
Abstract
Background
Bevacizumab combined with chemotherapy has become the first-line therapy in advanced nonsquamous non-small-cell lung cancer (NSCLC). However, few studies have focused on cisplatin/pemetrexed with bevacizumab as the first-line therapy to treat advanced nonsquamous NSCLC. Importantly, whether the epidermal growth factor receptor (EGFR) mutations or anaplastic lymphoma kinase (ALK) rearrangements can influence the efficacy of bevacizumab in combination with chemotherapy is very interesting. Herein, we report three cases with different types of gene drives in advanced nonsquamous NSCLC.
Case presentation
In the first case, a patient presented with wild-type EGFR and negative ALK rearrangement. In the second case, a patient presented with wild-type EGFR and positive ALK rearrangement. In the third case, a patient presented with negative ALK rearrangement and mutated EGFR in exon 19.
Conclusion
We speculate that bevacizumab in combination with cisplatin/pemetrexed as the first-line therapy is well tolerated and results in a clinically meaningful treatment benefit, irrespective of the gene drive type in advanced nonsquamous NSCLC. However, more data are needed to confirm the relationship.
Introduction
Non-small-cell lung cancer (NSCLC) is one of the most common carcinomas in the world.Citation1 Patients with advanced NSCLC have a poor prognosis, with 4–6 months median progression-free survival (PFS) and 8–10 months median overall survival (OS).Citation2–Citation4 Chemotherapy is the preferred option for advanced NSCLC, and platinum-based doublet chemotherapy is the internationally recognized standard for treating advanced NSCLC.Citation5,Citation6 However, the efficacy of traditional chemotherapy has reached a plateau. With the development of molecular biology and cellular biology, targeted therapies bring hope to patients with NSCLC. Patients harboring epidermal growth factor receptor (EGFR) mutations or anaplastic lymphoma kinase (ALK) rearrangements may benefit from treatment with tyrosine kinase inhibitors or ALK inhibitors.Citation7,Citation8 In addition, bevacizumab, one of the most widely used drugs of targeted therapy, has been the first-line therapy in combination with chemotherapy in advanced nonsquamous NSCLC.Citation9 However, few studies have focused on the combination of bevacizumab with pemetrexed/cisplatin. In addition, the correlation between EGFR mutations or ALK rearrangements and the efficacy of bevacizumab in combination with chemotherapy has been problematic in clinical practice. In our study, we share three case reports. In the first case, a patient presented with no EGFR mutations and ALK rearrangements. In the second case, we present a patient who has no EGFR mutations but has ALK rearrangements. While in the third case, we present a patient who has EGFR mutations but has no ALK rearrangements.
Case reports
This study was approved by the Ethics Committee of Shandong Cancer Hospital, and all patients signed informed consent forms for procedures to be performed and the reporting of their results.
Case 1
A 69-year-old man presented to Shandong Cancer Hospital. The right lung mass was found by computed tomography (CT) scan 9 months ago, when the patient underwent a routine physical examination (). CT-guided percutaneous needle biopsy of the lung mass proved adenocarcinoma, and the gene detection showed that the EGFR was wild type and the ALK rearrangement was negative. The patient received bevacizumab (7.5 mg/kg), cisplatin (75 mg/m2), and pemetrexed (500 mg/m2) administered every 3 weeks. During the treatment, digestive tract reaction and myelotoxicity were well tolerated. Chest CT showed significant shrinkage of the primary mass after two cycles of therapy (). Interestingly, after four cycles of therapy, the lung mass showed further shrinkage, as evidenced by CT scan (). In addition, the expression of carcinoembryonic antigen was reduced progressively in the course of treatment ().
Figure 1 Case 1.
Abbreviation: CT, computed tomography.

Table 1 Clinical characteristics of different patients during the course of treatment
Case 2
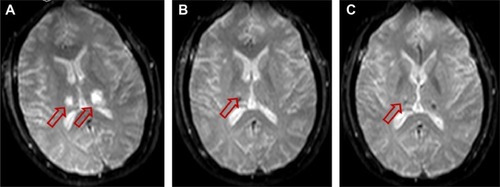
A 52-year-old woman also presented to Shandong Cancer Hospital. Multiple lung nodules and multiple brain metastases were found in the patient by CT scan and magnetic resonance imaging scan, respectively ( and ). CT-guided percutaneous needle biopsy of the mass proved adenocarcinoma, and the gene detection showed that the EGFR was wild type and the ALK rearrangement was positive. This patient also received bevacizumab (7.5 mg/kg), cisplatin (75 mg/m2), and pemetrexed (500 mg/m2) administered every 3 weeks. During the treatment, digestive tract reaction and myelotoxicity were well tolerated. Chest CT showed significant shrinkage of the major lung nodule after two cycles of therapy (). Importantly, brain magnetic resonance imaging showed that the major brain metastasis mass almost disappeared after two cycles of therapy (). Similarly, after four cycles of therapy, the major lung nodule showed further shrinkage as seen from CT scan (), and the brain metastasis mass also almost disappeared (). In addition, the expression of carcinoembryonic antigen was reduced progressively in the course of treatment ().
Figure 2 Case 2.
Abbreviation: CT, computed tomography.

Figure 3 Case 2.
Abbreviation: MRI, magnetic resonance imaging.
Case 3
A 58-year-old woman also presented to Shandong Cancer Hospital. The left lung mass was found by CT scan 3 months ago (). CT-guided percutaneous needle biopsy of the lung mass proved adenocarcinoma, and the gene detection showed that a deletion mutation in the exon 19 of the EGFR and the ALK rearrangement was negative. She also received bevacizumab (7.5 mg/kg), cisplatin (75 mg/m2), and pemetrexed (500 mg/m2) administered every 3 weeks. During the treatment, digestive tract reaction and myelotoxicity were also well tolerated. Chest CT showed significant shrinkage of the major lung nodule after two cycles of therapy (). Similarly, after four cycles of therapy, the major lung nodule showed further shrinkage as seen from CT scan (). The expression of carcinoembryonic antigen was also reduced progressively in the course of treatment ().
Figure 4 Case 3.
Abbreviation: CT, computed tomography.

Discussion
The vascular endothelial growth factor pathway is well established as one of the key regulators in tumor angiogenesis, which is a fundamental event in tumor growth and metastatic dissemination.Citation10,Citation11 Bevacizumab, a recombinant humanized IgG1 monoclonal antibody, can inhibit tumor angiogenesis and suppress tumor growth and metastasis by specifically binding with vascular endothelial growth factor, thereby blocking the biological effects of vascular endothelial growth factor.Citation12 In addition, bevacizumab can increase the concentration of chemotherapeutic drug by promoting tumor vascular stabilization, reducing tissue gap pressure, and increasing vascular permeability, thus enhancing the efficacy of chemotherapy.Citation13
At present, bevacizumab showed encouraging efficacy as the first-line therapy for patients with nonsquamous NSCLC in some studies (). The Eastern Cooperative Oncology Group 4599, a Phase III clinical study of III/IV nonsquamous NSCLC, compared the efficacy of carboplatin/paclitaxel and carboplatin/paclitaxel plus bevacizumab and showed that the median OS was extended by 2 months and the median PFS was extended by 1.7 months, respectively.Citation14 The AVAiL compared the efficacy of cisplatin/gemcitabine and cisplatin/gemcitabine plus bevacizumab for advanced NSCLC and showed that the hazard ratio for PFS was 0.75 in the low-dose group and 0.82 in the high-dose group compared with placebo, respectively.Citation15 Reynolds et al evaluated the combination of nab-paclitaxel, carboplatin, and bevacizumab in advanced (stage IIIB/IV) nonsquamous NSCLC and showed the response rate was 31% with a stable disease rate of 54%. The median PFS was 9.8 months, and the median OS was 16.8 months.Citation16 The SAiL study, an open-label, single-group, Phase IV study from centers in 40 countries, assessed the safety and efficacy of first-line bevacizumab combined with standard chemotherapy regimens in clinical practice and confirmed the manageable safety profile of first-line bevacizumab in combination with various standard chemotherapy regimens for the treatment of advanced nonsquamous NSCLC.Citation17 Interestingly, these studies considered mainly White patients as the research subjects. In fact, bevacizumab was also efficacious in Asian populations by subgroup analyses of the AVAiL and SAiL studies. In addition, the randomized Phase II JO19907 study compared the efficacy and safety of first-line carboplatin/paclitaxel alone with carboplatin/paclitaxel plus bevacizumab in Japanese patients with advanced nonsquamous NSCLC. The results showed that the hazard ratio for PFS was 0.61 with carboplatin/paclitaxel plus bevacizumab versus carboplatin/paclitaxel alone.Citation18 Importantly, the Phase III BEYOND trial was undertaken to confirm the efficacy of first-line bevacizumab plus platinum doublet chemotherapy in a Chinese patient population, and the results showed that the PFS was prolonged by 2.7 months and the OS was also prolonged by 6.6 months in patients with carboplatin/paclitaxel plus bevacizumab versus carboplatin/paclitaxel plus placebo.Citation19 After reviewing the earlier research, we can find that bevacizumab combined with chemotherapy has been used as the first-line therapy status for advanced nonsquamous lung cancer. However, two problems should be paid attention. First, bevacizumab can prolong survival only in combination with paclitaxel, and the survival benefits to patients were not found in combination with gemcitabine. This can be attributed to the fact that paclitaxel can trigger inflammation in the body, thus promoting the formation of tumor blood vessels.Citation20,Citation21 Interestingly, bevacizumab, an antiangiogenic drug, not only can reverse these negative factors but also can augment the treatment effect of paclitaxel. Second, pemetrexed, an effective therapeutic agent in the treatment of NSCLC, is a novel metabolic antagonist capable of inhibiting multiple enzymes involved in folate metabolism. At present, cisplatin plus pemetrexed therapy has been used as a standard therapeutic strategy for patients with advanced nonsquamous NSCLC.Citation22 However, few studies have focused on cisplatin/pemetrexed with bevacizumab as the first-line therapy to treat advanced nonsquamous NSCLC. Similar studies have been analyzed, and we found the application of combination of pemetrexed/oxaliplatin and bevacizumab in patients with stage IV NSCLC and showed that the objective response rate was 55.3%. The median PFS and OS were 6.2 months and 14.6 months, respectively.Citation23 However, in this study, the application of bevacizumab is combined with oxaliplatin and not with cisplatin. In addition, Barlesi et alCitation24 demonstrated that in patients with nonsquamous NSCLC who had achieved disease control with platinum-based chemotherapy plus bevacizumab, bevacizumab plus pemetrexed maintenance was associated with a significant PFS benefit compared with bevacizumab alone. However, the study was not from the People’s Republic of China, and the study did not carry out subgroup analysis according to different gene mutation types. Hirai et alCitation25 also retrospectively evaluated the feasibility of cisplatin/pemetrexed/bevacizumab therapy as a first-line chemotherapeutic strategy for patients with advanced nonsquamous NSCLC and clarified the effectiveness and tolerability of cisplatin/pemetrexed/bevacizumab therapy in patients with nonsquamous NSCLC. However, the study was also not from the People’s Republic of China, and the dose of bevacizumab was 15 mg/kg in this study. In our study, we mainly proved the effectiveness of cisplatin/pemetrexed/bevacizumab therapy in Chinese patients with nonsquamous NSCLC, irrespective of the gene drive type. In addition, the dose of bevacizumab that all the patients received was 7.5 mg/kg in our study. However, these are just a few case reports, and it requires a larger, randomized controlled trial to verify.
Table 2 Randomized controlled trials of bevacizumab plus chemotherapy
The discovery of EGFR mutations or ALK rearrangements has led to altered treatments for patients with NSCLC who harbor these drivers. Agents that inhibit the tyrosine kinase-binding sites have demonstrated improved PFS versus chemotherapy. However, the correlation between EGFR mutations or ALK rearrangements and the efficacy of bevacizumab in combination with chemotherapy warrants further analysis. The BEYOND trial showed the significance of high EGFR tyrosine kinase inhibitor in both arms after progression, but overall postprogression treatments were balanced in the EGFR mutation-positive group. EGFR mutation-positive tumor status seemed to be prognostic for a better prognosis regardless of treatment. The median PFS was 12.4 months with carboplatin/paclitaxel plus bevacizumab and 7.9 months with carboplatin/paclitaxel plus placebo in EGFR mutation-positive tumors and 8.3 months and 5.6 months in wild-type tumors, respectively.Citation19 Interestingly, another study showed that ALK-positive patients had a significantly longer PFS on pemetrexed compared with EGFR or KRAS mutant patients in NSCLC. This conclusion suggested that pemetrexed should be preferentially considered for the treatment of ALK-positive lung adenocarcinoma.Citation26 In our study, we chose three patients with different types of gene drives and found that the disease in the three patients was controlled. However, we also found the disease remission of the first patient is relatively slow compared to the other two patients. This phenomenon may be due to different driving genes. Of course, more clinical studies are needed for further clarification.
There are still some limitations in our report. First, at present, the patients in our report are still in the maintenance therapy, and the exact PFS or OS was not observed due to a short span of time. Second, in our report, we mainly evaluated the changes of the main mass in the lung. In fact, different degrees of lymph node metastasis were found in the three patients before treatment, and all these lymph node metastases get relieved to some extent after treatment.
Conclusion
In summary, based on the three cases and previous studies, cisplatin/pemetrexed/bevacizumab therapy can serve as a primary therapeutic strategy for patients with advanced nonsquamous NSCLC and with or without EGFR mutations or ALK rearrangements. More clinical studies are needed to further validate our hypothesis.
Acknowledgments
This work was supported by the special fund for Scientific Research in Public Interest (201402011).
Disclosure
The authors report no conflicts of interest in this work.
References
- JemalABrayFCenterMMFerlayJWardEFormanDGlobal cancer statisticsCA Cancer J Clin2011612699021296855
- LiuKJGuanZZLiangYA double-blind, randomized phase II study of dicycloplatin plus paclitaxel versus carboplatin plus paclitaxel as first-line therapy for patients with advanced non-small-cell lung cancersArch Med Sci201410471772425276156
- StinchcombeTESocinskiMACurrent treatments for advanced stage non-small cell lung cancerProc Am Thorac Soc20096223324119349493
- HottaKMatsuoKUeokaHKiuraKTabataMTanimotoMAddition of platinum compounds to a new agent in patients with advanced non-small-cell lung cancer: a literature based meta-analysis of randomised trialsAnn Oncol200415121782178915550583
- SchillerJHHarringtonDBelaniCPComparison of four chemotherapy regimens for advanced non-small-cell lung cancerN Engl J Med20023462929811784875
- OheYOhashiYKubotaKRandomized phase III study of cisplatin plus irinotecan versus carboplatin plus paclitaxel, cisplatin plus gemcitabine and cisplatin plus vinorelbine for advanced non-small-cell lung cancer: Four-Arm Cooperative Study in JapanAnn Oncol200718231732317079694
- Perez-SolerRChachouaAHammondLADeterminants of tumor response and survival with erlotinib in patients with non-small-cell lung cancerJ Clin Oncol200422163238324715310767
- KrisMGNataleRBHerbstRSEfficacy of gefitinib, an inhibitor of the epidermal growth factor receptor tyrosine kinase, in symptomatic patients with non-small cell lung cancer: a randomized trialJAMA2003290162149215814570950
- CohenMHGootenbergJKeeganPPazdurRFDA drug approval summary: bevacizumab (Avastin) plus Carboplatin and Paclitaxel as first-line treatment of advanced/metastatic recurrent nonsquamous non-small cell lung cancerOncologist200712671371817602060
- FerraraNRole of vascular endothelial growth factor in physiologic and pathologic angiogenesis: therapeutic implicationsSemin Oncol200229suppl 16101412516033
- BergersGBenjaminLETumorigenesis and the angiogenic switchNat Rev Cancer20033640141012778130
- Jenab-WolcottJGiantonioBJBevacizumab. current indications and future development for management of solid tumorsExpert Opin Biol Ther20099450751719344286
- WillettGGBoucherYdi TomasoEDirect evidence that the VEGF-specific antibody bevacizumab has antivascular effects in human rectal cancerNat Med200410214514714745444
- SandlerAGrayRPerryMCPaclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancerN Engl J Med2006355242542255017167137
- ReckMvon PawelJZatloukalPPhase III trial of cisplatin plus gemcitabine with either placebo or bevacizumab as first-line therapy for nonsquamous non-small-cell lung cancer: AVAilJ Clin Oncol20092781227123419188680
- ReynoldsCBarreraDJotteRPhase II trial of nanoparticle albumin-bound paclitaxel, carboplatin, and bevacizumab in first-line patients with advanced nonsquamous non-small cell lung cancerJ Thorac Oncol20094121537154319887966
- CrinòLDansinEGarridoPSafety and efficacy of first-line bevacizumab-based therapy in advanced non-squamous non-small-cell lung cancer (SAiL, MO19390): a phase 4 studyLancet Oncol201011873374020650686
- NihoSKunitohHNokiharaHRandomized phase II study of first-line carboplatin-paclitaxel with or without bevacizumab in Japanese patients with advanced non squamous non-small-cell lung cancer. JO19907 Study GroupLung Cancer201276336236722244743
- ZhouCWuYLChenGBEYOND: a randomized, double-blind, placebo-controlled, multicenter, phase III study of first-line carboplatin/paclitaxel plus bevacizumab or placebo in Chinese patients with advanced or recurrent nonsquamous non-small-cell lung cancerJ Clin Oncol201533192197220426014294
- RoodhartJMHeHDaenenLGNotch1 regulates angio-supportive bone marrow-derived cells in mice: relevance to chemoresistanceBlood2013122114315323690447
- Volk-DraperLHallKGriggsCPaclitaxel therapy promotes breast cancer metastasis in a TLR4-dependent mannerCancer Res201474195421543425274031
- ScagliottiGVParikhPvon PawelJPhase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancerJ Clin Oncol200826213543355118506025
- MirOBoudou-RouquettePGirouxJPemetrexed, oxaliplatin and bevacizumab as first-line treatment in patients with stage IV non-small cell lung cancerLung Cancer201277110410922364783
- BarlesiFScherpereelARittmeyerARandomized phase III trial of maintenance bevacizumab with or without pemetrexed after first-line induction with bevacizumab, cisplatin, and pemetrexed in advanced nonsquamous non-small-cell lung cancer: AVAPERL (MO22089)J Clin Oncol201331243004301123835708
- HiraiFSetoTInamasuEFeasibility of cisplatin/pemetrexed with 15 mg/kg bevacizumab for the treatment of patients with advanced non-squamous non-small cell lung cancerOncol Lett2015962577258226137109
- CamidgeDRKonoSALuXAnaplastic lymphoma kinase gene rearrangements in non-small cell lung cancer are associated with prolonged progression-free survival on pemetrexedJ Thorac Oncol20116477478021336183