
Abstract
Infantile nystagmus (IN), previously known as congenital nystagmus, is an involuntary to-and-fro movement of the eyes that persists throughout life. IN is one of three types of early-onset nystagmus that begin in infancy, alongside fusion maldevelopment nystagmus syndrome and spasmus nutans syndrome. Optometrists may also encounter patients with acquired nystagmus. The features of IN overlap largely with those of fusion maldevelopment nystagmus syndrome, spasmus nutans syndrome, and acquired nystagmus, yet the management for each subtype is different. Therefore, the optometrist’s role is to accurately discern IN from other forms of nystagmus and to manage accordingly. As IN is a lifelong condition, its presence not only affects the visual function of the individual but also their quality of life, both socially and psychologically. In this report, we focus on the approaches that involve optometrists in the investigation and management of patients with IN. Management includes the prescription of optical treatments, low-vision rehabilitation, and other interventions such as encouraging the use of the null zone and referral to support groups. Other treatments available via ophthalmologists are also briefly discussed in the article.
Introduction
Infantile nystagmus (IN), a constant involuntary to-and-fro movement of the eyes that persists throughout life, is one of three types of early-onset nystagmus that begin in infancy. Fusion maldevelopment nystagmus syndrome (FMNS), which was formerly known as latent nystagmus, and spasmus nutans syndrome (SNS) are the other two types. Previously, various terms have been used to refer to IN, the most common being congenital nystagmus. Despite this label, the condition is rarely present at birth. A study by Reinecke et alCitation1 reported the development of nystagmus in the first 2 weeks of life in only three of 35 infants examined. Since IN typically develops within the first few months after birth, the term congenital has been replaced with infantile.Citation2 The occurrence of IN in the general population is estimated to be 0.14%.Citation3 This included nystagmus associated with visually impaired conditions and nystagmus with no known condition (idiopathic). The prevalence of any form of nystagmus (ie, not just IN) is estimated at 0.17% in people under the age of 18. In contrast, the prevalence is much higher in the adult population (0.27%).Citation3 This increase is accounted for by cases of acquired nystagmus, which generally (but not always) occurs later in life. IN can occur spontaneously, or it may be inherited. Hereditary IN may be X-linked, recessive, or dominant.Citation4 A number of genetic studies have discovered mutations in the FRMD7 gene in individuals with X-linked idiopathic IN.Citation5 These mutations account for approximately 20%–57% of X-linked cases of idiopathic IN and 3.6%–7% of isolated cases.Citation6,Citation7
Clinical characteristics of IN
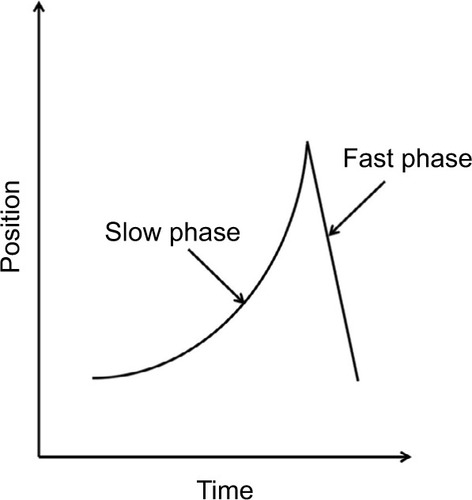
In IN, the eyes oscillate constantly and predominantly in the horizontal axis, although vertical and/or torsional movement may be present as a secondary component.Citation8 The nystagmus occurs in both eyes and is usually conjugate. Thus, the amplitude of IN is similar in both eyes, ranging between 0.3° and 15.7°, with an average frequency of 2–3 Hz.Citation8,Citation9 A nystagmus cycle consists of two phases: an initiating slow phase in which the eyes slowly move away from the fixation point, and a corrective phase where the eye moves back toward the fixation point (). This corrective phase can be either a slow or a fast eye movement. A pendular pattern is seen when both the initiating and corrective phases are slow movements, and a jerk pattern is seen when the corrective phase is a saccade. These patterns differ between individuals with IN, and also within the individuals themselves at different gaze angles or times.Citation10
Figure 1 Waveform showing the initiation (slow) phase and correction (fast) phase of a jerk nystagmus cycle.
The IN waveform
The nystagmus waveform represents the position of the eye over time, and it is obtained by performing eye movement recordings. It is described in terms of its amplitude, frequency, and the overall pattern or shape of the oscillation. Nystagmus intensity is calculated by multiplying the nystagmus amplitude by the frequency, thus representing the average velocity of the eye movements.Citation11 The intensity of an individual’s nystagmus is not typically constant and can be influenced by a number of factors. Among these factors is the direction of gaze. The intensity of IN is at a minimum at certain gaze angle(s) known as the null zone. The null zone is within 10° of the primary position (straight ahead) in 73% of individuals with IN.Citation8 If the null zone is not in the primary position, patients may adopt an abnormal head posture (AHP) to place the eyes in this position. In many individuals (44%), nystagmus intensity also reduces during convergence.Citation8,Citation12,Citation13 Furthermore, the state of attention and fatigue can affect nystagmus intensity.Citation14 Stress, for example, has been found to increase intensity.Citation15,Citation16 These factors should be taken into consideration during an eye examination, as they may affect the outcome of clinical tests.
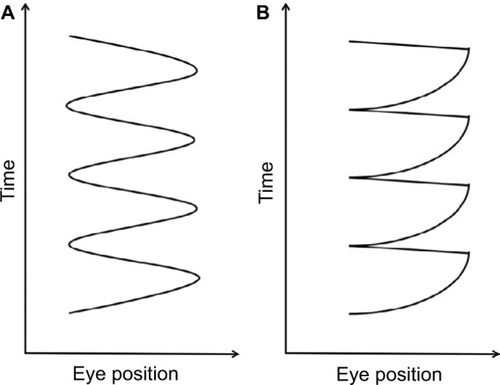
A total of 12 waveform patterns have been identified in IN.Citation4 These 12 waveforms can be broadly categorized into pendular and jerk waveforms (). The velocity of a pendular eye movement is equal in both directions. The eyes may change direction smoothly, producing a sinusoidal pendular waveform, or they may change direction abruptly, producing a triangular waveform.Citation17 Jerk waveforms, however, consist of a slow phase in one direction followed by a corrective saccade, known as a fast phase. It is further described by the direction of the fast phase, whether it is left, right, up, or down. A specific characteristic of the jerk IN waveform that distinguishes it from other types of nystagmus is the accelerating slow phase that follows the foveation period; a period when the eye movement is relatively slower for a short period of time when the object of regard coincides with the fovea.Citation17,Citation18 An accelerating slow phase is unlikely to be visible to an examiner, so this can only be confirmed by using a high-speed eye tracking device.
Figure 2 (A) Pendular and (B) jerk waveform patterns in IN.
The evolution of the IN waveform during visual development has been investigated by a number of researchers. One of the earliest studies – in three infants – reported that IN started with large triangular waveforms, developing into pendular and, subsequently, jerk waveform nystagmus by 7 months to 1.5 years.Citation1 However, a later study observed square-wave jerks (a form of saccadic intrusion) at 7 weeks of age, which then developed into a smaller amplitude (4°–20°) pendular nystagmus at 8 weeks.Citation20 Over the next few weeks, the amplitude first increased (to approximately 30°) and then began to decrease to 4°–10° until 7.5 months. A more recent study was conducted on a group of 20 infants aged between 4 and 42 months in whose nystagmus a combination of two components was observed, ie, asymmetric pendular and pseudocycloid waveforms, which was previously undocumented.Citation21 In addition, the researchers observed a decrease in the amplitude of both components of waveforms from birth until 1.5 years of age. Foveation duration also increased up to the age of 1.5–2 years, and thereafter remained relatively stable.
Although the exact type of IN waveform is not crucial for the diagnosis of IN itself, knowledge about the different waveforms is helpful in estimating the visual prognosis. For instance, pendular waveforms are more likely to be associated with an identifiable visual system pathology.Citation22 Therefore, children with a pendular waveform that persists longer are suspected to have more poorly developed vision, as compared to children who transition to a jerk waveform earlier.Citation23 Although access to eye movement recording equipment is limited in optometric practices, it is usually possible to determine whether a waveform is pendular or jerk without an eye tracker, just by direct observation. Jerk nystagmus, for instance, can be determined simply by observing the beat direction (ie, fast phase).
Visual acuity (VA)
VA varies widely in patients with IN, depending on the associated visual condition (if any). The mean VA of individuals with idiopathic IN (IN with no associated visual pathology) is 0.35 logMAR, which is better than that of individuals with associated visual system pathology (0.67 logMAR in patients with albinism, and 0.55 logMAR in the group with any other ocular pathology).Citation8 The poor VA seen in patients with IN could be due to the underlying pathology, motion-blur-induced stimulus deprivation amblyopia, or a combination of both.Citation24
Refractive error
Individuals with IN are more likely to have high refractive error than the general population. The range of refractive errors found in patients with IN is very broad. Some studies find that hyperopia is more common in IN,Citation25 regardless of the VA,Citation26 while others report that the trend is more myopic.Citation27 The prevalence of corneal astigmatism (especially with-the-rule astigmatism) is also remarkably high in individuals with IN.Citation28 The average amount of astigmatism in these individuals is 1.85DC; 57% of people with IN have astigmatism higher than 2.00DC.Citation8 Astigmatism tends to increase with ageCitation29 and is suspected to be caused by the interaction between the cornea and the eyelids during the constant oscillations.Citation28,Citation30 Although full correction is given, patients with IN are better able to distinguish horizontal stimuli than vertical ones,Citation24,Citation31–Citation33 which may be attributable to the presence of meridional amblyopia.Citation33,Citation34
Reading performance
Nystagmus intensity decreases when converging to view near objects in around 44% of individuals with IN.Citation8,Citation12 However, there is no significant improvement in near VA at this time, despite significant dampening of the nystagmus.Citation11,Citation9 Barot et alCitation35 studied the reading performance of 71 individuals with IN and 20 controls, measuring reading acuity, near VA, and reading speed. Reading performance was 18.8% slower in participants with IN associated with albinism and 14.7% slower in idiopaths. However, near-normal reading speed can be accomplished by using a font size up to 0.6 logMAR larger than the near VA.Citation35
Reversed optokinetic nystagmus (OKN) response
Another unique characteristic of IN is reversal of the OKN response. In a typical person without nystagmus, the fast phase of OKN beats in the opposite direction to the stimulus. However, some individuals with IN show a reversed response, ie, the fast phase of the OKN beats in the same direction as the stimulus.Citation36,Citation22
Oscillopsia
Despite the constant oscillation of the eyes that produce retinal image motion, people with nystagmus generally perceive the world as stable.Citation37 Therefore, they rarely complain of oscillopsiaCitation38 (perception of the world swinging back and forth).Citation39 In contrast, oscillopsia is commonly experienced by patients with acquired nystagmus.Citation22 However, reports of oscillopsia are not necessarily indicative of acquired nystagmus, but should be an indication for further investigation. Individuals with IN can sometimes experience oscillopsia intermittently in situations such as when they are tired, excited, stressed, or concentrating.Citation8
Head nodding
Another occasional feature of IN is head nodding.Citation8 This head oscillation is independent of the oscillation occurring in the eyes, often being in a different direction or with a different phase. Head nodding clearly does not compensate for the nystagmus eye movements, and its etiology is unclear. It can be suppressed by the patient voluntarily, but may recur if the patient’s attention is distracted from doing so.Citation40 This feature of IN is also present in SNS, but in SNS, the head oscillation is in synchrony with the eyes. Key distinguishing features of SNS and IN can be seen in eye movement recordings, as the waveform of SNS is asymmetrical between the two eyes, pendular, high in frequency, and low in amplitude.Citation2,Citation22
Associated conditions vs idiopathic IN
IN can present with anterior visual pathway abnormalities, or it can present without any detectable abnormalities at all (ie, it can be idiopathic). Anterior visual pathway abnormalities occur in 38%–91% of cases of IN.Citation3,Citation8,Citation41,Citation42 This includes, but is not limited to, congenital cataracts, retinal dystrophies, and degenerations such as Leber’s congenital amaurosis, optic nerve disorders such as optic nerve hypoplasia and optic atrophy, foveal hypoplasia, aniridia, albinism, achromatopsia, and achiasma. Only 9% of cases of IN are reported as idiopathic,Citation41,Citation42 although Lorenz and GampiCitation43 and Abadi and BjerreCitation8 reported a higher prevalence. However, since the idiopathic diagnosis can only be reached after all possible associated visual conditions have been excluded, the prevalence of IN depends to some extent upon the persistence of the investigator and the exhaustiveness of clinical testing. Children with IN associated with sensory abnormalities tend to have poorer vision than those who are idiopathic. Therefore, it is important to distinguish the two so that appropriate management can be given.
Optometric investigation of IN
Although unlikely, an optometrist may come across a patient with nystagmus (whether a child or an adult) who has not been seen by the hospital eye services. Referral of these cases is essential so that an underlying cause can be identified, if possible. The optometrist must ascertain the appropriate speed of referral by deciding, following a detailed discussion of history and symptoms, whether the nystagmus is likely to be infantile or acquired – the latter requiring emergency referral. Often, the history can be very informative in making this determination. The difficulty in making such a differential diagnosis by signs is due to the fact that the features of IN overlap largely with those of acquired nystagmus, FMNS, and SNS. However, some key features are distinguishable. For example, features of acquired nystagmus include a pronounced vertical component, complaints of oscillopsia, and saccadic oscillations without apparent slow phases (technically, saccadic oscillations are not a form of nystagmus, but these conditions are often misdiagnosed as such and require onward referral).Citation22 Note that asymmetrical movements between the two eyes raises the likelihood of the nystagmus being acquired, although this feature may not be seen with the naked eye. IN is not a progressive condition, and changes in nystagmus are not expected in adulthood. Therefore, any suspected changes in nystagmus in adults should always be referred to the hospital eye service as they could represent (however unlikely) the development of comorbid acquired nystagmus.
On the other hand, FMNS is often associated with infantile esotropia and amblyopia (which disrupts binocularity).Citation44 In FMNS, nystagmus might not be observable under binocular viewing (without eye movement recording) but becomes apparent when one eye is occluded. The nystagmus fast phase will be seen beating toward the uncovered eye, while remaining conjugate. FMNS respects Alexander’s Law, ie, that the nystagmus gets more intense in abduction. This means that if the left eye is viewing, the nystagmus is more intense in leftgaze, and vice versa. Moreover, in IN, an increase in the intensity can sometimes be seen when one eye is covered, indicating the presence of a latent component. Therefore, the cover test should be performed to determine the presence of a latent component or FMNS.
Key features of SNS include a low amplitude, high frequency (often >10 Hz), and asymmetrical pendular nystagmus that may be conjugate or disconjugate. In addition, children with SNS usually present with AHP and head nodding.Citation2,Citation22 Also, oscillations of the eyes often reduce to subclinical levels after a few years,Citation45,Citation46 giving the impression that the nystagmus has disappeared.
Performing tests on patients with nystagmus can be a clinical challenge requiring good skills. For example, tests that require the eyes to be still – such as noncontact tonometry – may be difficult to undertake. However, the alternative of using a contact tonometer has a higher risk of causing corneal abrasion. The clinician will need to use their individual judgment in each situation depending on the patient and test being performed. Consider using the patient’s null zone to dampen nystagmus while carrying out tests such as perimetry. As mentioned earlier, stress can increase nystagmus intensity, so the practitioner should do everything possible to minimize the patient’s anxiety and discomfort.
Nystagmus intensity increases with occlusion in patients with a latent component, which may produce an artefactual reduction in VA. To avoid this increase in intensity, fogging should be used to remove fixation of the untested eye, using convex lenses between +4.00DS and +10.00DS.Citation47 Studies have shown that patients with IN take longer to direct their gaze toward a fixated target and report slowness to see.Citation48,Citation49 Therefore, giving patients more time to respond when reading the acuity chart would be beneficial to both the patient and practitioner.
Although performing refraction on a patient with nystagmus may seem challenging, an accurate refraction can still be obtained. The use of trial frames and wide-aperture trial lenses (as opposed to a phoropter) are advantageous, as they allow the patient to move their head freely toward – if not into – their null zone.
Slit-lamp examination and funduscopy are essential to rule out conditions commonly associated with IN. The practitioner should look for structural abnormalities such as iris transillumination (albinism) and congenital cataracts. During funduscopy, attention should be paid to abnormalities in the optic disc (optic nerve hypoplasia), fovea (foveal hypoplasia in albinism or aniridia), and fundus pigmentation. Optical coherence tomography should be used to assess for foveal hypoplasia. Given that idiopathic IN is a diagnosis by exclusion, the hospital eye service can be expected to perform electroretinography and visual evoked potentials to assess for disorders such as congenital stationary night-blindness and cone dysfunction, which can be difficult to detect with funduscopy alone.
Management by the optometrist
In this paper, we focus on the approaches that involve optometrists in the management of individuals with IN. This includes the prescription of optical treatments, low-vision rehabilitation, and other interventions such as use of the null zone and support groups.
Optical prescription
As might be expected, correction of refractive error has been shown to improve the VA of individuals with IN.Citation50,Citation51 Correction of even the smallest significant amount of refractive error can result in subjective improvements in vision. Therefore, the management should begin with correction of refractive errors, usually with spectacles. However, the use of spectacles may not be ideal in patients with an AHP caused by an eccentric null zone, as it may require them to use an eccentric point of the lens. This will induce prismatic and peripheral lens effect aberrations, leading to blurred vision and perhaps asthenopia. In such cases, contact lenses may be prescribed.
The use of contact lenses to correct refractive error has been reported to improve VA by at least one line when compared to the use of spectacles.Citation52,Citation53 The presence of contact lenses on the eyes appears to dampen nystagmus intensity, an effect that does not occur when the eye is anesthetized.Citation54 This suggests that correction of refractive error may not be the primary mechanism involved, and that the sensory feedback from the contact lenses on the cornea or lids might have a moderating impact on the nystagmus. The presence of high with-the-rule astigmatism in patients with IN leads to a higher sensitivity to rotational instability of the contact lens, resulting in reduced VA.Citation55 Therefore, special care must be taken when fitting contact lenses to these patients. The use of rigid gas-permeable lenses may provide a more stable fit compared to soft lenses in these cases.Citation55
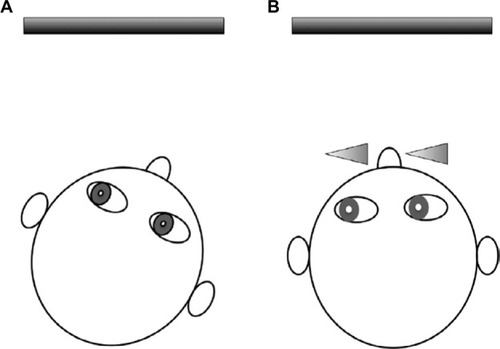
Prisms may be used to reduce AHP by shifting the eyes into the null position while the head is in the primary position. As an example, base right prisms can be used to shift the eyes into left gaze for patients with a leftward null zone, allowing the head to remain straight (). Be aware that eccentric null positions will require high powered prisms, which may be heavy. An alternative is to use Fresnel stick-on prisms, although neither option may be cosmetically acceptable to the patient. Patients with IN who have a null zone in the convergent position may benefit from wearing base out spectacle prisms that will induce convergence and thus dampen nystagmus intensity when viewing distant targets.Citation56 This can be achieved by prescribing 7Δ base out in front of both eyes, with –1.00DS to compensate for the accommodation that accompanies the convergence.Citation57,Citation40 In rare cases, some nystagmats may present with a divergence null. In such cases, base-in prisms would be beneficial.Citation58
Figure 3 Example of reducing a right AHP (A) using base right prisms to shift the eyes into the direction of the null zone (left gaze) while the head is in primary position (B).
Low-vision rehabilitation
As discussed above, the VA of individuals with IN is usually reduced. Although some may have 6/6 or better vision, most are visually impaired, affecting their ability to perform daily tasks. For this group of individuals, low-vision rehabilitation is beneficial. This includes increasing the font size of texts together with the use of optical or electronic magnification devices. The use of devices such as tablets is ideal, as these can provide a wide range of magnifications. Additionally, other adaptive strategies during viewing (eg, use of the null zone) can also be trained.
Use of the null zone
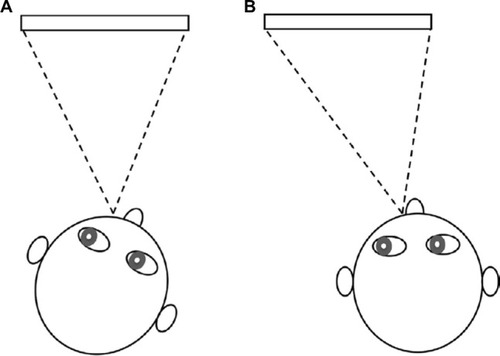
Many of the interventions available for IN aim to utilize the null zone, which has been shown to improve VA.Citation59 Nystagmats sometimes adopt an AHP to achieve the required gaze position, but long-term use of such head postures may lead to a restriction of neck movement.Citation60 Besides using prisms, adjustment to the surroundings, such as changing the seating position during viewing, can be made to place the eyes into the null zone while keeping the head straight. Such adjustments may improve the patient’s comfort for long periods of viewing. illustrates an example of environmental changes that can be made in a classroom for a child with a null zone in left gaze.
Figure 4 Example of environmental changes for a child with a left null zone (A). The child can be seated to on the right side of the classroom/television to place the eyes into the left gaze for a more comfortable head posture (B).
Support groups
IN is a lifelong condition that affects not only visual function but also the quality of life of patients and those who are close to them.Citation61,Citation62 A recent study by McLean et alCitation61 investigated the impact of nystagmus on the daily life of patients older than 16 years. The authors found that the physical appearance of nystagmus causes individuals to suffer from low self-esteem. The constant oscillation of the eyes and AHP made participants feel that they stand out and/or do not fit in with their peers. This can lead to social withdrawal. An earlier study by Pilling et alCitation62 on the social and visual function in nystagmus discovered that children with nystagmus have poorer social function compared to adults.
Besides confidence issues, many individuals with nystagmus feel frustrated with the lack of understanding from the general public regarding their condition. Many also report feeling abandoned by the medical community. This can lead to feelings of hopelessness and fear of failing.Citation61 The findings from these studies demonstrate the importance of raising awareness of nystagmus and the need for support groups for patients. Therefore, it is important for patients to get the correct information and support regarding their condition. In the UK, patients with any form of nystagmus can be referred to Nystagmus Network (http://nystagmusnetwork.org), a charity and support group that provides information and support for family members and children who are growing up with nystagmus.Citation63 Child patients should always be referred to the Local Educational Authority’s VI support service.
Treatments for IN
A number of treatments by ophthalmologists are available for nystagmus depending on the type and presenting symptoms. These treatments do not completely cure the nystagmus, but rather modify the waveform and/or reduce AHP. A review by Thurtell and LeighCitation64 discusses the various therapies available for different types of nystagmus, including both surgical and pharmaceutical options. As with optical treatments, the aims are to improve the VA, correct any AHP, and treat any strabismus.Citation47 Some treatments also aim to reduce nystagmus intensity.Citation47,Citation64
Surgical treatment
Several surgical procedures have been reported to improve nystagmus in patients with IN. Surgery is indicated when there is a null point at eccentric gaze causing a significant AHP, presence of strabismus, or to improve VA through the use of convergence.Citation65,Citation66 One of the earliest surgical procedures to be developed involved recession and resection of the extraocular muscles to move the null zone into the primary position of gaze (Kestenbaum surgery).Citation67 Artificial divergence surgery is another method involving recession of both medial rectus muscles in patients with nystagmus that dampens on convergence.Citation68 A combination of this surgery with the Kestenbaum technique has been shown to produce a better visual outcome compared to performing each procedure on its own.Citation69,Citation70 Following the success of the Kestenbaum surgery in improving VA in patients with IN, it was hypothesized that similar outcomes would be produced through a combined procedure of tenotomy (detachment of the muscles) and reattachment at the same site of the muscle origin.Citation71 Subjective improvement in VA has been reported. However, there are only limited reports of improvement in clinically measured VA.Citation71–Citation74
Pharmacological treatment
Various drugs have been reported to reduce nystagmus intensity in IN.Citation75 The only ones to have gone through a randomized controlled trial are memantine and gabapentin. The improvement in vision seen with the prescription of memantine was 0.15 logMAR compared to placebo (0.04 logMAR). Slightly less improvement in VA was seen with gabapentin (0.09 logMAR).Citation75–Citation77
Cannabis and baclofen have also shown potential for improving VA in IN, but these medications have not undergone rigorous testing. The effect of smoking cannabis was shown through eye movement recordings and improved VA in one case study of a 19-year-old patient with nystagmus.Citation78 Baclofen is known to reduce nystagmus amplitude and AHP and increase VA, and is often used in patients with periodic alternating nystagmus, a form of IN that reverses direction.Citation79 The reader is directed to recent review articles for a full discussion of other pharmacological treatments of IN.Citation80–Citation82
Conclusion
The principal aim of an optometrist’s investigation of a patient with nystagmus should be to distinguish the characteristics that differentiate IN from the various other forms of the condition. This can be difficult, as many of the features overlap in the various subtypes. Correct diagnosis is crucial however, as proper management may at the least improve quality of life, and a referral might even save a life. Management of IN does not involve a cure, but rather minimization of the intensity, thereby improving the physical appearance, and potentially improving visual function. Management of IN depends on understanding and treating the associated visual system pathology (if any) and maximizing use of the null zone. Small changes in clinical measurements may impact the patient’s visual function significantly. Therefore, it is advantageous for optometrists to have adequate knowledge of the therapies available.
The potential impact of this lifelong condition on the visual function and psychological well-being of those who have it warrants a thorough clinical examination and management. It is well worth providing the patient with a good understanding of their own condition through additional care and attention.
Disclosure
The authors report no conflicts of interest in this work.
References
- ReineckeRDGuoSGoldsteinHPWaveform evolution in infantile nystagmus: An electro-oculo-graphic study of 35 casesBinocul Vis198834191202
- AvalloneJMBedellHEBirchEEA classification of eye movement abnormalities and strabismus20012010(November 18, 2010):Report of a National Eye Institute Sponsored Works Available from http://www.nei.nih.gov/news/statements/cemas.pdf
- SarvananthanNSurendranMRobertsEOThe prevalence of nystagmus: The Leicestershire Nystagmus SurveyInvestig Ophthalmol Vis Sci200950115201520619458336
- HertleRWDell’OssoLFNystagmus in Infancy and ChildhoodNew York, NYOxford University Press2013
- SelfJLoteryAA review of the molecular genetics of congenital idiopathic nystagmus (CIN)Ophthalmic Genet200728418719118161616
- SelfJEShawkatFCrispinMTAllelic variation of the FRMD7 gene in congenital idiopathic nystagmusArch Ophthalmol200712591255126317846367
- ThomasSProudlockFASarvananthanNPhenotypical characteristics of idiopathic infantile nystagmus with and without mutations in FRMD7Brain2008131Pt 51259126718372314
- AbadiRVBjerreAMotor and sensory characteristics of infantile nystagmusBr J Ophthalmol200286101152116012234898
- HertleRWMaldanadoVKMaybodiMYangDClinical and ocular motor analysis of the infantile nystagmus syndrome in the first 6 months of lifeBr J Ophthalmol200286667067512034691
- Dell’OssoLFDaroffRCongenital nystagmus waveforms and foveation strategyDoc Ophthalmol19753911551821201697
- HansonKSBedellHEWhiteJMUkwadeMTDistance and near visual acuity in infantile nystagmusOptom Vis Sci2006831182382917106409
- DickinsonCMThe elucidation and use of the effect of near fixation in congenital nystagmusOphthalmic Physiol Opt1986633033113822471
- GradsteinLGoldsteinHPWizovSSHayashiTReineckeRDRelationships among visual acuity demands, convergence, and nystagmus in patients with manifest/latent nystagmusJ AAPOS19982421822910532740
- AbadiRVDickinsonCMWaveform characteristics in congenital nystagmusDoc Ophthalmol19866421531673608756
- ChamKMAndersonAJAbelLATask-induced stress and motivation decrease foveation-period durations in infantile nystagmus syndromeInvestig Ophthalmol Vis Sci20084972977298418390641
- JonesPHHarrisCMWoodhouseJMMargrainTHEnnisFAErichsenJTStress and visual function in infantile nystagmus syndromeInvestig Ophthalmol Vis Sci201354137943795124222308
- ScheimanMWickBBinocular Vision3rd edPhiladelphia, PALippincot William & Wilkins2008
- FeliusJFuVLNBirchEEHertleRWJostRMSubramanianVQuantifying nystagmus in infants and young children: relation between foveation and visual acuity deficitInvestig Ophthalmol Vis Sci201152128724873122003105
- DunnMJClinical assessment of nystagmusOptom Today20165678085
- GottlobIInfantile nystagmus: development documented by eye movement recordingsInvestig Ophthalmol Vis Sci19973837677739071231
- TheodorouMClementRTaylorDMooreAThe development of infantile nystagmusBr J Ophthalmol201599569169525395685
- LeighRJZeeDSThe Neurology of Eye Movements5th edNew York, NYOxford University Press2015
- FeliusJMuhannaZAVisual deprivation and foveation characteristics both underlie visual acuity deficits in idiopathic infantile nystagmusInvestig Ophthalmol Vis Sci20135453520352523687170
- DunnMJMargrainTHWoodhouseJMEnnisFHarrisCMErichsenJTGrating visual acuity in infantile nystagmus in the absence of image motionInvest Ophthalmol Vis Sci20145542682268624651552
- HealeyNMcLooneEMahonGJacksonAJSaundersKJMcClel-landJFInvestigating the relationship between foveal morphology and refractive error in a population with infantile nystagmus syndromeInvest Ophthalmol Vis Sci20135442934293923518766
- HealeyNMcClellandJFSaundersKJJacksonAJLongitudinal study of spherical refractive error in infantile nystagmus syndromeOphthalmic {&} Physiol Opt J Br Coll Ophthalmic Opt2014343369375
- SampathVBedellHEDistribution of refractive errors in albinos and persons with idiopathic congenital nystagmusOptom Vis Sci200279529229912035986
- WangJWyattLMFeliusJOnset and progression of with-the-rule astigmatism in children with infantile nystagmus syndromeInvest Ophthalmol Vis Sci201051159460120019374
- FresinaMBenedettiCMarinelliFVersuraPCamposECAstigmatism in patients with idiopathic congenital nystagmusGraefes Arch Clin Exp Ophthalmol201325161635163923456100
- DickinsonCMAbadiRVCorneal topography of humans with congenital nystagmusOphthalmic Physiol Opt1984413136709367
- AbadiRVPascalEVisual resolution limits in human albinismVis Res1991317–8144514471891830
- LoshinDSBrowningRAContrast sensitivity in albinotic patientsAm J Optom Physiol Opt1983603158166 Available from http://www.ncbi.nlm.nih.gov/pubmed/68464936846493
- BedellHELoshinDSInterrelations between measures of visual acuity and parameters of eye movement in congenital nystagmusInvest Ophthalmol Vis Sci19913224164211993594
- HarveyEMDevelopment and treatment of astigmatism-related amblyopiaOptom Vis Sci200986663463919430327
- BarotNMcLeanRJGottlobIProudlockFAReading performance in infantile nystagmusOphthalmology201312061232123823462273
- WongAMFEye Movement DisordersNew York, NYOxford University Press2008
- BedellHEPerception of a clear and stable visual world with congenital nystagmusOptom Vis Sci2000771157358111138830
- LeeAGBrazisPWLocalizing forms of nystagmus: symptoms, diagnosis, and treatmentCurr Neurol Neurosci Rep20066541442016928352
- BricknerRMOscillopsia - A new symptom commonly occurring in multiple sclerosisArch Neurol Psych1936363586589
- KhannaSDell’OssoLFThe diagnosis and treatment of infantile nystagmus syndrome (INS)ScientificWorldJournal200661385139717086344
- GelbartSSHoytCSCongenital nystagmus: A clinical perspective in infancyGraefe’s Arch Clin Exp Ophthalmol198822621781803360350
- WeissAHBiersdorfWRVisual sensory disorders in congenital nystagmusOphthalmology19899645175232726182
- LorenzBGampeEAnalysis of 180 patients with sensory defect nystagmus (SDN) and congenital idiopathic nystagmus (CIN)Klin Monatsbl Augenheilkd200121831211225397
- Dell’OssoLFSchmidtDDaroffRBLatent, manifest latent, and congenital nystagmusArch Ophthalmol1979971018771885 Available from http://www.ncbi.nlm.nih.gov/pubmed/485910485910
- WeissmanBMDell’OssoLFAbelLALeighRJSpasmus nutans. A quantitative prospective studyArch Ophthalmol198710545255283566606
- GottlobIWizovSSReineckeRDSpasmus nutans. A long-term follow-upInvest Ophthalmol Vis Sci19953613276827717499100
- AnsonsAMDavisHMeinJDiagnosis and management of ocular motility disorders3rd edOxfordBlackwell Science Ltd2001
- WangZIDell’OssoLFBeing “slow to see” is a dynamic visual function consequence of infantile nystagmus syndrome: model predictions and patient data identify stimulus timing as its causeVis Res200747111550156017328937
- DunnMJMargrainTHWoodhouseJMErichsenJTVisual processing in infantile nystagmus is not slowInvest Ophthalmol Vis Sci20155695094510126241396
- HertleRWExamination and refractive management of patients with nystagmusSurv Ophthalmol200045321522211094245
- AndersonJLavoieJMerrillKKingRASummersCGEfficacy of spectacles in persons with albinismJ AAPOS20048651552015616497
- AllenEDDaviesPDRole of contact lenses in the management of congenital nystagmusBr J Ophthalmol198367128348366671101
- BiousseVTusaRJRussellBThe use of contact lenses to treat visually symptomatic congenital nystagmusJ Neurol Neurosurg Psychiatry200475231431614742616
- Dell’OssoLFTraccisSContact-lenses and congenital nystagmusClin Vis Sci198833229232
- JayaramachandranPProudlockFAOdedraNGottlobIMcLeanRJA randomized controlled trial comparing soft contact lens and rigid gas-permeable lens wearing in infantile nystagmusOphthalmology201412191827183624811959
- SerraADell’OssoLFJacobsJBBurnstineRACombined gaze-angle and vergence variation in infantile nystagmus: two therapies that improve the high-visual-acuity field and methods to measure itInvestig Ophthalmol Vis Sci20064762451246016723456
- Dell’OssoLFImproving visual acuity in congenital nystagmusNeuro-ophthalmology Symp Univ Miami Bascom Palmer Eye Inst1973798106 Available from http://books.google.co.uk/books?id=xM4EAQAAIAAJ
- StahlJSPlantGTLeighRJMedical treatment of nystagmus and its visual consequencesJ R Soc Med200295523523711983763
- Da CostaACRVLopesMCBNakanamiCRInfluence of head posture on the visual acuity of children with nystagmusArq Bras Oftalmol201477181125076365
- MorrisBSmithVElphickJLawsDECompensatory head posture and neck problems: is there an association? A cohort study of nystagmus patientsEye (Lond)200923227928318344967
- McLeanRJWindridgeKCGottlobILiving with nystagmus: a qualitative studyBr J Ophthalmol201296798198622517800
- PillingRFThompsonJRGottlobISocial and visual function in nystagmusBr J Ophthalmol200589101278128116170116
- SandersJThe UK Nystagmus Network (NN)Semin Ophthalmol20062161
- ThurtellMJLeighRJTherapy for nystagmusJ Neuroophthalmol201030436137121107124
- AndersonJRCauses and treatment of congenital eccentric nystagmusBr J Ophthalmol195337526728113042022
- HertleRWAnningerWYangDShatnawiRHillVMEffects of extraocular muscle surgery on 15 patients with oculo-cutaneous albinism (OCA) and infantile nystagmus syndrome (INS)Am J Ophthalmol2004138697898715629289
- NelsonLBErvin-MulveyLDCalhounJHHarleyRDKeislerMSSurgical management for abnormal head position in nystagmus: the augmented modified Kestenbaum procedureBr J Ophthalmol198468117968006498134
- SpielmannAClinical rationale for manifest congenital nystagmus surgeryJ AAPOS200042677410773804
- ZubcovAAStarkNWeberAWizovSSReineckeRDImprovement of visual acuity after surgery for nystagmusOphthalmology199310010148814978414409
- GräfMDroutsasKKaufmannHSurgery for nystagmus related head turn: Kestenbaum procedure and artificial divergenceGraefe’s Arch Clin Exp Ophthalmol = Albr von Graefes Arch für Klin und Exp Ophthalmol20012395334341
- Dell’OssoLFHertleRWWilliamsRWJacobsJBA new surgery for congenital nystagmus: effects of tenotomy on an achiasmatic canine and the role of extraocular proprioceptionJ AAPOS1999316618210428591
- Dell’OssoLFExtraocular muscle tenotomy, dissection, and suture: a hypothetical therapy for congenital nystagmusJ Pediatr Ophthalmol Strabismus19983542322339713798
- HertleRWDell’OssoLFFitzGibbonEJThompsonDYangDMellowSDHorizontal rectus tenotomy in patients with congenital nystagmus: results in 10 adultsOphthalmology2003110112097210514597515
- WangZIDell’OssoLFPrakashSChenXSmooth-pursuit changes after the tenotomy and reattachment procedure for infantile nystagmus syndrome: model predictions and patient dataJ Pediatr Ophthalmol Strabismus201249529530222074359
- SarvananthanNProudlockFAChoudhuriIDuaHGottlobIPharmacologic treatment of congenital nystagmusArch Ophthalmol2006124691691816769853
- SheryTProudlockFASarvananthanNMcLeanRJGottlobIThe effects of gabapentin and memantine in acquired and congenital nystagmus: a retrospective studyBr J Ophthalmol200690783984316556621
- McLeanRJShethVAbbasAPradeepAProudlockFAGottlobIA randomized controlled crossover trial of gabapentin and memantine in infantile nystagmusAbstracts of the European Neuro-Ophthalmology Society (EUNOS) 12th Meeting201539S43
- PradeepAThomasSRobertsEOProudlockFAGottlobIReduction of congenital nystagmus in a patient after smoking cannabisStrabismus2008161293218306120
- ComerRMDawsonELMLeeJPBaclofen for patients with congenital periodic alternating nystagmusStrabismus200614420520917162442
- McLeanRJGottlobIThe pharmacological treatment of nystagmus: a reviewExpert Opin Pharmacother200910111805181619601699
- StruppMThurtellMJShaikhAGBrandtTZeeDSLeighRJPharmacotherapy of vestibular and ocular motor disorders, including nystagmusJ Neurol201125871207122221461686
- ThurtellMJLeighRJTreatment of nystagmusSemin Neurol201535552252626444397