
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
To diagnose keratoconus at its earliest stage is meaningful in order to avoid refractive surgery in the eye, which may lead to further damage in the abnormal cornea structure and consequently cause iatrogenic ectasia. In this article, the following aspects of detecting earliest stage of keratoconus were reviewed: 1) nomenclature of the earliest forms of keratoconus; 2) diagnosis of keratoconus using curvature-based topography (also known as Placido-based topography, ie, videokeratography) as a traditional method and elevation-based topography as a new method which has gained popularity in recent years; and 3) other methods analyzing keratoconus cornea like corneal biomechanics and wavefront sensing. Elevation-based topography using either Scheimpflug imaging techniques or slit-scanning imaging techniques has shown to be advantageous over the curvature-based topography in detecting keratoconus at its earliest stage. Posterior elevation of the cornea is notified to enhance the sensitivity and specificity of detection if used along with the measurements of anterior surface of the cornea. Cornea biomechanics analysis and wavefront sensing also revealed differences between normal eyes and keratoconic eyes in their earliest stage. Combining the latest technology and the traditional techniques will be the future trend to improve early diagnosis of keratoconus.
Introduction
One of the most important aspects of avoiding iatrogenic ectasia in cornea during refractive surgery was to detect keratoconus in its earliest stage. However, there were several challenges in earliest detection of this disease. First, in the literature there were several names referring to the earliest stage of keratoconus, which were frequently misused and cause confusion. Second, speaking of keratoconus, eye doctors get used too much to describing the cornea simply with a single K value or as a skewed axis bowtie in videokeratoscopy. This single K value, in fact, was far from sensitive in detecting earliest keratoconus than using a comprehensive system, which also accounts for other cornea property parameters. Videokeratoscopy itself has had numerous limitations, especially compared with the newly developed elevation-based topography. Third, even if there were many other technologies that show different aspects in earliest keratoconus, like biomechanics features and wavefront aberrations, the lack of awareness among eye doctors to combine multiple cornea features comprehensively limited their role in early detection of this disease. In this article, the above listed three challenges will be reviewed and discussed. Hopefully by doing so, it will lead to the recognition of the latest trend in early detection of keratoconus.
Nomenclature of earliest keratoconus
Forme fruste keratoconus
Referring to the earliest stage keratoconus, three names were widely encountered in the literature: forme fruste keratoconus (FFKC), keratoconus suspect, and preclinical or subclinical keratoconus. FFKC was firstly proposed by AmslerCitation1 in 1961 and then adapted by KlyceCitation2 as “The fellow eye (of a clinical manifest keratoconus eye) that has no clinical findings of any sort except for certain topographical changes (vide infra)”.
In the literature, there is a clear consensus for FFKC that it should be the healthier eye in a keratoconus patient, and this healthier eye should not have any clinical signs of clinical manifest keratoconus, like Vogt’s striae and Fleischer’s ring, nor should this eye have any significant topographic changes like skewed axis bowtie which indicates it is a clinical manifest keratoconus.Citation3,Citation4
Keratoconus suspect
There were several opinions on when to use the term “keratoconus suspect”. In Klyce’s option, keratoconus suspect should be a term reserved for corneas with very specific topographic changes and for patients who do not have keratoconus in the fellow eye: “In general terms, a topographic keratoconus suspect will have a localized area of abnormal steepening which is often inferior, but can be central, or, rarely, superior, and may present as an asymmetrical, truncated or skewed-axis bowtie”. He then summarized “the term keratoconus suspect should properly be reserved for corneas with subtle signs of keratoconus but without evidence of clinical keratoconus in either eye”.Citation2 In fact, his definition here also fits subclinical keratoconic eyes, as we would describe in the next few sections.
But another opinion overlapped keratoconus suspect with FFKC as we defined above. WaringCitation5 identified keratoconus suspect as “the fellow eyes of unilateral keratoconus that had no slit-lamp findings”. He further noted the term keratoconus suspect should extend to “patients with manifest clinical keratoconus in one eye and only videokeratographic inferior steepening in the other, and in family members of patients with clinically manifest keratoconus, who show only videokeratographic steepening inferiorly”, because such a way is “in the same sense that a patient who has glaucoma suspect.”
A third opinion of Rabinowitz et al defined keratoconus suspect in a progressive prospective and their definition was independent of the status of the fellow eye as “no slit lamp findings, no scissoring on retinoscopy, and AB/SRAX (Asymmetric Bowtie pattern with a Skewed Radial Axis) on videokeratography only”.Citation6 They developed a detection system to differentiate normal cornea and keratoconus suspect. They recommend using the inferior–superior (I-S) value, which computed the vertical gradient cornea power of 6 mm region. An I-S value between 1.4 and 1.9 diopters suggests a keratoconus suspect, while a larger value suggests clinical keratoconus. A lower value suggests a normal variant cornea. But they also admitted that the differences in videokeratography indexes between keratoconus suspect and normal eyes are subtle. Their criteria for keratoconus suspect actually also fit to subclinical keratoconus, as we would describe in the next few sections.
Some authors provided their own definitions of keratoconus suspect. Rao et alCitation7 defined their keratoconus suspect, after excluding the contact lens warping, as “to achieve the computer designation keratoconus pattern suspected, either the central K or the I-S value calculated for a given videokeratography must be two standard deviations greater than the mean”.
At this point though, one needs to be cautious about the localized steepening of the cornea, which could be caused by various other factors than earliest keratoconus. Common factors that can cause inferior steepening of videokeratography but no clinical manifest of keratoconus include but not limited to “hard contact lenses wearing, nosecone compression, technician’s finger compression, and a dry cornea inferiorly”.Citation5 The rigid contact lens caused cornea warpage can persist for quite a long time. So the term keratoconus suspect should be applied to these patients until contact lenses have been removed for an adequate period of time.Citation8,Citation9
Due to tremendous discrepancies among authors, we highly suggest using this terminology only with a clear description of objective, topographic index-based criteria. Also, figuring out what exactly the criteria are helps tremendously in understanding various authors throughout the literature.
Subclinical keratoconus
Some of the authors in the literature agreed on the subclinical keratoconus as a fellow eye of a clinical manifest keratoconus eye with the following features: 1) no clinical findings (keratometric, retinoscopic, or biomicroscopic) of keratoconus; 2) I-S asymmetry and/or bowtie pattern with SRAX, detected on tangential Placido disk-based videokeratography (CSO EyeTop or Keratron); and 3) no history of contact lens wear, ocular surgery, or trauma.Citation10–Citation12
Some others have had their own definitions. Jafarinasab et alCitation13 used major and minor criteria to select subclinical keratoconus, independent of the condition of the fellow eye. Major criteria include: 1) the presence of Vogt’s striae and Fleischer ring measuring at least 2 mm; 2) SRAX index >20°; 3) KPI >30%; 4) KSI >30%; and 5) an abnormal KCI. Minor criteria include: 1) asymmetric bow–tie pattern without SRAX; 2) inferior steepening; 3) KSI between 15% and 30%; and 4) KPI between 23% and 30%. Subclinical keratoconus was diagnosed in the presence of one major or two minor criteria.
SRAX is an index that reflects the irregular astigmatism in keratoconus. KPI is a linear discriminate analysis of eight quantitative topographic indices. KCI is derived by using a binary decision-making tree that was input from the KPI and four other indices. KSI is a index derived from neural network algorithm.
Ruiseñor Vázquez et alCitation17 used a keratoconus severity score system, which involved evaluating slit-lamp findings, topography pattern, cornea power, and higher order aberrations. While one eye scored high enough to be considered as clinical keratoconus, the fellow eye scored lower would be considered a subclinical keratoconus.
Sometimes, people used this term to refer to a much larger variety of earliest stage keratoconus, like including FFKC and keratoconus suspect.Citation18 But it was soon criticized and their definition was requested to be refined with a combination of clear objective topographic indices.Citation19
Therefore, similar to the term keratoconus suspect, make sure of the exact definition of the author when the term “subclinical keratoconus” is mentioned. Also, for authors to mention this term, they need to provide their clear definitions and employ objective topographic indices to do so.
The fellow eye and family history
In 1991, Maguire and Lowry observed a fellow eye in a unilateral keratoconus patient for 2 years. At the very beginning of the observation, this patient had one eye identified as clinical manifest keratoconus and the other eye had a normal topography, but showed a localized cornea steepening of “44.5 diopters located 2.1 mm inferior to the vertex normal”.Citation20 Two year later, “cone apex power increased to 51 diopters, and the patient developed a Fleischer’s ring, Vogt’s striae, and mild visual aberration”;Citation20 in other words, a clinical manifest keratoconus.
After the first observation of a single fellow eye within 2 years by Maguire and Lowry, Li et alCitation21 observed over a 100 patients diagnosed as unilateral keratoconus at the baseline. They concluded that within 16 years, approximately 50% of the clinical normal fellow eyes would develop into clinical manifest keratoconus. The greatest risk of onset is during the first 6 years of diagnosis.
Li et alCitation22 also followed over 300 people who had a family history of keratoconus but did not have keratoconus themselves (unaffected keratoconus relatives) for 1 to 8 years, and compared them with over 100 normal controls. They concluded that between the two groups, there was no statistically significant difference in progression to keratoconus. The family history did not play a significant role in keratoconus progression.
Therefore, the fellow eye of a unilateral keratoconus patient should be refrained from refractive surgery, especially within the first 6 years after first diagnosis. People with a keratoconus family history but who did not have keratoconus themselves are more likely to be treated as people from a normal population.
Summary of nomenclature of earliest keratoconus
FFKC as clearly agreed in the literature should refer to the fellow eye of a clinical manifest keratoconus. The eye itself should have neither clinical signs of keratoconus nor significant topographic signs that lead to diagnosis of keratoconus.
Subclinical keratoconus and keratoconus suspect can be used interchangeably for an eye showing some feature of keratoconus topography, but not severe enough to be named as clinical manifest keratoconus. Its fellow eye can be either a clinical manifest keratoconus or a normal eye. But one needs to provide his/her definition with objective, topographic-based criteria if these names are to be used. For the purpose of clarity, we will use only “subclinical keratoconus” for the later part of this article to indicate the situation suitable for both names, except when citing another author’s work.
Detect earliest keratoconus with curvature-based topography, like videokeratography
In the past, early detection of keratoconus was based on keratoscope, a Placido-based curvature distortion measurement of the anterior surface of the cornea.Citation23
In the recent 30 years, the emergence of computer-assisted keratoscope, well known as videokeratography, enabled quantitative and more precise measurement on anterior cornea surface of keratoconic eyes. Rabinowitz and McDonnell found that a central K value larger than 47.2 diopters and an I-S value larger than 1.4 diopters to indicate that it is a subclinical keratoconus instead of a normal eye. A central K larger than 47.8 diopters and an I-S value larger than 1.9 diopters indicate it is a clinical manifest keratoconus.Citation24
Rabinowitz and RasheedCitation14 later developed an even better index known as KISA% to enhance the specificity of diagnoses keratoconus in its earliest stage. KISA% involves two more parameters: Astigmatism (AST), the degree of regular corneal astigmatism, and SRAX index, an expression of the irregular astigmatism occurring in keratoconus. Rabinowitz indicates that the eyes with KISA% larger than 100% will be identified as clinical manifest keratoconus, and 60% to 100% to be keratoconus suspect with minimal overlapping with normal corneas. KISA% is computed as follows.
where:
K is central K value;
I-S is inferior to superior value, which is the difference of cornea power between average of 5 inferior points and 5 superior points 3 mm from the center at 30 degree intervals;
AST is the regular astigmatism;
SRAX is the skewed radial axis index, an expression of irregular astigmatism occurring in keratoconus. (see Rabinowitz and RasheedCitation14 for more detailed calculations of above mentioned indices).
In the meantime, Maeda–Klyce developed a KPI system which uses eight indices generated from videokeratography to detect keratoconus. A KPI score larger than 0.23 is indicative of keratoconus. However, it is not readily useful for keratoconus suspect due to a significant overlapping between keratoconus suspect and keratoconus in its scoring system.
Maeda et alCitation25 developed a neural network model to detect and classify cornea topography abnormalities. Beside keratoconus, this model was capable of examining a variety of cornea abnormalities including postphotorefractive keratectomy and postkeratoplasty. Later, Smolek and KlyceCitation16 further modified this model, which approached 100% of accuracy, sensitivity, and specificity in the diagnosis of keratoconus.
The Rabinowitz system, the Maeda–Klyce system, and the later developed neural network system were the three most widely used diagnostic systems based on videokeratography to define normal cornea, subclinical keratoconus (or keratoconus suspect), and clinical manifest keratoconus. These definitions were then widely used to classify normal and ectasic cornea in more recent research that evaluated the sensitivity and specificity of parameters measured by elevation-based topography and other modalities.
Elevation-based topography
In recent years, the elevation-based topography gained more and more attention in keratoconus early detection. Two principles were employed in the most popular elevation-based topography devices, slit-scanning and Scheimpflug imaging techniques. Slit-scanning technique is used in the Orbscan II (Bausch and Lomb Surgical, Inc., Rochester, NY, USA) and it is the only commercial available slit-scanning implementation. Whereas, Scheimpflug is widely used in a variety of instruments: the Pentacam (Oculus, Arlington, WA, USA), the Galilei (Ziemer Ophthalmic Systems AG, Port, Switzerland), the Precisio (Ligi Tecnologie Medicali, Taranto, Italy), and the Sirius (CSO Ophthalmic, Instrument Company, Auckland, New Zealand).
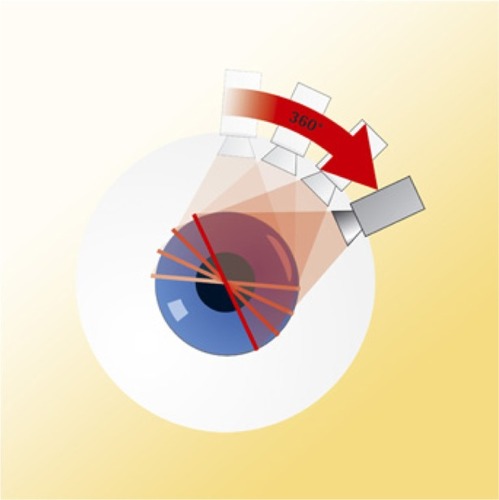
The slit-scanning technique was performed by two vertical scans of 40 light-slits projections, 20 from the left and 20 from the right, onto the camera to the instrument axis (). The Scheimpflug camera obtained images by rotating around the optic axis with projected light-slits (). The anterior and posterior edges of the slits would be captured by the camera and analyzed to reconstruct the anterior segment surfaces.
Figure 1 Slit-scanning technique performed by Orbscan.
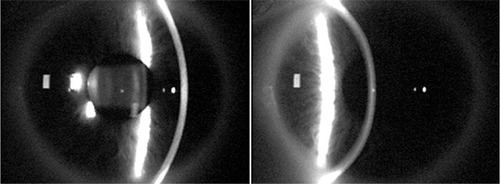
Figure 2 Scheimpflug technique performed by Pentacam.
Elevation-based topography obtains obvious advantages than the traditional curvature-based topography. First, elevation-based topography covers much more cornea area than videokeratography (9 versus 6 mm) in diameter. Larger measurement area allows detection of changes in more peripheral cornea, which is affected in later stage of keratoconus and in pellucid marginal degeneration.
Second, elevation-based topography does not make the assumption that the eye is a Gullstrand’s reduced eye, which has to be made in videokeratography and other Placido-based topography. In this assumption, the line of sight is assumed to be the same as the line that goes through the anatomic center of the eye. In fact, in most of the eyes, the angle between these two lines (known as angle Kappa) is less than 5 degrees. Most of the time, such an assumption would not result in too much bias. However, if a normal eye happened to have an angle kappa greater than 5 degrees, it will be easily misdiagnosed as having an asymmetric bowtie in curvature-based topography. Elevation-based topography does not make such a mistake because it avoids the Gullstrand’s reduced eye assumption.
Another advantage of using elevation-based topography is that it is capable of measuring the posterior surface of the cornea in addition to the anterior surface. This is the most exciting feature offered by elevation-based topography because in recent years more and more studies have shown that compared to normal eyes, there is a significant posterior surface difference in earliest keratoconus eyes.
There were significant posterior elevation differences between normal eye and the eye fulfilled either of the Rabinowitz or Klyce–Maeda keratoconus criteria.Citation7 Posterior elevation of the cornea had a higher sensitivity and specificity to discriminate keratoconic eyes from normal eyes in earlier staged keratoconus than later staged keratoconus, based on the Amsler–Krumeich classification staging of keratoconus.Citation27,Citation28 In subclinical keratoconus, there was a significant difference in posterior elevation than normal eyes (, column 3).Citation12 Adding posterior corneal elevation data to an artificial intelligence algorithm would improve the sensitivity and specificity to separate normal eyes and subclinical keratoconic eyes (, row “Arbelaez 2012”, columns 9–11).Citation18 However, none of them recommended using posterior elevation as a single factor to diagnose subclinical keratoconus due to the sensitivity and specificity always being incapable of steadily reaching more than 90% and the disparity of cut-off points among different measuring methods (, columns 7 and 8). The posterior elevation should be combined with other parameters such as cornea curvature, cornea power, anterior elevation, and thickness to achieve a better effect.
Table 1 Studies use posterior elevation and derived parameters to discriminate subclinical keratoconus and normal eyes
In FFKC, elevation-based topography was able to tell apart FFKC from normal eyes, whereas Placido-based topography, even using a neural network recognition system, could not do so.Citation3 Fukuda et alCitation29 proved that either a three-dimensional anterior segment optical coherence tomography or an elevation-based topography adopting Scheimpflug principle combined with a curvature-based topography would recognize the differences between FFKC and normal eyes (, row “Fukuda 2013”). Muftuoglu et alCitation4 further noted in Pentacam that a parameter called “back difference elevation” was superior than posterior elevation to recognized FFKC. However, using either of the above two parameters alone would not be recommended to diagnose FFKC due to insufficient sensitivity and specificity (, columns 7 and 8).
Table 2 Studies use posterior elevation and derived parameters to discriminate forme fruste keratoconus (FFKC) and normal eyes (N)
There was also a study that compared the keratoconus cross-linking treatment guided either by curvature-based topography or an elevation-based topography adopting the Scheimpflug principle. Crosslinking guided by Scheimpflug resulted in better cornea surface regularity, more flat and more central cones, compared to the ones guided by curvature-based topography.Citation30
Nederan et alCitation31 compared the most popular two types of elevation-based topography, Pentacam and Orbscan IIz. They found the two devices have no differences in measuring cornea central thickness (CCT) and thinnest central thickness, but there was a significant difference in anterior chamber depth and pupil diameter. The measurements of different devices were not interchangeable. The disparity between the two methods was not elucidated. However, it was observed that by removal of the acoustic factor and CCT would be overestimated by Orbscan IIz.Citation32 Orbscan IIz’s usage of ultrasound to assist its pachymetry measurement may underline its possibility to overestimate corneal thickness.
Beside the cornea curvature and elevation, earliest keratoconus showed significant differences than the normal eyes in a variety of other cornea characteristics. The two most widely studied characteristics include corneal biomechanics and wavefront aberrations.
Corneal biomechanics
It is well known keratoconus eyes have a significant lower CCT, corneal hysteresis, and corneal resistant factor (CRF) than normal eyes.Citation33,Citation34 shows corneal hysteresis, CRF, and CCT values for normal eyes, FFKC, mild keratoconic, and keratoconic eyes from different studies. In mild keratoconus, it is controversial to say there is a significant difference between mild keratoconus and normal eyes in cornea hysteresis.Citation33,Citation35 Area under receiver operating characteristic curve shows only 87% of sensitivity and 65% of specificity for corneal hysteresis, and 90.5% of sensitivity and 66% of specificity for CRF to discriminate mild keratoconus and normal eyes.Citation35 However, some studies group FFKC and normal eyes with central cornea thickness.Citation36 In the low corneal central thickness groups (<500 and <540 μm), corneal hysteresis achieves 91% of sensitivity for both cornea thickness groups to distinguish FFKC and normal eyes.Citation36 But for CRF it is only 81% and 87% sensitivity. Specificity was not studied.
Table 3 Corneal central thickness (CCT), corneal hysteresis (CH), and corneal resistant factor (CRF) in normal (N), forme fruste keratoconus (FFKC), mild keratoconus (mild KC), and keratoconus (KC) eyes
Wavefront aberrations
In the earliest studies, wavefront aberrations were derived from videokeratography surface height measurement. Using this method, Schwiegerling and GreivenkampCitation37 found that an index made up of two lower order aberrations (eg, defocus and astigmatism) detects keratoconus as effective as curvature characteristics like I-S value, steepest radial axes, and surface asymmetry index. Later, Gobbe and GuillonCitation38 found that keratoconus suspect distinguishes itself from normal eyes by a larger amount of vertical coma.
Later on, Shack–Hartmann wavefront sensor was widely used to measure the wavefront characteristics in keratoconus, subclinical keratoconus, and FFKC. Vertical coma is the most important higher order aberration in keratoconus eyes.Citation39 Vertical coma was also the most widely mentioned aberration that had a significant difference between subclinical keratoconus and normal eyes.Citation40–Citation42 However, using vertical coma alone cannot achieve high enough sensitivity and specificity to discriminate subclinical keratoconus and normal eyes.Citation43
In FFKC, vertical coma also was the most widely mentioned aberration that was significantly larger than normal eyes.Citation44–Citation46 Although front surface vertical coma played a much more important role than other aberrations and parameters,Citation44 using this single aberration term only was not good enough to discriminate FFKC and normal eyes.Citation44,Citation45 If other parameters like I-S value, other higher order aberrations, and pachymetry were involved, the discrimination function would achieve better performance.Citation44,Citation45 Sensitivity and specificity achieved one if front surface aberrations, back surface aberrations, and pachymetry are used altogether in the discrimination of FFKC and normal eyes.Citation44
Summary and conclusion of early detection of keratoconus
Subtle changes in earliest keratoconus eyes like posterior corneal elevation, corneal hysteresis, cornea resistant factor, and vertical coma could be detected by elevation-based topography, biomechanics, and wavefront sensor. However, none of these subtle changes had enough sensitivity or specificity to be used alone to make a diagnosis. To develop a multiple factor system that combines curvature measurements, elevation measurements, pachymetry, biomechanics, and wavefront error of the cornea will be the future trend to diagnose the earliest form of keratoconus including forme fruste keratoconus and subclinical keratoconus.
Disclosure
The author reports no conflicts of interest in this work.
References
- AmslerMThe ‘forme fruste’ of keratoconusWien Klin Wochenschr19617384284313861052
- KlyceSDChasing the suspect: keratoconusBr J Ophthalmol20099384584719553507
- SaadAGatinelDTopographic and tomographic properties of forme fruste keratoconus corneasInvest Ophthalmol Vis Sci2010515546555520554609
- MuftuogluOAyarOOzulkenKOzyolEAkıncıAPosterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patientsJ Cataract Refract Surg2013391348135723820305
- WaringGONomenclature for keratoconus suspectsRefract Corneal Surg199392192228343441
- LiXYangHRabinowitzYSKeratoconus: Classification scheme based on videokeratography and clinical signsJ Cataract Refract Surg20093591597160319683159
- RaoSNRavivTMajmudarPAEpsteinRJRole of Orbscan II in screening keratoconus suspects before refractive corneal surgeryOphthalmology20021091642164612208710
- Ruiz-MontenegroJMafraCHWilsonSEJumperJMKlyceSDMendelsonENCorneal topographic alterations in normal contact lens wearersOphthalmology19931001281348433817
- WilsonSELinDTCKlyceSDReidyJJInslerMSTopographic changes in contact lens-induced corneal warpageOphthalmology1990977347442374677
- De SanctisULoiaconoCRichiardiLTurcoDMutaniBGrignoloFMSensitivity and specificity of posterior corneal elevation measured by Pentacam in discriminating keratoconus/subclinical keratoconusOphthalmology20081151534153918405974
- De SanctisUAragnoVDalmassoPBrusascoLGrignoloFDiagnosis of subclinical keratoconus using posterior elevation measured with 2 different methodsCornea20133291191523572130
- UçakhanÖÖÇetinkorVÖzkanMKanpolatAEvaluation of Scheimpflug imaging parameters in subclinical keratoconus, keratoconus, and normal eyesJ Cataract Refract Surg2011371116112421596255
- JafarinasabMRShirzadehEFeiziSKarimianFAkaberiAHasanpourHSensitivity and specificity of posterior and anterior corneal elevation measured by Orbscan in diagnosis of clinical and subclinical keratoconusJ Ophthalmic Vis Res201510101526005546
- RabinowitzYSRasheedKKISA% index: a quantitative videokeratography algorithm embodying minimal topographic criteria for diagnosing keratoconusJ Cataract Refract Surg1999251327133510511930
- MaedaNKlyceSDSmolekMKThompsonHWAutomated keratoconus screening with corneal topography analysisInvest Ophthalmol Vis Sci199435274927578188468
- SmolekMKKlyceSDCurrent keratoconus detection methods compared with a neural network approachInvest Ophthalmol Vis Sci199738229022999344352
- Ruiseñor VázquezPRGallettiJDMinguezNPentacam Scheimpflug tomography findings in topographically normal patients and subclinical keratoconus casesAm J Ophthalmol2014158324024709808
- ArbelaezMCVersaciFVestriGBarboniPSaviniGUse of a support vector machine for keratoconus and subclinical keratoconus detection by topographic and tomographic dataOphthalmology20121192231223822892148
- SaadAGatinelDSubclinical keratoconus: the need for an objective classification systemOphthalmology2013120e56e5723916087
- MaguireLJLowryJCIdentifying progression of subclinical keratoconus by serial topography analysisAm J Ophthalmol1991112141451882920
- LiXRabinowitzYSRasheedKYangHLongitudinal study of the normal eyes in unilateral keratoconus patientsOphthalmology200411144044615019316
- LiXYangHRabinowitzYSLongitudinal study of keratoconus progressionExp Eye Res20078550250717681291
- KrachmerJHFederRSBelinMWKeratoconus and related noninflammatory corneal thinning disordersSurv Ophthalmol1984282933226230745
- RabinowitzYSMcDonnellPJComputer-assisted corneal topography in keratoconusRefract Corneal Surg198954004082488838
- MaedaNKlyceSDSmolekMKNeural network classification of corneal topography. Preliminary demonstrationInvest Ophthalmol Vis Sci199536132713357775110
- OliveiraCMRibeiroCFrancoSCorneal imaging with slit-scanning and Scheimpflug imaging techniquesClin Exp Optom201194334220718786
- IshiiRKamiyaKIgarashiAShimizuKUtsumiYKumanomidoTCorrelation of corneal elevation with severity of keratoconus by means of anterior and posterior topographic analysisCornea20123125325822316650
- KamiyaKIshiiRShimizuKIgarashiAEvaluation of corneal elevation, pachymetry and keratometry in keratoconic eyes with respect to the stage of Amsler-Krumeich classificationBr J Ophthalmol20149845946324457362
- FukudaSBeheregaraySHoshiSComparison of three-dimensional optical coherence tomography and combining a rotating Scheimpflug camera with a Placido topography system for forme fruste keratoconus diagnosisBr J Ophthalmol2013971554155924081501
- KanellopoulosAJAsimellisGComparison of Placido disc and Scheimpflug image-derived topography-guided excimer laser surface normalization combined with higher fluence CXL: the Athens Protocol, in progressive keratoconusClin Ophthalmol201371385139623901251
- NaderanMShoarSNaderanMKamaleddinMARajabiMTComparison of corneal measurements in keratoconic eyes using rotating Scheimpflug camera and scanning-slit topographyInt J Ophthalmol20158227528025938040
- González-PérezJGonzález-MéijomeJMRodríguez AresMTParafitaMÁCentral corneal thickness measured with three optical devices and ultrasound pachometryEye Contact Lens201137667021301351
- ShahSLaiquzzamanMBhojwaniRMantrySCunliffeIAssessment of the biomechanical properties of the cornea with the ocular response analyzer in normal and keratoconic eyesInvest Ophthalmol Vis Sci2007483026303117591868
- ShahSLaiquzzamanMComparison of corneal biomechanics in pre and post-refractive surgery and keratoconic eyes by Ocular Response AnalyserCont Lens Anterior Eye20093212913219233712
- FontesBMAmbrósioRJardimDVelardeGCNoséWCorneal biomechanical metrics and anterior segment parameters in mild keratoconusOphthalmology201011767367920138369
- SchweitzerCRobertsCJMahmoudAMScreening of forme fruste keratoconus with the ocular response analyzerInvest Ophthalmol Vis Sci2010512403241019907025
- SchwiegerlingJGreivenkampJEKeratoconus detection based on videokeratoscopic height dataOptom Vis Sci1996737217289002087
- GobbeMGuillonMCorneal wavefront aberration measurements to detect keratoconus patientsCont Lens Anterior Eye200528576616318836
- PantanelliSMacRaeSJeongTMYoonGCharacterizing the wave aberration in eyes with keratoconus or penetrating keratoplasty using a high-dynamic range wavefront sensorOphthalmology20071142013202117553566
- BührenJKühneCKohnenTDefining subclinical keratoconus using corneal first-surface higher-order aberrationsAm J Ophthalmol200714338138917317387
- Gordon-ShaagAMillodotMIfrahRShneorEAberrations and topography in normal, keratoconus-suspect, and keratoconic eyesOptom Vis Sci20128941141822311193
- JafriBLiXYangHRabinowitzYSHigher order wavefront aberrations and topography in early and suspected keratoconusJ Refract Surg20072377478117985796
- ReddyJCRapuanoCJCaterJRSuriKNagraPKHammersmithKMComparative evaluation of dual Scheimpflug imaging parameters in keratoconus, early keratoconus, and normal eyesJ Cataract Refract Surg20144058259224680519
- BührenJKookDYoonGKohnenTDetection of subclinical kera-toconus by using corneal anterior and posterior surface aberrations and thickness spatial profilesInvest Ophthalmol Vis Sci2010513424343220164452
- BührenJKühneCKohnenTWavefront analysis for the diagnosis of subclinical keratoconusOphthalmologe200610378379016896685
- SaadAGatinelDEvaluation of total and corneal wavefront high order aberrations for the detection of forme fruste keratoconusInvest Ophthalmol Vis Sci2012532978299222427590
- JafarinasabMRFeiziSKarimianFHasanpourHEvaluation of corneal elevation in eyes with subclinical keratoconus and keratoconus using Galilei double Scheimpflug analyzerEur J Ophthalmol201323337738423335313
- UçakhanÖÖÇetinkorVÖzkanMKanpolatAEvaluation of Scheimpflug imaging parameters in subclinical keratoconus, keratoconus, and normal eyesJ Cataract Refract Surg20113761116112421596255
- The PentacamThe Gold Standard in Anterior Segment Tomography. [webpage on the Internet]OCULUS Optikgeräte GmbH2015 [cited December 12, 2015]. Available from: http://www.pentacam.com/sites/messprinzip.phpAccessed December 25, 2015