
Abstract
Purpose
Individuals approaching presbyopia may exhibit ocular symptoms as they contend with visual demands of near work, coupled with natural age-related changes in accommodation. Therefore, accommodation and vergence of 30- to 40-year-old, myopic, soft contact lens wearing subjects with symptoms of asthenopia and no history of using multifocal lenses were evaluated.
Patients and methods
In this prospective, observational study, 253 subjects with asthenopia were evaluated by 25 qualified practitioners, each at a different clinical site. Subjects were 30–40 years in age, had symptoms of soreness, eyestrain, tired eyes, or headaches with near work, regularly performed 2–3 consecutive hours of near work, and were undiagnosed with presbyopia. Amplitude of accommodation (AC) and near point convergence (NPC) were measured with a Royal Air Force binocular gauge. Triplicate push up and push down AC and NPC measures were recorded, and average AC values were compared to those calculated using the Hofstetter formula (HF).
Results
The average AC push up/push down value was significantly better than the HF prediction for this age range (8.04±3.09 vs 6.23±0.80 D), although 22.5% of subjects had mean AC below their HF value (5.36±0.99 D). The average NPC push up/push down value was 12.0±4.69 cm. The mean binocular AC value using the push up measure was significantly better than the push down measure (8.5±3.4 vs 7.6±3.0 D). The mean NPC value using the push up measure was significantly worse than the push down measure (13.0±5.0 vs 11.0±4.7 cm). The most frequent primary diagnosis was ill-sustained accommodation (54%), followed by accommodative insufficiency (18%), and accommodative infacility (12%).
Conclusion
Based upon a standardized assessment of accommodation and vergence, ill-sustained accommodation was the most frequent diagnosis among this population.
Introduction
The digital world has rapidly expanded beyond the desktop computer. In 2015, the Pew Research Center (Washington, DC) reported that nearly two-thirds of Americans owned a smartphone, compared with approximately one-third in 2011.Citation1 With increased use of digital media and decreased digital screen size, the demands on the binocular visual system have also increased. In 2016, almost 90% of Americans were estimated to use digital devices for ≥2 hours each day, and almost 60% for ≥5 hours each day.Citation2 Further, 65% reported experiencing symptoms of digital eyestrain, and 77% of those individuals reported using two or more devices simultaneously. Thirty-two percent of the population in the age range of 35–50 years spends at least 9 hours on digital devices each day, and 63% report symptoms of digital eyestrain.Citation3
The term digital eyestrain describes physical discomfort felt after ≥2 hours in front of digital screens at close to mid-range distance and is characterized by symptoms including neck/shoulder/back pain, eyestrain, headache, blurred vision, and dry eyes.Citation3 However, ocular symptoms such as eyestrain, tired eyes, irritation, redness, blurred vision, and double vision, as well as headaches were reported associated with the use of computers at the end of the last century when computers became standard in the workplace.Citation4–Citation6 This set of symptoms came to be known as “computer vision syndrome” (CVS).Citation7–Citation12 The similarity in symptoms suggests that digital eyestrain and CVS are related if not the same, with the one important difference that digital devices are typically viewed at closer distance than are computer monitors.
Recent studies have identified mechanisms contributing to CVS as decreased blink frequency and blink amplitude, increased tear evaporation rate, and decreased tear film stability.Citation13,Citation14 One important aspect of CVS is the reduction in blink rate under conditions of sustained concentration.Citation15 For example, blink rate in normal, non-lens wearing subjects decreased from nominal 17 blinks per minute at rest down to 4.5 blinks per minute when reading,Citation16 and from 18±5.7 down to 3.6±1.8 blinks per minute during video display viewing.Citation6 This phenomenon is especially significant for contact lens wearers because the resultant tear film disruption leads to visual aberration, due to both altered light refraction through the lens and lens dehydration that in itself alters lens geometry.Citation17 Not surprisingly, the incidence of CVS is greater in lens wearers, especially after 6 hours of computer use.Citation18 The use of other digital technologies with flat-panel displays such as cell phones, tablets, and e-readers is likewise associated with the symptoms of CVS.Citation3,Citation19
While blink activity contributes to digital eyestrain, prolonged exposure to near objects challenges the accommodative convergence system.Citation10,Citation20 Further, the accommodative system has been known to decline with age for at least a century and a half.Citation21 Well before the introduction of the first personal computer, Hofstetter published his eponymous formula to calculate the mean, minimum, and maximum amplitude of accommodation (AC) for different age groups,Citation22 based upon his analysis of normal AC values that others published previously, in 1864 (130 subjects, 10–80 years of age)Citation21 and 1912 (4,200 subjects, 8–72 years of age).Citation23 With increased age, the interval between 35 and 44 years has been described as the incipient phase of presbyopia, in which the AC becomes progressively reduced and leads to the eventual need for near addition interventions.Citation24 The lack of near addition correction among patients in the early stages of presbyopia was found to be a risk factor for ocular complaints among those with longer daily durations of demanding computer work.Citation25
The interaction between accommodation and vergence is also challenged during this age.Citation26 Similar to age-related changes in AC, heterophoria and fixation disparity are reported to increase with age (in the exo direction).Citation27 In a population of 2,433 individuals ranging from 10 to 86 years of age, near point convergence (NPC) increased with age over the entire range of the population studied, the sharpest changes occurring between the 30 to 39-year-old and the 40 to 49-year-old age old groups.Citation28 While not intending to evaluate the effect of age, Siderov et al nonetheless measured and compared NPC of non-presbyopic and presbyopic subjects and found 2× greater NPC in the latter group.Citation29 They also speculated that differences between NPC (break) and NPC (recovery) in presbyopes may reflect age-related differences in vergence dynamics. Spierer and Hefetz followed 100 individuals over a 20-year period and found an increase in NPC as subjects became pre-presbyopic (as they reached 34–38 years of age).Citation30
Accommodative and vergence dysfunctions are a diverse group of anomalies that have a similar symptomatic profile to those reported as digital eyestrain. Common symptoms associated with accommodative and vergence anomalies include blurred vision, headache, ocular discomfort, ocular or systemic fatigue, diplopia, motion sickness, and loss of concentration while performing a task.Citation31 Individuals approaching presbyopia may exhibit ocular symptoms as they contend with the visual demands of digital device viewing and other near work, coupled with natural age-related changes in accommodation. The exact cause of these symptoms is not well understood.
The objectives of this prospective, single-arm, observational study were first to evaluate and characterize the accommodation and vergence of a large population of 30 to 40-year-old myopic subjects who both used technology or performed other near-work tasks and reported symptoms of asthenopia (including burning, irritated, tearing, red, dry, and tired eyes, blurred vision and double vision, as well as sore or aching eyes, eye fatigue, muscle stress inside the eye, muscle stress around the eye, and headache) with no history of using multifocal lenses, and second to compare the measured accommodation values to those predicted by the Hofstetter formula (HF) proposed over a half century ago.Citation22 As little such data appear in published literature, especially in the current age of digital devices, the results obtained with this relatively large population across multiple investigation centers provide insight into the relationships between age, CVS, and accommodative dysfunction.
Materials and methods
This study was reviewed and approved by Southwest Independent Institutional Review Board (Fort Worth, TX, USA). Written approval of the protocol, informed consent form, and subject instructions were provided prior to initiation of the study. Eligible subjects gave written informed consent and complied with the study procedures.
Study design and population
Pre- and early-presbyopic, soft contact lens wearing subjects who reported symptoms of asthenopia were recruited and evaluated in this prospective study conducted in the United States. Twenty-five investigators, each at a different clinical site, enrolled a total of 253 subjects in the study. Eligible male and female subjects, 30–40 years of age, were myopic soft contact lens wearers with clear central corneas free from anterior segment disorders. All regularly performed at least one of the following activities daily for 2–3 hours without a break: computer use, cell phone use for games, maps, or Internet search, other handheld device use, reading, or hobbies that require midrange or close-up vision. In addition, all subjects experienced at least one of the following, four times a week as a result of these activities: eyestrain, tired eyes, headaches with near work, or soreness, ache, or pain inside the eyes. Individuals who required monovision, multifocal, or toric contact lenses or who had been diagnosed with presbyopia were not eligible to participate.
Outcomes evaluated
All testing was conducted with subjects using their habitual soft contact lenses. To ensure uniform testing, all study site investigators were trained on the use of the study instruments using the same standard clinical protocol. AC and NPC were measured with a Royal Air Force (RAF) binocular gauge. The RAF gauge and a metronome were used to regulate movement of the target. The box was moved slowly toward the subject at a rate of ~2 cm per second. Three push up and push down AC and NPC measures were recorded in triplicate (three measurements in each eye for each of the measures), and average AC values were compared to those predicted by the HF.Citation22 Near heterophoria was measured by Maddox Wing test, which was selected because it is repeatable across study sites. Investigators diagnosed primary accommodation/vergence dysfunction using the Optometric Clinical Practice Guidelines of the American Optometric AssociationCitation31 ().
Table 1 Summary of accommodation/vergence dysfunction classifications and descriptions
Statistical analysis
All statistical analyses were conducted using the SAS statistical analysis package (version 9.1; SAS Institute Inc, Cary, NC, USA). All continuous variables are summarized as means and standard deviations. AC push up/push down measurements were compared to the Hofstetter predicted values using Student’s t-test. Paired t-test was employed to compare the push up values against push down values from the same subjects for AC and NPC, respectively. Two-tailed tests were used for all comparisons. p-values <0.05 were designated statistically significant.
Results
Twenty-five investigators enrolled a total of 253 subjects in the study. The average subject age was 35.0±3.2 years (mean ± standard deviation). The subjects ranged in age from 30 to 40 years, with a median age of 35.0 years. Of the 253 subjects enrolled, 79.6% were female and 20.4% male; 80.8% were Caucasian, 10.9% Black/African-American, 6.8% Asian, 0.8% American Indian/Alaskan Native, and 0.8% other. All recruited subjects were adapted, soft contact lens wearers. The predominance of females in the study population did not occur by design but rather likely reflects the greater number of female than male contact lens wearers in the United States. The mean refraction sphere was −3.27±1.6 D, with a range from −0.25 to −7.00 D. The mean refraction cylinder was −0.35±0.28 D, with a range from 0.00 to −1.00 D.
The average AC push up/push down value (8.04±3.09 D) was significantly better than what the HF would predict for this age range (6.23±0.80 D, p<0.0001, ). However, 67 of the 253 subjects (26.5%) had AC below their predicted HF values with their habitual lenses. The mean AC push up/push down value for these 67 subjects was 5.51±1.02 D. The mean binocular AC value using the push up measure (8.5±3.4 D) was significantly better than the push down measure (7.6±3.0 D, p<0.0001, ).
Table 2 Average amplitude of accommodation compared to predicted values from Hofstetter formula
Table 3 Comparison of average push up and push down values for AC and NPC
The average NPC push up/push down value was 12.0±4.69 cm. The mean NPC value using the push up measure (13.0±5.0 cm) was significantly worse than the push down measure (11.0±4.7 cm, p<0.0001, ). Among subjects with horizontal (n=209) and vertical (n=20) near phorias, the means were 0.92±3.16 D for exophoria and 0.60±1.35 D for right hyperphoria, respectively ().
Table 4 Summary of horizontal and vertical phoria measures
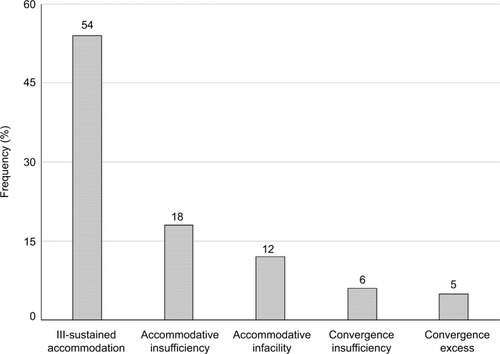
The most frequent investigators-diagnosed primary accommodation/vergence dysfunction diagnosis for asthenopic symptoms was ill-sustained accommodation (54%), followed by accommodative insufficiency (18%), and accommodative infacility (12%) (). Convergence insufficiency (6%) and excess (5%) were less frequent.
Figure 1 Primary diagnosis for asthenopic symptoms among adults aged 30–40 years.
Discussion
Accommodative function begins to decline as early as age 10 and continues to decline with age.Citation32 This may be related to ocular symptoms such as eyestrain, tired eyes, irritation, redness, blurred vision, double vision, and headaches that have been reported with the use of computers and other digital devices, aka CVS.Citation7–Citation12 Individuals approaching presbyopia typically own multiple digital devices and spend prolonged amounts of time using them on a daily basis.Citation3
This observational clinical study of accommodative and vergence dysfunction resulting from digital device use and other near work was conducted to characterize the asthenopic symptoms in a large clinical population, since most recent clinical studies reported in published literature are of relatively smaller populations than the 253 subjects evaluated in this study. Such dysfunction is classified in as accommodative insufficiency, ill-sustained accommodation, accommodative infacility, convergence insufficiency, and convergence excess. In this study of 30 to 40-year-old soft contact lens wearers with asthenopia, ill-sustained accommodation, which is characterized by a normal AC but fatigue with repeated accommodative stimulation,Citation31 was the most common primary diagnosis (). While ill-sustained accommodation in this age group while viewing digital technology is not surprising, it is not well discussed in published academic literature, and this may be the first study to document the high incidence of such dysfunction in early-presbyopes.
NPC in the present study (13.0±5.0 cm push up/11.0±4.7 cm push down) was greater than that reported previously as measured using a 6/12 single target on a Gulden fixation stick (8.30±3.9 cm push up in a 30 to 39-year-old population).Citation28 Both of these populations presented NPC greater than those of a single population of 100 individuals in which NPC was measured annually beginning in the 1970s for 20 consecutive years before common use of digital devices (6.3±0.8 cm at 18–22 years of age, compared with 6.8±1.3 cm at 34–38 years of age).Citation30
The mean phoria in the present study was exophoria, with low hyperphoria reported in a subset of the study cohort. Measured values () were within the 0.78–2.33 range reported by Collier and Rosenfield,Citation20 who found decreased CVS symptoms in patients with low amounts of exophoria compared with zero phoria. However, near vision fatigue has also been associated with greater exo-fixation disparity.Citation33 As phoria values measured in this study were in the normal range, it is apparent that the accommodation system rather than vergence system is the primary driver of asthenopia in the present study population.
Changes in AC during aging are understood in presbyopia.Citation24 To quantitate accommodative changes during aging, Hofstetter analyzed historical data published in the mid-19thCitation21 and early 20thCitation23 centuries to develop formulas to predict minimum, probable, and maximum AC.Citation22 Noteworthy is that the historical data were collected before common electric lighting, decades before Hofstetter’s analysis, before television became commonplace, and over a century before the current digital device age.
Measured AC values in the present study population were better than the HF predicted values (6.23±0.80 D), with average push up/push down values of 8.04±3.09 D (). In comparison, Spierer and Hefetz measured lower AC of 5.5±1.5 D in a population of 18 to 22-year-old subjects.Citation30 Win-Hall and Glasser measured a lower average AC of 4.76±1.32 D, with a range of 3.33–8.59 D in a study of 15 pre-presbyopic subjects aged 38–49 years.Citation34 The Win-Hall and Glasser study measured accommodation using both WR-5100K open-field autorefractor and iTrace aberrometer instruments at a single study site. Data reported in the present study were collected from 253 subjects by 25 investigators, each using the same standardized technique employing an RAF gauge and metronome to regulate movement of the target. Differences between the studies might be attributed to the differences in the respective age groups and likely also reflect differences in study design, technique, and sample size. It should be noted that digital display use pervasive in today’s society was but a concept during the time of Spierer and Hefetz’s study and had just begun to be widely adopted at the time of Win-Hall and Glasser’s study.
While differences between study protocols may in part explain differences between study results, HF itself may not accurately predict AC values in the pre-presbyopic age group. The formula is based upon analysis of historical data measured in subjects of all ages, including children, younger adults, pre-presbyopic adults, and presbyopic adults. A recent clinical study suggests that HF inaccurately predicts AC values in children,Citation35 which implies that Hofstetter should have excluded measurements taken in children when calculating the constants in his formula. We speculate that the formula might make more accurate predictions if different sets of constants are calculated for different age groups (young child, youth child, young adult, pre-presbyopic adult, and presbyopic adult).
Hofstetter’s own studies of convergenceCitation36 were conducted during the nascent golden age of (analog) television. The effects of black and white versus color and analog versus digital images upon accommodation are beyond the scope of this study but may be important when comparing studies from different eras and may in part explain the differences between measured data and HF predictions.
Another marked difference between eras that may affect the decline in accommodation is life expectancy. The average life expectancy in the United States was 47.3 years in 1900, compared with 68.2 years in 1950 and 77.9 years in 2007.Citation37 The disparity between results of the present study and Hofstetter’s prediction might also imply that age-related patterns of lost accommodative function changed over the years as life expectancy increased, with those born at the turn of the last century facing presbyopia shortly before death and those born today living nearly as long with presbyopia as without. Alternatively, the HF has never been validated rigorously by clinical trial and may be inherently less accurate than commonly assumed.
Accommodation values in the present study fell within the higher range reported by Cheng et al, perhaps due to technique differences, or to the slightly older population in that study.Citation38 Push up values in the present study were better than push down values, in agreement with Antona et al.Citation39 Others have also reported a difference between push up and push down measurements; a suggested compromise has been to average the push up and push down values to account for differences in the techniques.Citation40
This large observational study supports the hypothesis that habitual use of modern digital devices and other near work exacerbates accommodative dysfunction in pre- and early-presbyopes wearing contact lenses. However, as the study was observational and lacked control groups, further clinical evaluation is needed to confirm this finding, as well as to elucidate if the observed effects can be attributed primarily to one or two dominant variables (eg, degree of myopia, particulars of contact lenses wear, duration of screen use, etc).
Increased computer usage and resulting symptoms motivated development of potential treatments and therapies, such as vision therapy or exercises to relax the accommo-dative response and relieve symptoms of eyestrain.Citation41 The ergonomics of work environments have also been evaluated to determine whether better working conditions, such as improved lighting or screen filters, might be helpful.Citation42,Citation43 In addition, refractive lens options such as computer vision or progressive glasses, antiglare-treated lenses, and filtered lenses, as well as multifocal contact lenses may help relieve symptoms of asthenopia.Citation2,Citation44 Glasses designed to stimulate blinking during computer use have also been reported.Citation45 Under some conditions, the type of display and font size of the handheld device can be adjusted to provide a better viewing experience.Citation46 Physiological factors such as dry eye and blink response also contribute to the symptoms and are considered potential areas of treatment.Citation10
Visual displays must also be considered in the context of sensitivity to blur. Some display characteristics can affect the amount of rendered image blur, which plays a role in accommodation as it increases at larger or smaller depths, thereby contributing to the depth of field. Blur also serves as a cue for accommodation; thus, when there are large fluctuations in accommodation, discomfort can arise from visual fatigue.Citation47
Optical blur has also been studied relative to aberrations, as both low and high order aberrations result in blurred images formed by the eye.Citation48 Some studies suggest that controlling aberrations might aid the accommodation system.Citation38,Citation49–Citation52 For example, Cheng et al reported that accommodation was accompanied by concurrent changes in aberration, with spherical aberration (SA) showing the greatest change with accommodation.Citation38 Additional studies are needed to understand the implications of SA correction in pre- and early-presbyopia, and to investigate the optimal amount of SA in this age group.
As technology demands on vision continue to increase, the accommodative burden and resulting symptoms will increase and become of greater clinical interest. Surveys show that devices with ever-decreasing screen sizes are becoming increasingly popular across age groups, and as early as childhood.Citation1,Citation2 Understanding the influence of these technologies on the accommodative burden can aid in the development of treatments, therapies, and refractive lens options. As reported in the present study, ill-sustained accommodation was the most frequent primary diagnosis among this 30 to 40-year-old population. These outcomes underscore the importance of providing a comprehensive binocular vision assessment in current patient populations, and assessing near vision demands relative to near work and multiple digital platforms such as smart phones, tablets, e-readers, and computers. Further clinical studies to determine if accommo-dative dysfunction during contact lens wear observed in this study is a consequence of digital display use or near work, a concomitant effect of other causes or symptoms of CVS, or something else entirely, are warranted.
Conclusion
Demands on the binocular visual system are certain to increase as the use of digital media increases and the size of digital screens decreases. The use of digital media by pre- and early-presbyopic populations has grown with the introduction of new devices. Based upon the standardized assessment of accommodation and vergence, ill-sustained accommodation was the most common diagnosis among this relatively large population of 30 to 40-year-old myopic, adapted, soft contact lens wearing subjects with symptoms of asthenopia, while vergence dysfunction was less prevalent. As near vision demands of digital media increase, the importance of comprehensive binocular vision assessment also increases.
Acknowledgments
The authors would like to thank Suzie Webster for her contributions to the manuscript.
The abstract of this paper was presented at the Annual Meeting of the American Academy of Optometry held at San Francisco, CA, USA on November 17–20, 2010 as a poster presentation (program number 105221) with interim findings. The poster’s abstract was published online and is available for download at https://www.aaopt.org/detail/knowledge-base-article/evaluation-binocular-function-among-preearly-presbyopes-asthenopia.
Disclosure
William Reindel and Marjorie Rah are employees of Bausch & Lomb Inc; Lening Zhang was an employee of Bausch & Lomb Inc at the time of the study; and Joseph Chinn is a paid consultant to Bausch & Lomb Inc. The authors report no other conflicts of interest in this work.
References
- Pewinternet.org [homepage on the Internet]U.S. smartphone use in 2015Washington, DCPew Research Center2015 [updated April 1, 2015; cited February 1, 2017]. Available from: http://www.pewinternet.org/2015/04/01/us-smartphone-use-in-2015/Accessed September 1, 2017
- The Vision CouncilOverexposed: the digital device dilemma2016Digital eye strain reportAlexandria, VAThe Vision Council2016 [cited February 1, 2017]. Available from: https://visionimpactinstitute.org/wp-content/uploads/2016/03/2016EyeStrain_Report_WEB.pdfAccessed November 27, 2017
- The Vision CouncilHindsight is 20/20/20: protect your eyes from digital devices2015Digital eye strain reportAlexandria, VAThe Vision Council2015 [cited February 1, 2017]. Available from: http://www.pcom.ph/sites/default/files/downloads/vc_digitaleyestrain_report2015.pdfAccessed November 27, 2017
- EichenbaumJWComputers and eyestrainJ Ophthalmic Nurs Technol199615123268715024
- TsubotaKNakamoriKDry eyes and video display terminalsN Engl J Med19933288584
- PatelSHendersonRBradleyLGallowayBHunterLEffect of visual display unit use on blink rate and tear stabilityOptom Vis Sci199168118888921766652
- SheedyJWhat’s in a name: “computer vision syndrome ”?Optometry200273739940212365656
- American Optometric AssociationThe effects of computer use on eye health and visionSt Louis, MOAmerican Optometric Association1997 [cited February 1, 2017]. Available from: http://www.aoa.org/Documents/optometrists/effects-of-computer-use.pdfAccessed September 1, 2017
- Von StrohRComputer vision syndromeOccup Health Saf199362106266
- RosenfieldMComputer vision syndrome: a review of ocular causes and potential treatmentsOphthalmic Physiol Opt201131550251521480937
- GowrisankaranSSheedyJEComputer vision syndrome: a reviewWork201552230331426519133
- BlehmCVishnuSKhattakAMitraSYeeRWComputer vision syndrome: a reviewSurv Ophthalmol200550325326215850814
- WolkoffPNøjgaardJKTroianoPPiccoliBEye complaints in the office environment: precorneal tear film integrity influenced by eye blinking efficiencyOccup Environ Med200562141215613602
- CardonaGGarcíaCSerésCVilasecaMGispetsJBlink rate, blink amplitude, and tear film integrity during dynamic visual display terminal tasksCurr Eye Res201136319019721275516
- GowrisankaranSNaharNKHayesJRSheedyJEAsthenopia and blink rate under visual and cognitive loadsOptom Vis Sci20128919711022051780
- BentivoglioARBressmanSBCassettaECarrettaDTonaliPAlbaneseAAnalysis of blink rate patterns in normal subjectsMov Disord1997126102810349399231
- SchaferJSteffenRReindelWChinnJEvaluation of surface water characteristics of novel daily disposable contact lens materials, using refractive index shifts after wearClin Ophthalmol201591973197926543349
- TausteARondaEMolinaMJSeguíMEffect of contact lens use on computer vision syndromeOphthalmic Physiol Opt201636211211926743161
- PorcarEPonsAMLorenteAVisual and ocular effects from the use of flat-panel displaysInt J Ophthalmol20169688188527366692
- CollierJDRosenfieldMAccommodation and convergence during sustained computer workOptometry201182743444021514899
- DondersFCMooreWDOn the Anomalies of Accommodation and Refraction of the Eye: With a Preliminary Essay on Physiological DioptricsLondonNew Sydenham Society1864
- HofstetterHWThe relationship of proximal convergence to fusional and accommodative convergence. Useful age-amplitude formulaOptom World1950384245
- DuaneANormal values of the accommodation at all agesJAMA1912591210101013
- PointerJSGilmartinBPatterns of refractive change in myopic subjects during the incipient phase of presbyopia: a preliminary studyOphthalmic Physiol Opt201131548749321410500
- JaschinskiWKönigMMekontsoTMOhlendorfAWelscherMComputer vision syndrome in presbyopia and beginning presbyopia: effects of spectacle lens typeClin Exp Optom201598322823325963113
- VedamurthyIHarrisonWWLiuYCoxISchorCMThe influence of first near-spectacle reading correction on accommodation and its interaction with convergenceInvest Ophthalmol Vis Sci20095094215422219264892
- YektaAAPickwellLDJenkinsTCBinocular vision, age and symptomsOphthalmic Physiol Opt1989921151202622645
- OstadimoghaddamHHashemiHNabovatiPYektaAKhabazkhoobMThe distribution of near point of convergence and its association with age, gender and refractive error: a population-based studyClin Exp Optom2017100325525927652584
- SiderovJChiuSCWaughSJDifferences in the near point of convergence with target typeOphthalmic Physiol Opt200121535636011563422
- SpiererAHefetzLNormal heterophoric changes: 20 years’ follow-upGraefes Arch Clin Exp Ophthalmol199723563453489202961
- CooperJSBurnsCRCotterSADaumKMGriffinJRScheimanMMOptometric clinical practice guideline. Care of the patient with accommodative and vergence dysfunctionSt Louis, MOAmerican Optometric Association1998 Revised 2010 [cited February 1, 2017]. Available from: http://www.aoa.org/documents/optometrists/CPG-18.pdfAccessed September 1, 2017
- CristarellaMCVisual functions of the elderlyAm J Occup Ther1977317432440888904
- JaschinskiWThe proximity-fixation-disparity curve and the preferred viewing distance at a visual display as an indicator of near vision fatigueOptom Vis Sci200279315816911913842
- Win-HallDMGlasserAObjective accommodation measurements in prepresbyopic eyes using an autorefractor and an aberrometerJ Cataract Refract Surg200834577478418471632
- HashemiHNabovatiPKhabazkhoobMYektaAEmamianMFotouhiADoes Hofstetter’s equation predict the real amplitude of accommodation in children?Clin Exp Optom Epub2017517
- HofstetterHWThe relationship of proximal convergence to fusional and accommodative convergenceAm J Optom Arch Am Acad Optom195128630030814838099
- Life expectancy at birth, at age 65, and at age 75, by sex, race, and Hispanic origin: United States, selected years 1900–2010Atlanta, GACenter for Disease Control/National Center for Health Statistics/Office of Analysis and Epidemiology2010 [cited July 1, 2017]. Available from: https://www.cdc.gov/nchs/data/hus/2010/022.pdfAccessed September 1, 2017
- ChengHBarnettJKVilupuruASA population study on changes in wave aberrations with accommodationJ Vis20044427228015134474
- AntonaBBarrraFBarrioAGonzalezESanchezIRepeatability intraexaminer and agreement in amplitude of accommodation measurementsGraefes Arch Clin Exp Ophthalmol2009247112112718791730
- RosenfieldMLoganNEdwardsKOptometry: Science, Techniques, and Clinical Management2nd edEdinburghButterworth–Heinemann-Elsevier2009
- OmoriMWatanabeTTakaiJAn attempt at preventing asthenopia among VDT workersInt J Occup Saf Ergon20039445346214675518
- MuttiDOZadnickKIs computer use a risk factor for myopia?J Am Optom Assoc19966795215308888885
- SheedyJEThe bottom line on fixing computer-related vision and eye problemsJ Am Optom Assoc19966795125178888881
- Aoa.org [homepage on the Internet]5 tips for multifocal contact lens successSt Louis, MOAmerican Optometric Association2016 [updated February 9, 2016; cited February 1, 2017]. Available from: http://www.aoa.org/news/clinical-eye-care/5-tips-for-multifocal-contact-lens-success?sso=yAccessed September 1, 2017
- AngCKMohidinNChungKMEffects of wink glass on blink rate, nibut and ocular surface symptoms during visual display unit useCurr Eye Res201439987988425014251
- GillKMaoAPowellAMSheidowTDigital reader vs print media: the role of digital technology in reading accuracy in age-related macular degenerationEye (Lond)201327563964323492860
- O’HareLHibbardPBVisual discomfort and blurJ Vis20131357
- SawidesLDorronsoroCHaunAMPeliEMarcosSUsing pattern classification to measure adaptation to the orientation of high order aberrationsPLoS One201388e7085623967123
- AllenPMRakhakrishmanHRaeSAberration control and vision training as an effective means of improving accommodation in individuals with myopiaInvest Ophthalmol Vis Sci200950115120512919643961
- KhalifaMAAllamWAKhalifaAMImproving near vision in presbyopic eyes by selective treatment of high-order aberrationsClin Ophthalmol201151525153022069357
- GambraESawidesLDorronsoroCMarcosSAccommodative lag and fluctuations when optical aberrations are manipulatedJ Vis2009964
- TheagarayanBRadhakrishnanHAllenPMCalverRIRaeSMO’LearyDJThe effect of altering spherical aberration on the static accommodative responseOphthalmic Physiol Opt2009291657119154282