
Abstract
Purpose
To compare the biomechanically-corrected intraocular pressure (bIOP) measured by the Corvis ST (Oculus, Wetzlar, Germany) with IOP measurements made by other commonly used tonometers; and to test the correlations between IOP measures and central corneal thickness.
Methods
One randomly-selected eye from each of 94 healthy subjects was assessed. The bIOP was determined by the CorVis ST and compared with the IOP measurements made by standard Goldmann Applanation Tonometer (GAT: Haag-Streit AG, Bern, Switzerland), the Icare (Icare Finland Oy, Vantaa, Finland), and the Ocular Response Analyzer (ORA-IOPcc: Reichert, New York, USA). Corneal thickness was assessed by the Oculus Pentacam. The correlation between bIOP and the other devices and between CCT were assessed using the Pearson correlation test or Spearman’s rho test accordingly to the distribution of these values. The Bland-Altman method and intraclass correlation coefficients (ICC) were used to assess the agreement of bIOP results with IOP obtained with other techniques. The limits of agreement (LoA) were determined as the mean difference ±1.96 SD of the mean differences. In all tests, the significance level was considered to be 0.05.
Results
Mean and SD of the bIOP were 16.11±1.66 mmHg. Significant differences were found between the bIOP and other IOP measurements (GAT, 3.02±2.60 mmHg, p<0.001, Icare, 1.51±2.95 mmHg, p<0.001, IOPcc, 1.09±1.96 mmHg, p<0.001). The lowest and highest mean differences in IOP were with the IOPcc and GAT, respectively. Interestingly, there were no significant differences in bIOP, GAT-IOP and ORA-IOPcc between the eyes with thin or thick corneal thicknesses, with Icare-IOP being the only exception (p<0.001).
Conclusion
The Corvis bIOP has a higher correlation with the IOPcc by ORA, which are also compensated for the effects of corneal biomechanics and have less association with corneal thickness relative to the uncorrected GAT and Icare measurements.
Background
Although interactions between intraocular pressure (IOP) and the biomechanics of the eye have been reported widely,Citation1,Citation2 IOP measurements that are not corrected for the effects of biomechanics are still commonly used in screening, diagnosis and follow-up of patients with glaucoma. Several tonometers have been introduced for measuring IOP, some of which were intended to address the biomechanics influence on IOP measurements.Citation3 These include the Goldmann applanation tonometer (GAT), and non-contact tonometers such as the Ocular Response Analyzer (ORA)Citation4,Citation5 and the Corvis ST,Citation6 all based on the applanation principle.
The GAT has been considered the reference standard for IOP measurement since its development in the 1950s.Citation7 Its design assumes a central corneal thickness (CCT) value of 520 µm, so the IOP measurement will be affected if a patient’s CCT is different from this value.Citation8 Earlier studies have shown that not only the CCT but other geometrical and material parameters related to corneal stiffness should be considered in order to produce IOP measurements that were free of the effects of biomechanics.Citation9–Citation11
Variations in biomechanical properties of the cornea have different effects on the measurement of IOP depending on the design of the tonometry device used. Therefore, changes in these corneal properties can lead to different extents of over- or underestimation of the IOP and may ultimately lead to wrong diagnosis or management of patients with glaucoma or ocular hypertension.Citation12
The Icare tonometer is based on the principle of rebound measurement (RBT: Rebound Tonometer) and uses a probe for instantaneous mild contact with the cornea.Citation13–Citation15 In this situation, IOP is determined by the contact time with the cornea and the retardation in the speed of the probe.Citation13–Citation15
There are currently two devices available for in vivo assessment of corneal biomechanical parameters in the clinic, the Ocular Response Analyzer (ORA, Reichert Ophthalmic Instruments, Buffalo, NY, USA) and CorVis ST (Oculus Optikgeräte GmbH, Wetzlar, Germany) have been introduced for in vivo evaluation of the corneal biomechanics.Citation16 The newer device is OCULUS Corvis® ST, which integrates tonometry and pachymetry data with the corneal biomechanical response of the cornea. Assessing these parameters allows Corvis ST to correct for both factors and provide a biomechanically corrected IOP (bIOP), which has been shown clinically and experimentally to be less affected by corneal thickness and age than GAT and the uncorrected Corvis IOP readings.Citation3 Also, in cases with altered biomechanical properties such as following kerato-refractive surgeries or cross-linking; the bIOP was able to provide similar IOP readings that were similar to the pre-surgery estimations.Citation17–Citation20 Given that corneal biomechanical properties influence IOP measurement, and with recent evidence that the bIOP exhibits the least affected IOP measurement by corneal biomechanics,Citation21 this study was designed to compare the bIOP with IOP measured with other commonly-used tonometers to see how can these tonometers provide an IOP close to the actual IOP for diagnostic and therapeutic purposes in the clinic.
Methods
Ninety-four normal eyes were assessed in this retrospective clinical study. All stages of this study were conducted according to the tenets of the declaration of Helsinki. In addition, written informed consent was obtained from all subjects and the study was approved by the ethics committee of Mashhad University of Medical Sciences. (Code Number: 960298)
Inclusion criteria were healthy eyes with no history of ocular and systemic diseases or medications that affect IOP, spherical equivalent (SE) ≤4.00 diopters and corneal astigmatism less than 3.00 diopters.
The eyes with any type of glaucoma, corneal dystrophy, keratoconus or keratoconus suspected, history of previous kerato-refractive surgery or glaucoma surgery, systemic disease (diabetes mellitus, blood hypertension, and connective tissue diseases), moderate to severe dry eye syndrome and history of contact lens use were excluded from the study. Another exclusion criterion was pregnancy.
The eyes were subjected to routine ophthalmic examinations including refractive assessments using auto-keratorefractometer (Topcon Corp., Tokyo, Japan), slit-lamp biomicroscopy and fundus examination. Also, Scheimplfug tomography with Pentacam HR (Oculus; Wetzlar, Germany) was used for measuring the corneal thickness at the corneal apex or center (CCT). In subsequent analysis, the corneas were divided into two groups with a small thickness (CCT <540 µm) and large thickness (CCT ≥540 µm) similar to an earlier study.Citation22
IOP was measured using four techniques including two contact tonometers; the Goldmann Applanation Tonometer (GAT: Haag-Streit AG, Bern, Switzerland), the reference standard in tonometry,Citation23 and the Icare (Icare® TA01i, I-Care Finland Oy, Finland), one of the most commonly used tonometers in clinical practice.Citation14 Two non-contact IOP measurements were also obtained including the cornea-compensated IOP (IOPcc) by the Ocular Response Analyzer (ORA: Reichert Ophthalmic Instruments, New York, USA)Citation24 and the biomechanically-corrected IOP (bIOP) by the Corvis ST (Oculus, Wetzlar, Germany), both of which were intended to be significantly less dependent on corneal stiffness than the GAT.Citation12 The repeatability of IOP measurements by these four tonometers have been confirmed in earlier studies.Citation9,Citation19–Citation24
The uncorrected Corvis ST IOP measurements (IOPnct) and the Goldmann-correlated IOP (IOPg) produced by the ORA were collected during the study but not used in the analysis as they were not corrected for the effects of biomechanics.Citation21,Citation25
As IOP assessment with GAT was done following local anesthetics with Tetracaine 1%, GAT was always used last. IOP measurement using the other devices where anesthesia was not needed was done randomly. While IOP was measured using GAT and Icare by an experienced ophthalmologist (MRS), tonometry with ORA, and Corvis ST was performed by a well-trained and experienced operator (NM). All measurements were performed from 4 PM to 6 PM to ensure the stability of the results,Citation26 and were taken with the participants in a sitting position. A rest time of five minutes was adopted between measurements to ensure recovery from the aqueous outflow.Citation27
Data were analyzed in SPSS.17 software (SPSS.Inc, Chicago, USA). Assessment of the normal distribution of quantitative data was done using the Kolmogorov–Smirnov test. The repeated measures ANOVA (or within-subject ANOVA analysis) was used to compare the mean IOP obtained with different tonometers and the Bonferroni test for pairwise comparison. In this analysis, the dependent variable was IOP and independent variable was the measurement method (or tonometry device). The results were reported using the F-statistic [F(dfmethods, dferror)= F-ratio, p= p-value]. The software calculated the F-ratio by dividing the mean squares for the experimental effects (methods) by the error mean squares. Also, SPSS displays the significance level for the F-ratio. Due to the inhomogeneity of variance the assumption of sphericity was not met, therefore the degrees of freedom (df) were corrected using Greenhouse-Geisser estimates of sphericity. Correlation of bIOP, which was reported to provide more accurate estimates of the true IOP,Citation21 with IOP measurements was assessed using the Pearson correlation test or its non-parametric equivalent. The independent sample t-test or its non-parametric equivalent was used to evaluate the difference in IOP in the thin and thick cornea groups. The Bland-Altman methodCitation28 and Intraclass correlation coefficients (ICC) were used to assess the agreement of bIOP with other IOPs. ICC values of 0–0.2, 0.3–0.4, 0.5–0.6, 0.7–0.8 and more than 0.8 were considered indicators of poor, fair, moderate, strong and near perfect agreements.Citation29 The limits of agreement (LoA) were determined as the mean difference ±1.96SD of the mean differences. In all tests, p-values less than 0.05 were considered significant.
Results
The 94 participants included, twenty-six (27.7%) males and sixty-eight females (72.3%). The mean age was 30.55±6.04 years (range: 20–46 years). The mean IOP measurements and the pairwise comparisons between them are listed in .
Table 1 Mean And Standard Deviation (SD) Of Measured IOP Using Different Tonometers (n=94 Eyes)
shows that the highest IOP was the bIOP (16.11±1.66 mmHg), while the lowest was the GAT (13.08±2.64 mmHg). The lowest and highest standard deviations of measured IOP were related to the bIOP and Icare measurements, respectively, . The results also show a significant difference between mean IOPs obtained with different tonometers (F (2.496, 232.135) = 41.804, p< 0.001), where the Bonferroni test was used for the pairwise comparisons.
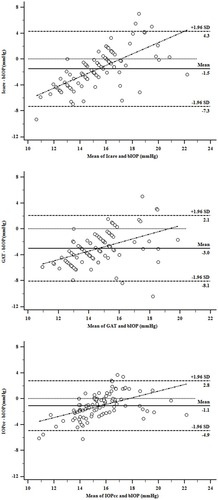
Figure 1 Agreement of the bIOP with the IOP measured using Icare (upper), GAT (middle) and IOPcc (lower). (n=94 eyes) The mean difference is shown by a solid horizontal line, while the 95% limits of agreement, zero mean difference and the regression line are indicated by dashed horizontal and oblique lines, respectively.
With recent evidence presented of bIOP being the least affected IOP measurement by corneal biomechanics,Citation21 Icare, GAT and IOPcc readings were compared to the bIOP in .
Table 2 Mean And Range Of Differences Between bIOP And Other IOP Measurements In mmHg, And 95% Limits Of Agreement (n= 94 Eyes)
shows that the least mean difference (−1.09 mmHg) and the highest agreement (±3.84) with bIOP were related to the IOPcc, which was intended to correct for corneal stiffness.Citation3,Citation30 With attention to ICC, the least agreement with bIOP was with GAT and the strongest agreement was with IOPcc. Also, there was a significant correlation between IOP measurements with the Icare, GAT, and IOPcc with bIOP using the Spearman correlation test. (p< 0.05)
”Further, Bland-Altman plots demonstrate the mean IOP difference between the two tonometers as a function of the mean IOP of these two devices. In other words, the IOP difference between each two tonometers and the bIOP was plotted against the mean of the same tonometer’s IOP measurements and the bIOP. () In each plot, the mean difference between the two methods is marked with a horizontal solid line, while the 95% limits of agreement and regression line are marked with horizontal and oblique dashed lines, respectively.
: It is apparent that in all plots, more than 95% of the difference between bIOP and the IOP measured with other tonometers was within ±2SD of the mean difference in IOP with two methods. The lowest agreement band or the highest agreement with bIOP was obtained with IOPcc. Also, the highest percentage of zero mean difference (5.4%) was related to the results of bIOP and IOPcc.
The correlation results of different IOPs with the central corneal thickness (CCT) obtained by the Pentacam were Icare: rs= 0.355, p= 0.003, GAT: rs= 0.177, p= 0.087, bIOP: rs= 0.125, p= 0.231, and IOPcc: r= 0.210, p= 0.042. These results show that IOP measurements by Icare and IOPcc were significantly correlated with CCT, unlike GAT and bIOP. Further analysis of these results, which considers the mean IOP with different tonometers in thin (<540 µm) and thick (≥540 µm) corneas, is presented in .
Table 3 Mean And Standard Deviation Of IOP (mmhg) In Small (<540 µm) And Large (≥540 µm) Central Corneal Thickness (n=94)
shows a significant difference in IOP measured in thin and thick corneas with Icare (p= 0.001) while GAT, bIOP and IOPcc did not show significant differences in measured IOP in corneas with a small and large thickness. (p> 0.05) The highest difference in measured IOP was with Icare (2.10 mmHg), while the lowest differences were with GAT (0.63 mmHg) and bIOP (0.77 mmHg).
Discussion
This study showed that among the measured IOPs; the least variation based on the range from IOPs was related to bIOP. The lowest mean difference and the highest agreement with bIOP were observed for the IOPcc.
IOP measured with the most commonly used tonometer in clinics, GAT, is influenced by various corneal morphological factors and especially corneal biomechanical properties.Citation3 Various studies were designed to compensate as much as possible for these factors and to estimate an IOP near the actual intraocular pressure, their efforts led to introduction of various devices such as the Dynamic Contour Tonometer (DCT), the Ocular Response Analyzer (ORA) and more lately the CorVis ST which provides biomechanically corrected IOP using the finite element modeling.Citation31,Citation32
Eliasy et al (2018) determined the true IOP in ex vivo condition in the cadaver eyes using a pressure transducer and reported no significant difference between the true IOP and bIOP with a mean difference 0.3 mmHg while the non-corrected IOP measured using Corvis (IOPnct) had a significant difference with a mean difference 7.5 mmHg.Citation21
The present study did not show a significant difference in the determined bIOP in the corneas with different thicknesses, like this lack of correlation were reported previously in ex vivo pressure assessment in human enucleated eyesCitation21 and also in comparison of the bIOP before and after different corneal refractive surgery techniques, laser in situ keratomileusis (LASIK) and refractive lenticule extraction small-incision lenticule extraction (SMILE), transepithelial photorefractive keratectomy (PRK) and transepithelial PRK combined with accelerated corneal cross-linking.Citation17,Citation19 These studies showed that the bIOP in contrast to the other IOPs derived using different tonometry methods such as GAT was not significantly affected by tissue subtracting refractive surgery techniques.
Therefore this may be considered as a significant milestone in the short and long-term follow-up of these patients that may be at risk for glaucoma over the next few years with attention to the fact that each 100 µm change in the corneal thickness was associated with a measurement error 0.7–7.1 mmHg and each 1 mmHg increase in the IOP raised the glaucoma risk by about 10%.Citation33–Citation35
Acceptable repeatability and reproducibility in bIOP assessment were reported in 32 normal cases with an age range from 18.6 to 64.2 years old.Citation36 Comparing bIOP with GAT showed that the bIOP was approximately 3 mmHg higher than GAT which is in contrast to the previous studies reported lower IOP using CorVis than GAT with a mean difference 1.3 mmHg.Citation6 This difference can be attributed to the age range difference, 23–75 years old versus 20–46 years old in the present study.
One limitation of this study was no including the dynamic contour tonometer (DCT) for comparative purposes since there is a view that the measured IOP using this tonometer is less affected by corneal stiffness properties compared to other tonometers. Also, this study was only conducted in healthy eyes and repeating these comparisons in patients with normal and low tension glaucoma and subjects with ocular hypertension is suggested for future researches.
Conclusion
The accurate IOP measurement is an essential part of the evaluation of glaucoma. In-vivo assessment of the corneal biomechanical properties and the ability to adjust IOP based on these parameters shows that using the conventional tonometers may lead to inaccurate tonometer readings and ultimately incorrect identification of those at risk. Given that most of the current definitions and protocols available in clinical protocols are based on GAT, the results of this study showed that the obtained results using this tonometer should be taken with caution, especially in the suspicious eyes.
Abbreviations
IOP, Intraocular pressure; GAT, Goldmann applanation tonometer; ORA, Ocular response analyzer; RBT, Rebound tonometer; CCT, Central corneal thickness; bIOP, biomechanically corrected IOP; SE, Spherical equivalent; IOPcc, Cornea-compensated IOP.
Ethics Approval And Consent To Participate
This research was approved by the ethical committee of Deputy of Research of Mashhad University of Medical Sciences (grant code: 960298). Subjects’ informed consent was obtained following the principles of the Declaration of Helsinki.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the personnel of Sedaghat Eye Clinic and the participants who made this study possible, and the Deputy of Research of Mashhad University of Medical Sciences (grant code: 960298).
Disclosure
Renato Ambrósio Jr reports personal fees from Oculus, during the conduct of the study, and personal fees from Alcon and Mediphacos and non-financial support from Essilor and Zeiss, outside the submitted work. Ahmed Elsheikh is a consultant for Oculus and has received financial support for his research from the company. The authors report no other conflicts of interest in this work.
References
- Bao F, Deng M, Wang Q, et al. Evaluation of the relationship of corneal biomechanical metrics with physical intraocular pressure and central corneal thickness in ex vivo rabbit eye globes. Exp Eye Res. 2015;137:11–17. doi:10.1016/j.exer.2015.05.01826026878
- Doughty MJ, Zaman ML. Human corneal thickness and its impact on intraocular pressure measures: a review and meta-analysis approach. Surv Ophthalmol. 2000;44(5):367–408.10734239
- Bao F, Huang Z, Huang J, et al. Clinical evaluation of methods to correct intraocular pressure measurements by the Goldmann applanation tonometer, ocular response analyzer, and Corvis ST tonometer for the effects of corneal stiffness parameters. J Glaucoma. 2016;25(6):510–519. doi:10.1097/IJG.000000000000035926709500
- Martinez-de-la-Casa JM, Garcia-Feijoo J, Fernandez-Vidal A, Mendez-Hernandez C, Garcia-Sanchez J. Ocular response analyzer versus Goldmann applanation tonometry for intraocular pressure measurements. Invest Ophthalmol Vis Sci. 2006;47(10):4410–4414. doi:10.1167/iovs.06-015817003433
- Bayoumi NH, Bessa AS, El Massry AA. Ocular response analyzer and goldmann applanation tonometry: a comparative study of findings. J Glaucoma. 2010;19(9):627–631. doi:10.1097/IJG.0b013e3181ca7e0120179628
- Hong J, Xu J, Wei A, et al. A new tonometer–the Corvis ST tonometer: clinical comparison with noncontact and Goldmann applanation tonometers. Invest Ophthalmol Vis Sci. 2013;54(1):659–665. doi:10.1167/iovs.12-1098423307970
- Stamper RL. A history of intraocular pressure and its measurement. Optom Vis Sci. 2011;88(1):E16–E28. doi:10.1097/OPX.0b013e318205a4e721150677
- Salvetat ML, Zeppieri M, Tosoni C, Brusini P. Repeatability and accuracy of applanation resonance tonometry in healthy subjects and patients with glaucoma. Acta Ophthalmol. 2014;92(1):e66–e73. doi:10.1111/aos.1220923837834
- Elsheikh A, Alhasso D, Gunvant P, Garway-Heath D. Multiparameter correction equation for Goldmann applanation tonometry. Optom Vis Sci. 2011;88(1):E102–e112. doi:10.1097/OPX.0b013e3181fc345321037494
- Aziz K, Friedman DS. Tonometers—which one should I use? Eye. 2018;32(5)931–937.
- Huseynova T, Waring GO, Roberts C, Krueger RR, Tomita M. Corneal biomechanics as a function of intraocular pressure and pachymetry by dynamic infrared signal and Scheimpflug imaging analysis in normal eyes. Am J Ophthalmol. 2014;157(4):885–893. doi:10.1016/j.ajo.2013.12.02424388837
- Reznicek L, Muth D, Kampik A, Neubauer AS, Hirneiss C. Evaluation of a novel Scheimpflug-based non-contact tonometer in healthy subjects and patients with ocular hypertension and glaucoma. Br J Ophthalmol. 2013;97(11):1410–1414. doi:10.1136/bjophthalmol-2013-30340023969314
- Chui WS, Lam A, Chen D, Chiu R. The influence of corneal properties on rebound tonometry. Ophthalmology. 2008;115(1):80–84. doi:10.1016/j.ophtha.2007.03.06117573114
- Martinez-de-la-Casa JM, Garcia-Feijoo J, Castillo A, Garcia-Sanchez J. Reproducibility and clinical evaluation of rebound tonometry. Invest Ophthalmol Vis Sci. 2005;46(12):4578–4580. doi:10.1167/iovs.05-058616303951
- Suman S, Agrawal A, Pal VK, Pratap VB. Rebound tonometer: ideal tonometer for measurement of accurate intraocular pressure. J Glaucoma. 2014;23(9):633–637. doi:10.1097/IJG.0b013e318285fefd23429611
- Pinero DP, Alcon N. In vivo characterization of corneal biomechanics. J Cataract Refract Surg. 2014;40(6):870–887. doi:10.1016/j.jcrs.2014.03.02124857436
- Chen KJ, Joda A, Vinciguerra R, et al. Clinical evaluation of a new correction algorithm for dynamic Scheimpflug analyzer tonometry before and after laser in situ keratomileusis and small-incision lenticule extraction. J Cataract Refract Surg. 2018;44(5):581–588. doi:10.1016/j.jcrs.2018.01.02329685776
- Hugo J, Granget E, Ho Wang Yin G, Sampo M, Hoffart L. Intraocular pressure measurements and corneal biomechanical properties using a dynamic Scheimpflug analyzer, after several keratoplasty techniques, versus normal eyes. J Fr Ophtalmol. 2018;41(1):30–38. doi:10.1016/j.jfo.2017.06.00629191679
- Lee H, Roberts CJ, Ambrosio R Jr., Elsheikh A, Kang DSY, Kim TI. Effect of accelerated corneal crosslinking combined with transepithelial photorefractive keratectomy on dynamic corneal response parameters and biomechanically corrected intraocular pressure measured with a dynamic Scheimpflug analyzer in healthy myopic patients. J Cataract Refract Surg. 2017;43(7):937–945. doi:10.1016/j.jcrs.2017.04.03628823441
- Lee H, Roberts CJ, Kim TI, Ambrosio R Jr., Elsheikh A, Yong Kang DS. Changes in biomechanically corrected intraocular pressure and dynamic corneal response parameters before and after transepithelial photorefractive keratectomy and femtosecond laser-assisted laser in situ keratomileusis. J Cataract Refract Surg. 2017;43(12):1495–1503. doi:10.1016/j.jcrs.2017.08.01929335093
- Eliasy A, Chen KJ, Vinciguerra R, et al. Ex-vivo experimental validation of biomechanically-corrected intraocular pressure measurements on human eyes using the CorVis ST. Exp Eye Res. 2018;175:98–102. doi:10.1016/j.exer.2018.06.01329908883
- Johnson TV, Toris CB, Fan S, Camras CB. Effects of central corneal thickness on the efficacy of topical ocular hypotensive medications. J Glaucoma. 2008;17(2):89–99. doi:10.1097/IJG.0b013e31814b993818344753
- Morales-Fernandez L, Martinez-de-la-Casa JM, Garcia-Feijoo J, Saenz-Frances F, Santos-Bueso E, Garcia-Sanchez J. Reproducibility of the new Goldmann AT900D digital tonometer. J Glaucoma. 2012;21(3):186–188. doi:10.1097/IJG.0b013e31820bd1e921423040
- Sullivan-Mee M, Gerhardt G, Halverson KD, Qualls C. Repeatability and reproducibility for intraocular pressure measurement by dynamic contour, ocular response analyzer, and goldmann applanation tonometry. J Glaucoma. 2009;18(9):666–673. doi:10.1097/IJG.0b013e31819c487d20010245
- Yaoeda K, Fukushima A, Shirakashi M, Fukuchi T. Comparison of intraocular pressure adjusted by central corneal thickness or corneal biomechanical properties as measured in glaucomatous eyes using noncontact tonometers and the Goldmann applanation tonometer. Clin Ophthalmol. 2016;10:829–834. doi:10.2147/OPTH.S10683627274187
- Grippo TM, Liu JH, Zebardast N, Arnold TB, Moore GH, Weinreb RN. Twenty-four-hour pattern of intraocular pressure in untreated patients with ocular hypertension. Invest Ophthalmol Vis Sci. 2013;54(1):512–517. doi:10.1167/iovs.12-1070923211815
- Bang SP, Lee CE, Kim YC. Comparison of intraocular pressure as measured by three different non-contact tonometers and goldmann applanation tonometer for non-glaucomatous subjects. BMC Ophthalmol. 2017;17(1):199. doi:10.1186/s12886-017-0593-129096616
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–310.2868172
- Portney LGWM. Foundations of Clinical Research. Applications to Practice. 2ed ed. Upper Saddle River, NJ: Prentice Hall Health; 2000.
- Roberts CJ, Mahmoud AM, Bons JP, et al. Introduction of two novel stiffness parameters and interpretation of air puff-induced biomechanical deformation parameters with a dynamic scheimpflug analyzer. J Refract Surg. 2017;33(4):266–273. doi:10.3928/1081597X-20161221-0328407167
- Joda AA, Shervin MM, Kook D, Elsheikh A. Development and validation of a correction equation for Corvis tonometry. Comput Methods Biomech Biomed Engin. 2016;19(9):943–953.27049961
- Vinciguerra R, Elsheikh A, Roberts CJ, et al. Influence of pachymetry and intraocular pressure on dynamic corneal response parameters in healthy patients. J Refract Surg. 2016;32(8):550–561. doi:10.3928/1081597X-20160524-0127505316
- Gunvant P, Baskaran M, Vijaya L, et al. Effect of corneal parameters on measurements using the pulsatile ocular blood flow tonograph and Goldmann applanation tonometer. Br J Ophthalmol. 2004;88(4):518–522. doi:10.1136/bjo.2003.01933115031169
- Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003;121(1):48–56. doi:10.1001/archopht.121.1.4812523884
- Tonnu PA, Ho T, Newson T, et al. The influence of central corneal thickness and age on intraocular pressure measured by pneumotonometry, non-contact tonometry, the Tono-Pen XL, and Goldmann applanation tonometry. Br J Ophthalmol. 2005;89(7):851–854. doi:10.1136/bjo.2004.05662215965165
- Lopes BT, Roberts CJ, Elsheikh A, et al. Repeatability and reproducibility of intraocular pressure and dynamic corneal response parameters assessed by the Corvis ST. J Ophthalmol. 2017;2017:8515742.28676837