with the exception of two PRK patients with corneal haze who both discontinued LE gel and were switched, one to prednisolone with no significant reduction in haze, and the other to difluprednate with no further follow-up available. Consistent with numerous prior studies with LE gel and other LE 0.5% formulations,Citation19–Citation27,Citation31 clinically significant IOP elevations (≥10 mmHg) were rare in this chart review and noted in only two (0.5%) patients (three eyes). In one patient for which sufficient follow-up information was available, reduction in LE gel administration frequency corresponded with a return of IOP to baseline levels. As might be expected, smaller IOP elevations (≥5 mmHg) were more frequent, and most often observed in PRK eyes, but still only noted in a small percentage of eyes overall. Notably, in PRK patients, considered at greater risk of IOP elevation, there were no elevations ≥10 mmHg reported for any eyes treated with LE gel beyond 60 days. In addition, mean postoperative IOP did not demonstrate any increase over the follow-up time frame which exceeded 60 days in a little more than one-third and 90 days in a little more than one-fourth of PRK eyes.
The dosing regimens of LE gel observed in this study followed expected patterns. Preoperatively, LE gel was administered in a small number of LASIK and PRK cases, and there were no instances of intraoperative administration. Ocular corticosteroids are recommended postoperatively for a short-time post-LASIK and for periods ranging from weeks to months following PRK.Citation1 In this study, almost all LASIK patients and nearly half of PRK patients began using postoperative LE gel on the same day as the surgery following completion of the procedure. The most common duration of LE gel treatment following LASIK was 7–14 days, with slightly less than 20% treated more than 30 days postoperatively. In contrast, 80% of PRK eyes were treated with LE gel for more than 30 days postoperatively, with slightly more than one-third treated for more than 60 days, and slightly more than one-fourth treated for more than 90 days. It should be noted that treatment duration was sometimes difficult to establish from patient charts. In some instances, standing orders were evident in the patient charts, outlining the planned course of treatment including LE gel dosing and planned duration, but there was no further documentation of LE gel usage within follow-up visit notes. In the absence of specific mention of treatment discontinuation, length of therapy was assumed to be according to respective site protocol.
Topical corticosteroids are highly valued in ophthalmology for their potent anti-inflammatory activity and utility in preventing certain postoperative complications, and have become a routine component of postsurgical management. However, corticosteroid class side effects such as IOP elevation, cataract formation, and delayed healing can complicate therapy and warrant a careful approach and vigilant follow-up when corticosteroids are administered directly onto the eye. The mechanism of corticosteroid-induced IOP elevation is theorized to involve glucocorticoid receptor-mediated changes in regulation of myocilin gene expression with a resulting decrease in outflow of aqueous humor secondary to changes in the trabecular meshwork.Citation34 LE has the ability to bind to the glucocorticoid receptor with greater affinity than dexamethasone and elicits potent and efficacious anti-inflammatory activity.Citation17,Citation18 However, due to the replacement of the C-20 ketone with a chloromethyl ester, unbound LE is rapidly metabolized into inactive metabolites thus limiting the potential to mediate unwanted side effects. In fact, clinical studies to date of this unique C-20 ester corticosteroid have reported consistently low rates of IOP elevation, comparable to vehicle and lower in comparison with other topical corticosteroids,Citation33 including dexamethasone,Citation25,Citation27,Citation35–Citation37 prednisolone,Citation20,Citation28,Citation29,Citation38,Citation39 and fluoromethalone.Citation23,Citation24,Citation40 The IOP findings from this chart review specific to the use of LE gel in refractive surgery extend the available safety data for LE gel beyond the postcataract surgery setting, and are consistent with findings from studies evaluating other LE formulations in refractive surgery. Thus, Zhang et alCitation22 recently described a chart review of 1,552 eyes that underwent excimer laser corneal refractive surgery managed postoperatively with LE suspension for 4 weeks (tapered regimen). Elevations in IOP, defined in this study as any increase in IOP over baseline (“low reaction”, >5 mmHg increase; “moderate reaction”, 5–15 mmHg increase; and “strong reaction”, <15 mmHg increase), were noted in 47 (3.0%) eyes occurring most often after 2 weeks of treatment. Four (0.3%) eyes were noted to have an IOP <15 mmHg over baseline. All IOP changes were reversible upon discontinuation of LE or treatment with 0.1% timolol hydrochloride. Similarly, Mifflin et alCitation26 reported results from a chart review of 579 eyes undergoing PRK treated postoperatively with either fluorometholone 0.1% (FML) or LE suspension, and reported clinically significant IOP elevations, defined as IOP elevations to >25 mmHg or >10 mmHg over baseline, in three (1.1%) FML eyes and four (1.3%) LE eyes over the 3 months follow-up. Mean IOP and/or elevations in IOP were also minimal in three prospective, comparative clinical trials of LE suspension for control of inflammation and pain following refractive surgery: Li et alCitation23 reported mean IOP was reduced from preoperative IOP in 160 eyes treated with LE suspension or FML following LASIK surgery and significantly lower in the LE-treated eyes compared with the FML-treated eyes (P<0.05). Gao et alCitation24 reported fewer IOP elevations in post-LASEK surgery eyes treated with LE vs those treated with FML (1.5% vs 6%; P<0.05). Patients (n=400) in that study received 1-week treatment with dexamethasone 0.1%/tobramycin 0.03% (dexamethasone/T) and fibroblast growth factor eye drops prior to being switched to either LE suspension or FML. Finally, Wu et alCitation25 compared the efficacy of 1-week treatment with LE that of dexamethasone/T in controlling postoperative inflammation in 224 post-LASIK eyes. An increase in mean IOP was noted at 1 week for dexamethasone/T-treated subjects compared with baseline (P<0.05) but not for LE-treated subjects.
The newer gel formulation of LE offers some benefits relative to the ointment and suspension formulations. The gel formulation has 70% less benzalkonium chloride preservative and a more physiologic pH when compared with the suspension formulation. The gel also contains two additional demulcents that act as moisturizing agents. LE suspension requires vigorous shaking prior to administration in order to ensure uniform distribution of drug and consistent dosing. LE gel is a non-settling formulation that requires no shaking prior to administration. The vehicle behaves as a semisolid gel at rest, but shear-thins to a liquid when the bottle is squeezed, allowing it to flow and easily express as a drop. Upon mixing with tear fluid on the ocular surface, the vehicle converts to a liquid.Citation30 This avoids one of the major drawbacks of the ointment formulation, namely blurred vision. However, the LE gel formulation is thought to provide prolonged corneal and conjunctival contact time relative to the suspension formulationCitation30 warranting continued vigilance with regard to potential safety ramifications, particularly with long-term use. Our study in post-PRK and post-LASIK patients included a sizable number of PRK eyes treated with LE gel for periods exceeding 60 and 90 days with little apparent effect on IOP. The two cases of IOP increase ≥10 mmHg were noted at days 18 and 41, respectively, with higher frequency of use, and the IOP elevation returned to baseline with decreased frequency of administration in the case where follow-up information was available.
Advancements in PRK equipment and technique such as higher-quality lasers, small flying-spot delivery systems, and larger ablation zones may help reduce the incidence of corneal haze, nonetheless it still remains a risk, particularly in cases with high myopia.Citation41–Citation44 The frequency of corneal haze following PRK in this study was low; 19.1% of PRK eyes were noted to have any instance of corneal haze, and only 1.4% of PRK eyes developed haze that was classified as moderate/severe. While this study was not designed to evaluate efficacy and corneal abnormalities were gathered as safety findings, the low rate of corneal haze observed in this population may be an indication of clinical benefit of LE gel in that regard as well. While there was no control group in our analysis to provide perspective, the frequency of haze reported was very similar to findings reported in the chart review study by Mifflin et alCitation26 comparing the suspension formulation of LE and FML in PRK patients. The percentage of eyes in that study with any incidence of haze ranged from approximately 18% to 27% during the first 2 months of follow-up. Visual outcomes in the two treatment groups were excellent, with a small, but statistically significant difference in favor of LE for mean uncorrected distance visual acuity at 6 months (P=0.013).
The main limitations of this study are the lack of a control group and the real-world, retrospective nature of the data collection, the latter of which contributed unavoidable consequences of missing data, most notably with regard to IOP follow-ups and details regarding the duration of LE gel treatment in some cases. Likewise, data gathering was limited primarily to objective findings such as IOP measurements and surgical outcomes; it was not possible to evaluate more subjective variables such as pain relief or patient satisfaction. The primary goal of this chart review was to characterize patterns of LE gel use in refractive surgery and assess the overall safety in these settings. Collection of safety data in this study, as in any retrospective chart review, was limited to information previously recorded during routine patient follow-up visits. As a result, it is possible that minor complaints may not have been noted, and patients may not have been questioned about certain AEs. However, it is presumed that any such events of clinical significance would have been recorded.
Finally, applanation tonometry was used to determine pre- and postrefractive IOP at all five clinical sites participating in this retrospective chart review. IOP measures were not corrected to account for the decreased central corneal thickness (CCT) either in the patient charts or in the analysis of cumulative IOP data from all five sites. This may also be a limitation. Applanation tonometry is based on the assumption that eyes have a uniform shape and CCT, and may therefore underestimate the real IOP in postrefractive eyes, particularly in postoperative eyes of moderate and highly myopic patients where changes in CCT are known to be greater. However, to date, no accepted IOP-adjustment formulas have been established specifically for applanation tonometry in postkeratorefractive eyes to account for the change in CCT. While dynamic contour tonometry has been suggested to be more accurate for IOP measurements in postrefractive surgery eyes,Citation45,Citation46 it is not widely available. As a precaution, we recommend any postkeratorefractive surgery patient with IOP increases of ≥5 mmHg as measured with applanation tonometry be followed more closely, especially in patients with greater depths of laser ablation. Despite the limitation of applanation tonometry, it is noteworthy that in the current chart review, there was only a relatively small percentage of patients with IOP elevations ≥5 mmHg.
Conclusion
Based on the real-world experience captured in this chart review, LE gel appears to have a high level of safety and tolerability when used for the management of postoperative pain and inflammation following LASIK and PRK surgery. AEs were few and not unexpected given the nature of refractive surgery cases, and there were no unusual corneal findings or healing abnormalities. The only meaningful safety-related findings included two PRK eyes with moderate/severe corneal haze and three PRK eyes of two patients with a clinically significant IOP elevation. These data corroborate a growing body of research suggesting that LE, in gel, suspension, and ointment formulation and in a variety of ocular surgical settings, provides the clinical benefits desired from a topical corticosteroid, and with an optimized safety profile.
Acknowledgments
Data collection and analysis was performed by Churchill Outcomes Research (Maplewood, NJ, USA) and funded by Bausch + Lomb, Inc. (Rochester, NY, USA). Writing assistance was provided by Sandra Westra, PharmD of Churchill Communications (Maplewood, NJ, USA), funded by Bausch + Lomb, Inc. This study was funded by Bausch + Lomb, Inc., Rochester, NY, USA.
Disclosure
CL Salinger has served as an advisory board member and paid speaker for Bausch + Lomb, Inc. MA Jackson is a consultant for Bausch + Lomb, Inc. The other authors report no conflicts of interest in this work.
References
- American Academy of Ophthalmology Refractive Management/Intervention PanelPreferred Practice Pattern® Guidelines. Refractive Errors and Refractive SurgerySan Francisco, CAAmerican Academy of Ophthalmology2013 Available from: www.aao.org/pppAccessed May 4, 2015
- NarooSACharmanWNChanges in posterior corneal curvature after photorefractive keratectomyJ Cataract Refract Surg20002687287810889434
- DuppsWJWilsonSEBiomechanics and wound healing in the corneaExp Eye Res20068370972016720023
- ShorttAJAllanBDEvansJRLaser-assisted in-situ keratomileusis (LASIK) versus photorefractive keratectomy (PRK) for myopiaCochrane Database Syst Rev20131CD00513523440799
- LoewensteinALipshitzIVarssanoDLazarMComplications of excimer laser photorefractive keratectomy for myopiaJ Cataract Refract Surg199723117411769368160
- AlioJLArtolaAClaramontePJAyalaMJSanchezSPComplications of photorefractive keratectomy for myopia: two year follow-up of 3000 casesJ Cataract Refract Surg1998246196269610444
- Moller-PedersonTCavanaghHDPetrollWMJesterJVStromal wound healing explains refractive instability and haze development after photorefractive keratectomy: a 1-year confocal microscopic studyOphthalmology20001071235124510889092
- DonnenfeldEDO’BrienTPSolomonRPerryHDSpeakerMGWittpennJInfectious keratitis after photorefractive keratectomyOphthalmology200311074374712689896
- WroblewskiKJPasternakJFBowerKSInfectious keratitis after photorefractive keratectomy in the United States army and navyOphthalmology200611352052516488012
- de RojasVLlovetFMartinezMInfectious keratitis in 18,651 laser surface ablation proceduresJ Cataract Refract Surg2011371822183121865006
- VetrugnoMMainoAQuarantaGMCardiaLThe effect of early steroid treatment after PRK on clinical and refractive outcomesActa Ophthalmol Scand200179232711167281
- BaekSHChangJHChoiSYKimWJLeeJHThe effect of topical corticosteroids on refractive outcome and corneal haze after photorefractive keratectomyJ Refract Surg1997136446529427202
- ArasCOzdamarAAktuncRErcikanCThe effects of topical steroids on refractive outcome and corneal haze, thickness, and curvature after photorefractive keratectomy with a 6.0-mm ablation diameterOphthalmic Surg Lasers1998296216279715485
- O’BrartDPLohmannCPKlononsGThe effects of topical corticosteroids and plasmin inhibitors on refractive outcome, haze, and visual performance after photorefractive keratectomy. A prospective, randomized observer-masked studyOphthalmology1994101156515747522315
- McGheeCNDeanSDanesh-MeyerHLocally administered ocular corticosteroids: benefits and risksDrug Saf200225335511820911
- BodorNLoftssonTWuWMMetabolism, distribution, and transdermal permeation of a soft corticosteroid, loteprednol etabonatePharm Res19929127512781448425
- DruzgalaPWuWMBodorNOcular absorption and distribution of loteprednol etabonate, a soft steroid, in rabbit eyesCurr Eye Res1991109339371959381
- ComstockTLDeCoryHHAdvances in corticosteroid therapy for ocular inflammation: loteprednol etabonateInt J Inflam2012201278962310.1155/2012/78962322536546
- ComstockTLPaternoMRSinghAErbTDavisESafety and efficacy of loteprednol etabonate ophthalmic ointment 0.5% for the treatment of inflammation and pain following cataract surgeryClin Ophthalmol2011517718621383946
- LaneSSHollandEJLoteprednol etabonate 0.5% versus prednisolone acetate 1.0% for the treatment of inflammation after cataract surgeryJ Cataract Refract Surg20133916817323232255
- The Loteprednol Etabonate Postoperative Study Group 2A double-masked, placebo-controlled evaluation of 0.5% loteprednol etabonate in the treatment of postoperative inflammationOphthalmology1998105178017869754192
- ZhangQ-SWangXWangZ-HInfluence of lotemax eyedrops on intraocular pressure following excimer laser corneal refractive surgeryChin J Exp Ophthalmol2013316551554
- LiW-TLiHWeiJClinical study on the application of 5 g/L loteprednol etabonate ophthalmic suspension after LASIKInt J Ophthalmol201010917921793
- GaoD-HLiK-JLuHClinical observations on the effect of Lotemax on changes in intra-ocular pressure after LASEK [sic: LASIK]Int J Ophthalmol2010109806807
- WuJ-SZhongX-WZhangX-XA randomized controlled study on the application of 0.5% loteprednol etabonate eye drops after LASIK surgeryChin J Exp Ophthalmol2012307641645
- MifflinMDLeishmanLLChristiansenSMSikderSHsuMMoshirfarMUse of loteprednol for routine prophylaxis after photo-refractive keratectomyClin Ophthalmol2012665365922570546
- ThanathaneeOSriphonPAnutarapongpanOA randomized controlled trial comparing dexamethasone with loteprednol etabonate on postoperative photorefractive keratectomyJ Ocular Pharmacol Ther201531165168
- HollandEJDjalilianARSandersonJPAttenuation of ocular hypertension with the use of topical loteprednol etabonate 0.5% in steroid responders after corneal transplantationCornea2009281139114319770719
- BartlettJDHorwitzBLaibovitzRHowesJFIntraocular pressure response to loteprednol etabonate in known steroid respondersJ Ocul Pharmacol199391571658345288
- CoffeyMJDeCoryHHLaneSSDevelopment of a non-settling gel formulation of 0.5% loteprednol etabonate for anti-inflammatory use as an ophthalmic dropClin Ophthalmol2013729931223430378
- RajpalRKRoelLSiou-MermetRErbTEfficacy and safety of loteprednol etabonate 0.5% gel in the treatment of ocular inflammation and pain after cataract surgeryJ Cataract Refract Surg20133915816723218817
- FongRLeitrizMSiou-MermetRErbTLoteprednol etabonate gel 0.5% for postoperative pain and inflammation after cataract surgery: results of a multicenter trialClin Ophthalmol201261113112422888209
- International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human UseICH Harmonised Tripartite Guideline. Guideline for Good Clinical Practice E6(R1)61996 Available from: http://www.ich.org/products/guidelines/efficacy/efficacy-single/article/good-clinical-practice.htmlAccessed October 8, 2015
- PleyerUUrsellPGRamaPIntraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same?Ophthalmol Ther201322557225135807
- WhiteEMMacyJIBatemanKMComstockTLComparison of the safety and efficacy of loteprednol etabonate 0.5%/tobramycin 0.3% with dexamethasone 0.1%/tobramycin 0.3% in the treatment of blepharokeratoconjunctivitisCurr Med Res Opin20082428729618062846
- ChenMGongLSunXA multicenter, randomized, parallel-group, clinical trial comparing the safety and efficacy of loteprednol etabonate 0.5%/tobramycin 0.3% with dexamethasone 0.1%/tobramycin 0.3% in the treatment of Chinese patients with blepharokeratoconjunctivitisCurr Med Res Opin20122838539422256909
- HollandEJBartlettJDPaternoMRUsnerDWComstockTLEffects of loteprednol/tobramycin versus dexamethasone/tobramycin on intraocular pressure in healthy volunteersCornea200827505518245967
- NovackGDHowesJCrockettSSherwoodMBChange in intraocular pressure during long-term use of loteprednol etabonateJ Glaucoma199872662699713785
- Loteprednol Etabonate US Uveitis Study GroupControlled evaluation of loteprednol etabonate and prednisolone acetate in the treatment of acute anterior uveitisAm J Ophthalmol199912753754410334346
- JungHHJiYSSungMSKimKKYoonKCLong-term outcome of treatment with topical corticosteroids for severe dry eye associated with Sjogren’s syndromeChonnam Med J201551263225914877
- AllanBDHassanHTopography-guided transepithelial photorefractive keratectomy for irregular astigmatism using a 213 nm solid-state laserJ Cataract Refract Surg2013399710423158680
- HansenRSLyhneNGrauslundJGronbechKTVestergaardAHFour-year to seven-year outcomes of advanced surface ablation with excimer laser for high myopiaGraefes Arch Clin Exp Ophthalmol201525371027103325582070
- DawsonDGGrossniklausHEMcCareyBEEdelhasuerHFBiomechanical and wound healing characteristics of corneas after excimer laser keratorefractive surgery: is there a difference between advanced surface ablation and sub-Bowman’s keratomileusis?J Refract Surg200824S90S9618269157
- SiganosDSKatsanevakiVJPallikarisIGCorrelation of subepithelial haze and refractive regression 1 month after photorefractive keratectomy for myopiaJ Refract Surg19991533834210367577
- SadighALFouladiRJHashemiHBeheshtnejadAHA comparison between Goldmann applanation tonometry and dynamic contour tonometry after photorefractive keratectomyGraefes Arch Clin Exp Ophthalmol201325160360822940796
- AristeidouAPLabirisGKatsanosAFanariotisMFoudoulakisNCKozobolisVPComparison between Pascal dynamic contour tonometer and Goldmann applanation tonometer after different types of refractive surgeryGraefes Arch Clin Exp Ophthalmol2011249576777320577756